
Abstract
Abstract
Purpose:
This study aims to ascertain the relative outcomes in patients with hilar cholangiocarcinoma (HCCA) undergoing either unilateral or bilateral self-expanded metallic stent (SEMS) insertion.
Materials and Methods:
In this retrospective single-center study, 93 patients with HCCA were treated through percutaneous insertion of either unilateral or bilateral SEMS during January 2012 to December 2018. We compared technical success, clinical success, and long-term outcomes of the treatment method.
Results:
Overall, 51 and 42 patients were treated through unilateral and bilateral SEMS insertion, respectively, with technical success rates of 92.2% (47/51) and 95.3% (40/42), respectively, (P = .859). No patients experienced any procedure-related complications, with unilateral and bilateral clinical success rates of 95.7% (45/47) and 97.4% (38/39), respectively, (P = 1.000) and with comparable adverse event rates between these groups (3/47 vs. 5/40; P = .541). Moreover, 8 and 3 patients treated with unilateral and bilateral stents exhibited stent dysfunction, respectively, (P = .183). In unilateral and bilateral groups, median patency rates were189 and 198 days, respectively, (P = .887). During the follow-up period, all patients died, with respective mean overall survival rates of 222 and 202 days for those treated using unilateral and bilateral stents (P = .755). Both Bismuth type III HCCA (P = .025) and a lack of chemotherapy (P = .000) correlated with reduced survival in univariate and multivariate regression analyses.
Conclusion:
Insertion of unilateral and bilateral SEMS exhibits similar clinical efficacy and long-term outcomes in patients with HCCA.
Introduction
Typically, malignant hilar biliary obstruction (MHBO) is caused by either malignant growths in the hilar lymph nodes or in the hepatobiliary system.1–7 Resective surgery is often not an option for patients with MHBO after the diagnosis, as the disease is mostly detected at a late stage, rendering only palliative treatment is feasible.1–7
Reportedly, self-expanded metallic stents (SEMS) can be inserted as a primary treatment option for alleviating MHBO symptoms.1–6 However, whether unilateral or bilateral stenting is preferable for treating MHBO remains unclear. Previous studies comparing the treatment approaches already mentioned have been limited because most studies examined patients with multiple tumor types, thereby potentially introducing a selection bias into their analyses.1,4–6 Thus, comparing these two stent types in patients with a single type of cancer is imperative.
Hence, this study aims to compare the clinical efficacy of unilateral and bilateral SEMS inserted to treat patients with hilar cholangiocarcinoma (HCCA).
Materials and Methods
This single-center retrospective study was approved by our institutional review board, which waived the need for obtaining written consent because of the retrospective study design.
Patients
Between January 2012 and December 2018, 93 patients with HCCA were treated through percutaneous SEMS insertion at our hospital, with 51 patients treated through unilateral SEMS insertion (January 2012–December 2014) and 42 through bilateral SEMS insertion (January 2015–December 2018) (Fig. 1). Before December 2014, we did not master the technique of bilateral SEMS insertion and, therefore, we can only use the technique of unilateral SEMS insertion. From January 2015, we introduced the technique of bilateral SEMS insertion and we used this technique up to now.
