
Abstract
Abstract
Background:
Sequential liver–kidney transplantation (SeqLKT) from the same living donor has shown excellent results in children with primary hyperoxaluria type 1 (PH1), yet its experience is limited due to the invasiveness of two major procedures for liver–kidney procurement in a single donor. Despite laparoscopic nephrectomy and hepatic left lateral sectionectomy (LLS) being considered standard procedures in living donation, the sequential use of the two laparoscopic approaches in the same living donor has never been reported.
Methods:
Herein, we present the first two case series of laparoscopic liver–kidney procurement in the same living donor for SeqLKT in children with PH1 and review of the current literature on this topic.
Results:
In the first case, a 15-month-old boy received a SeqLKT from his 32-year-old mother, who underwent a laparoscopic LLS and, after 8 months, a laparoscopic left nephrectomy. In the second case, a 34-month-old boy received a SeqLKT from his 40-year-old father who underwent laparoscopic LLS followed by hand-assisted right nephrectomy after 4 months. Both donors had uneventful postoperative courses and were discharged within 5 days from each surgery. The first recipient had no complication; the second child after liver transplantation developed a partial thrombosis of the inferior vena cava, which did not preclude the sequential kidney transplantation. After 12 months, donors and recipients displayed normal liver and renal functions.
Conclusions:
Sequential laparoscopic liver–kidney procurement in the same living donor is safe and feasible, and might be considered as a possible strategy to promote SeqLKT in children with PH1 from the same living donor.
Introduction
Primary hyperoxaluria type 1 (PH1) is a rare autosomal recessive metabolic disorder caused by a deficiency of the liver enzyme alanine-glyoxylate aminotransferase, resulting in increased hepatic oxalate production. The excess of oxalate causes progressive end-stage renal disease (ESRD) and systemic oxalosis, leading to severe morbidity and mortality. 1
Combined liver–kidney transplantation (CLKT) is considered the treatment of choice in patients affected by PH1 with ESRD. 1 Liver transplantation (LT) may be simultaneous or sequential with kidney transplantation (KT) depending on disease staging, renal function, and type of donor availability. 2 Initially, simultaneous or sequential CLKT has been mainly performed using organs from deceased donors. 3 Because of organ shortage, sequential liver–kidney transplantation (SeqLKT) from the same living donor has been proposed in PH1 patients, showing biochemical and immunological advantages for the recipient. 4 Yet, the experience of SeqLKT from the same living donor is limited due to the complexity of the donor surgical procedures.5–12
Although in living donation the laparoscopic left lateral sectionectomy (LLS)13,14 and nephrectomy15,16 showed good donor and recipient outcomes, the laparoscopic sequential liver–kidney procurement has never been reported.
To the best of our knowledge, we report the first two cases of sequential laparoscopic liver–kidney procurement from the same living donor for SeqLKT in children with PH1. The literature of living-related SeqLKT for PH1 patients has been systematically reviewed.
Center Experience
Case 1
A 15-month-old boy (weight: 8 kg; height: 74 cm) with genetically confirmed PH1 and ESRD was referred for CLKT. At presentation, the patient was on peritoneal dialysis with secondary hyperparathyroidism, hyperphosphatemia, and anemia. Serum oxalates were 128 μmol/L and hemodialysis was started (in addition to nocturnal peritoneal dialysis) to reduce his level. The family was offered the option of a living-related SeqLKT, and the 32-year-old mother (weight: 67 kg; body mass index [BMI]: 23.5) expressed her willingness to donate. Her evaluation revealed no physical or psychological contraindications for living donation. Computed tomography (CT) and three-dimensional reconstruction were used to define the donor anatomy and the expected liver graft volume (Fig. 1). Liver vascular anatomy consisted in an aberrant left hepatic artery (HA) arising from the left gastric artery and a right HA from the proper HA, while the left portal vein (PV), the hepatic veins (HVs), and biliary tree had standard anatomy. The expected left lateral segment (SII–SIII) volume was 243 gr (graft-to-recipient weight ratio [GRWR]: 3%). At the CT, the left kidney had conventional anatomy (one renal artery, one renal vein, one ureter) and was chosen for SeqLKT.

Preoperative donor imaging of the liver. Preoperative donor's CT scan showing the volumetry of
First, in the donor full laparoscopic LLS was carried out as described by Soubrane et al. 17 The patient was placed in supine position, with her legs apart to apply the French position. The pneumoperitoneum was established at 12 mmHg and five trocars were inserted (Fig. 2A). Within the lesser omentum, the left HA was isolated. The round ligament was dissected and all the branches for segment IV were divided, exposing the left PV. After the sectioning of the Arantius ligament, the left HV was encircled extra-parenchymally. To obtain a modified “hanging maneuver,” an umbilical tape was placed between the left HV and the middle HV, and passed over the left PV and left HA. Dissection of the parenchyma was then performed to the right of the falciform ligament, using bipolar forceps, clips, sutures, and sealing devices, without Pringle maneuver. To preserve vascularization of the left bile duct, the hilar plate was sharply divided at the level of the Rex recessus, and the stump of the bile duct of the donor's remnant liver was closed with sutures. When the parenchymal transection was completed, the left HA, the left PV, and the left HV were sequentially divided using mechanical staplers. A Pfannenstiel incision was used for graft extraction, and after harvesting the graft was flushed with preservation solution (Celsior) on the back table. During donor's surgery, blood transfusion was not required. The donor had an uneventful postoperative course and was discharged after 5 days.
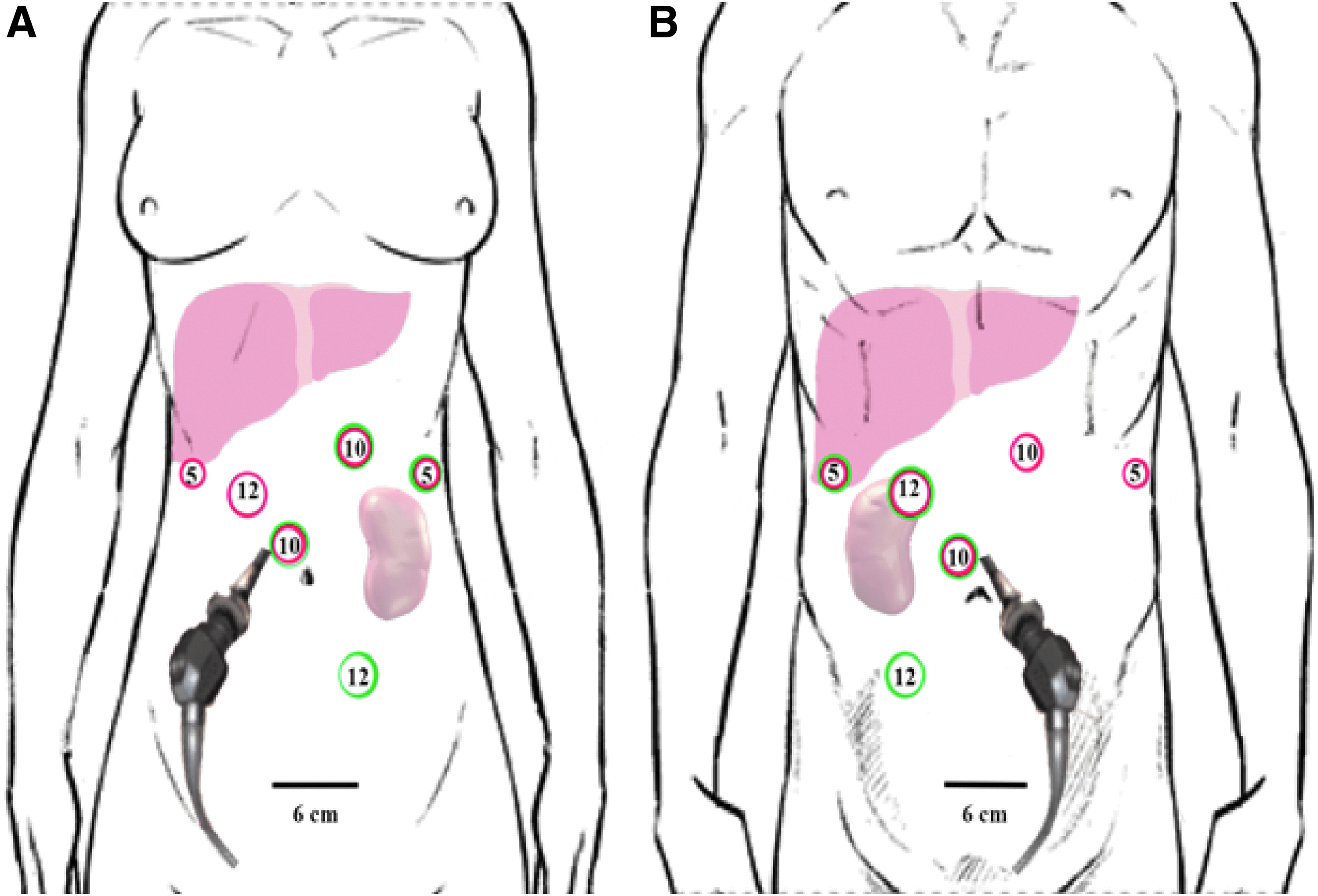
Trocar position for sequential laparoscopic left lateral sectionectomy and nephrectomy in the same living donor.
In the recipient, due to elevated preoperative oxalate levels a bilateral nephrectomy was performed. After hepatectomy with inferior vena cava (IVC) preservation, the left lateral segment was transplanted using the piggy-back technique. 18 After LT, liver function tests gradually normalized and hemodialysis was continued (six times/week). Recipient's postoperative course was characterized by chronic thrombocytopenia and anemia, and two spontaneous bone fractures, which required a delay of KT until complete recovery.
After 8 months, the oxalate plasma level decreased to 50 μmol/L, and the living-related KT was carried out. In the donor, four trocars were inserted [three trocars using the same incision previously performed for LLS, one additional 12-mm trocar placed in the inferior left iliac fossa (Fig. 2A)]. At abdominal exploration, no adhesions were found, and a full laparoscopic left nephrectomy was performed as described by Ratner et al. 19 The pre-existing Pfannenstiel incision was used for kidney extraction. The mother had an uneventful postoperative course and was discharged after 5 days. In the recipient, KT was performed without complications. Hemodialysis was continued for the first 10 days postsurgery to ensure complete removal of oxalate and stopped thereafter. After 12 months, the recipient had normal liver and renal functions (Fig. 3); the donor is currently in good condition with normal biochemical tests (creatinine: 0.8 mg/dL; aspartate aminotransferase [AST]: 23 IU/L; total bilirubin: 0.4 mg/dL).
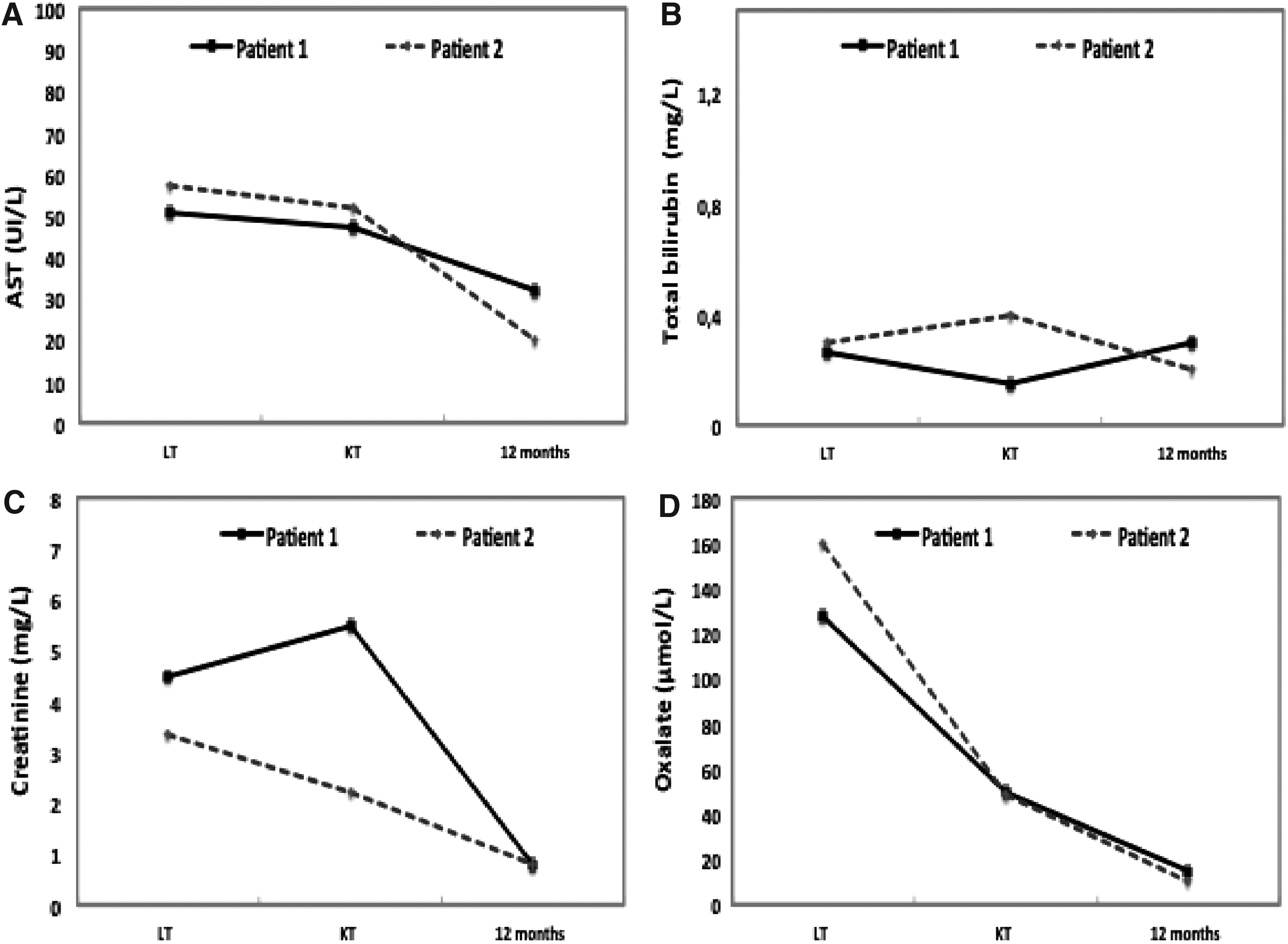
Recipients' liver–kidney functions
Case 2
A 34-month-old boy (weight: 11 kg; height: 86 cm) affected by genetically confirmed PH1 and ESRD, on peritoneal dialysis since the age of 2 months, was referred for CLKT. During the pretransplant investigation, the CT showed a thrombosis of the right iliac vein, but a patent left iliac vein. Oxalate plasma level was 160 μmol/L, and hemodialysis was started to maximize its removal. The 40-year-old father (weight: 67 kg; BMI: 24) proposed himself as a candidate donor and, after multidisciplinary evaluation, he was defined physically and psychologically suitable to donate. The father's CT showed a conventional liver anatomy and an estimated left lateral segment of 328 gr (GRWR: 2.9%); three renal arteries and one renal vein were detected in the left kidney, while single renal artery and vein in the right kidney, which was chosen for SeqLKT.
The donor liver surgery consisted in laparoscopic LLS without Pringle maneuver and blood transfusion requirement as described in Case 1 (to identify the left HA arising from the proper HA, the left side of the hepatic pedicle was dissected). Trocar positions are detailed in Figure 2B. The donor had an uneventful postoperative course and was discharged 5 days after surgery. In the recipient, after bilateral nephrectomy the left lateral segment was transplanted as defined in Case 1. After LT, a rapid normalization of liver function tests was observed, while hemodialysis was continued six times/week. Two months from surgery the child developed ascites. The angio-CT and cavography showed normal suprahepatic outflow, but thrombosis of the retrohepatic IVC; the left iliac vein and subhepatic IVC outflows were passing through the lumbar veins into the azigos vein (Fig. 4). Anticoagulants and diuretics were started, with a progressive resolution of the ascites.
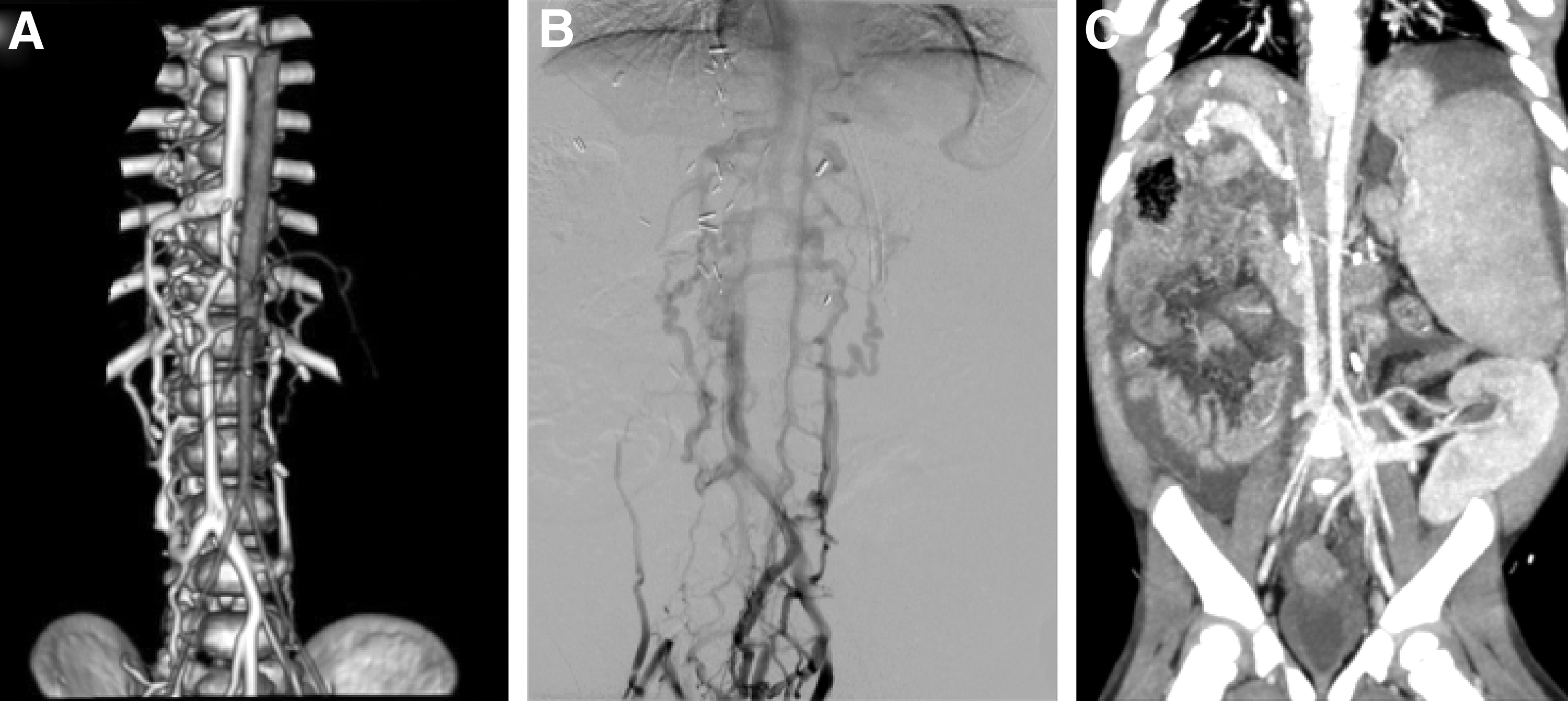
Case 2 angio-CT scan and cavography. Case 2 recipient's
After 4 months from LT, serum oxalate level was 49 μmol/L and KT was planned. The father underwent a right-hand-assisted nephrectomy with standard technique, 20 for which three trocar incisions previously performed for the LLS were used, and one 12-mm trocar incision was added in the inferior right iliac fossa (Fig. 2B). The pre-existing Pfannenstiel incision was used for the hand insertion and graft extraction. The donor postnephrectomy course was uneventful, and the patient was discharged after 4 days. In the recipient, KT was successfully performed in the left iliac fossa, and stable liver and renal functions were maintained throughout the entire follow-up (Fig. 3). After 12 months from surgery, the donor is in good clinical condition, with normal biochemical tests (creatinine: 1.1 mg/dL; AST: 35 U/L; total bilirubin: 0.7 mg/dL).
Discussion
In children, PH1 represents the principal indication (37%–61%) for CLKT, yet it is associated with inferior outcomes compared with other diseases requiring CLKT. 21 When severe systemic oxalosis is present, SeqLKT (first LT, then dialysis until sufficient oxalate clearance from the body, followed by KT) seems to be preferable compared with simultaneous CLKT.1,22 However, the timing for KT is influenced by the recipient's oxalate pool as well as the deceased donor kidney availability. 1
In the current era of organ shortage, the living-related SeqLKT in PH1 recipients combines the advantages of a sequential procedure—which optimizes the renal function by performing the KT when stable LT function and low plasma oxalate levels are achieved—and the benefits of a living-related transplantation, reducing the KT waiting-list time and the dialysis-related complications.
So far, SeqLKT from the same living donor in PH1 recipients has been reported only in small series (Table 1).5–12 Of 23 cases described in the literature, the median recipients' age at SeqLKT was 6 (1–41) years and the majority of recipients (74%) received a left lateral segment graft. Mor et al. reported that SeqLKT from the same living donor could be safely performed also in young adults with PH1 using a right liver lobe graft. 9 The interval between LT and KT was ∼6 (1–10.6) months, during which period dialysis was performed according to center's protocol (usually two to three times/week). Postoperative recipients' complications included bleeding (n = 2), cytomegalovirus infection (n = 3) and bile leak (n = 1) and biliary sepsis (n = 1). After a follow-up of 2.3 (0.2–19.7) years, the overall recipient patient survival was 88.5%, while liver and kidney graft survivals were 88.5% and 90.5% (two KT lost for rejection), respectively, which appears superior to those reported in pediatric CLKT from deceased donors (2-year survivals: 72.4% patient survival; 60.3% liver graft survival; 55.2% renal graft survival). 21
Reported Experience of Sequential Liver and Kidney Transplantation from the Same Living Donor in Patients with Primary Hyperoxaluria Type 1
CMV, cytomegalovirus; KT, kidney transplantation; LLH, left lobe hepatectomy; LLS, left lateral segmentectomy; LN, left nephrectomy; LT, liver transplantation; n.a., not available; RLH, right lobe hepatectomy; RN, right nephrectomy.
On the donor side, no mortality and morbidity were reported after sequential liver–kidney procurements in the same living donor, except for one patient who developed an abdominal fluid collection after liver resection, resolved by percutaneous drainage. All donors had a rapid postoperative recovery, and showed normal liver and renal function tests in the long term (range: 2.7 months–19.7 years).5–12
Despite these promising results, the number of SeqLKT from the same living donor is limited, most likely because of the invasiveness of the two donor surgeries using the open technique and the lack of guidelines recommending this procedure.
In the last two decades, the laparoscopic hand-assisted or pure laparoscopic nephrectomies have been established as the gold standard, being preferred to the open procedure due to less postoperative pain, shorter hospital stay, and earlier return to normal activities.15,16,23,24
Also for living liver donation, a laparoscopic approach to partial hepatectomy showed advantages over the open technique in terms of intraoperative blood losses, postoperative recovery, and abdominal wall complications.13,14 According to recent consensus guidelines, donor laparoscopic LLS for adult-to-child LT may be regarded as standard procedures, but it is still limited to few highly specialized centers.25,26 Recently, the feasibility of the combination of the two laparoscopic techniques in the same living donor was described by Gautier et al. for simultaneous CLKT. 27
Of 227 pediatric LTs performed at our center between September 2008 and December 2018, 12 (5.3%) children underwent CLKT for PH1 (five simultaneous CLKT [one from living donor], seven SeqLKT [four from living donor]). Following a 15-year learning curve in laparoscopic living donation, we adopted the laparoscopic approach for both liver and kidney procurements in the last two cases, which represent the first series of sequential laparoscopic LLS and nephrectomy in the same living donor.
In our experience, the sequential laparoscopic liver–kidney procurement in the same donor was safe and feasible, providing several advantages: on the donor side, it combined the benefits of the two laparoscopic procedures (when performed separately) maintaining the surgical risks independent for each operation; on the recipient side, the sequential procedures permitted to optimize the KT timing according to recipients' needs. Moreover, the donor LLS was associated with a rapid postoperative recovery without significant psychological/physical trauma (which would reduce the will to undergo a second operation) and permitted to reuse the same surgical incisions for the kidney procurement offering good esthetic results.
In the two PH1 recipients, liver and kidney functions rapidly recovered after transplantation, providing evidence that the laparoscopic donor procedures had no impact on graft outcomes. In the second case, the recipient developed IVC thrombosis after LT, which could be related to the pre-existing right iliac vein thrombosis and/or to the bilateral native nephrectomies performed after the hepatectomy. As proposed in other series,28,29 in our recipients the bilateral nephrectomy at the time of LT was performed to remove the significant stores of oxalate contained in the native kidneys, which may cause damage to the newly transplanted renal graft.
In our experience, the living donor laparoscopic sequential liver–kidney procurement might be proposed in well-selected cases, requiring (i) a robust indication for SeqLKT in PH1 recipients (according to clinical status, age, and oxalate levels); (ii) meticulous living-related donor assessment (age ≤55 years, BMI <30, absence of active infections/malignancies/systemic diseases, glomerular filtration rate ≥70–80 mL/min/1.73 m2, definition of liver/kidney anatomy and liver volume, psychological evaluation); and (iii) adequate donor–recipient matching (ABO compatibility, liver GRWR between 1.5 and 3). Yet, the laparoscopic living donor approach for SeqLKT has limitations related to the surgical technical complexity, which requires sufficient learning curve in mini-invasive liver–kidney procurement, and to the exposure of the same living donor to two major surgeries. So far, donor hepatectomy has imposed 0.1%–0.2% mortality and 25%–35% morbidity (mainly biliary leak) on healthy individuals, 30 while donor nephrectomy has shown <0.03% mortality and 10%–20% morbidity (major complication <3%). 31 Therefore, the potential living donor for SeqLKT has to be adequately informed of the risks for each surgical procedure.
Although additional experiences are needed, the two cases described herein suggest that sequential laparoscopic LLS and nephrectomy in the same living donor are safe and feasible, and could be considered as a preferential strategy to promote living-related SeqLKT in children affected by PH1.
Patient Consent
Informed consent was obtained from the patient for publication of their information.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.