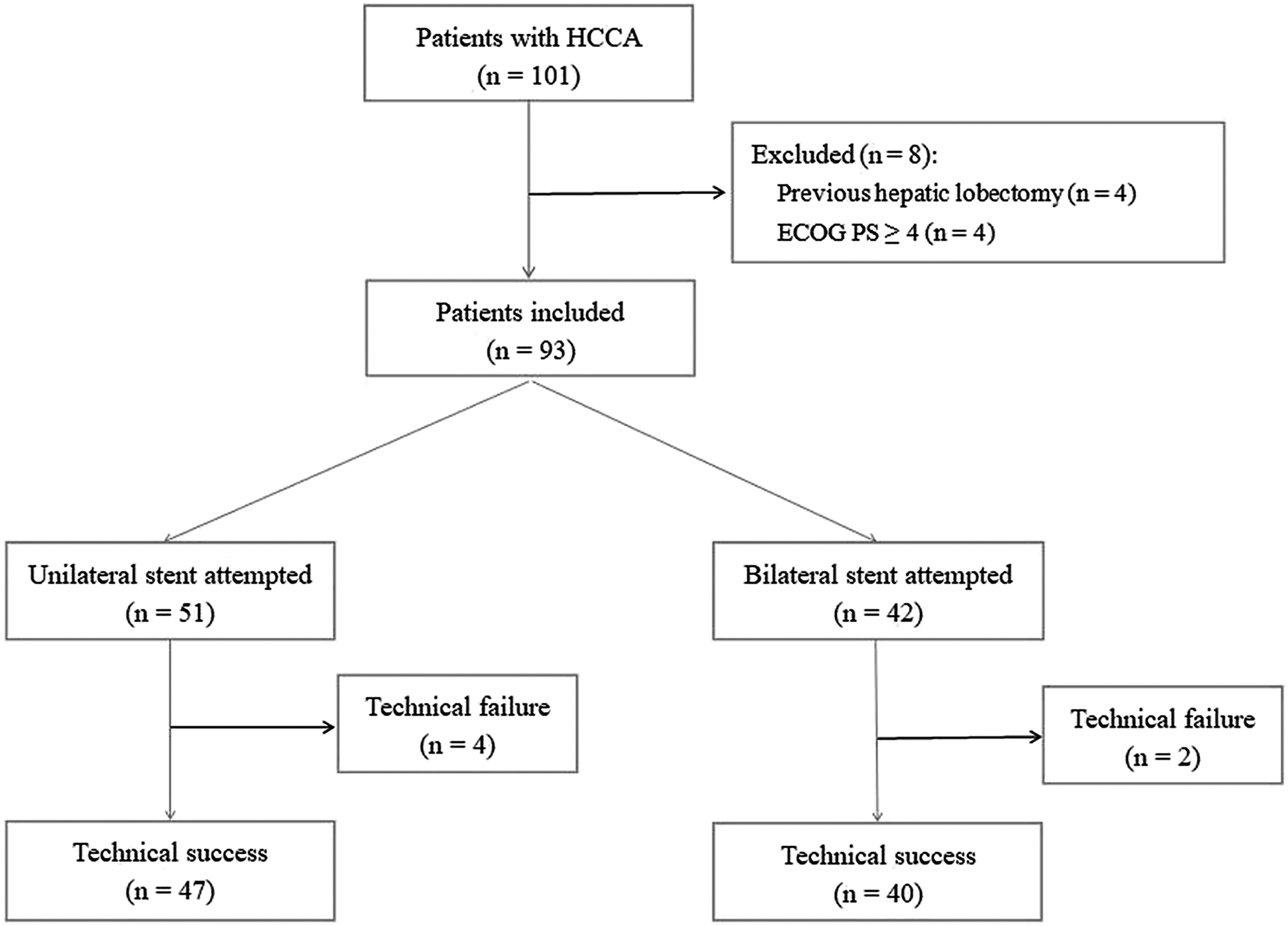
A schematic for the current study. HCCA, hilar cholangiocarcinoma.
The inclusion criteria in this study were as follows: (a) a confirmed HCCA diagnosis, (b) surgical resection is not a feasible option for treating HCCA, (c) patients displayed evidence of obstructive jaundice, and (d) patients had Bismuth type ≥ II HCCA. Conversely, the exclusion criteria were as follows: (a) a history of hepatolobectomy and (b) an Eastern Cooperative Oncology Group (ECOG) performance status ≥4.
Diagnosis
HCCA was diagnosed using a combination of abdominal computed tomography (CT), magnetic resonance imaging, and percutaneous biopsy findings.
Unilateral stenting
Patients were positioned in the supine position. Then, a combination of fluoroscopic and ultrasonic guidance was used to puncture the right intrahepatic biliary tract, into which a 21-G Chiba needle (Cook, Bloomington, IN) was inserted. Next, cholangiography was performed to gauge the degree of obstruction. After that, the obstruction site was detected with either a 4F or 5F VER catheter (Cordis, Hialeah, FL) and a 0.9 mm standard guidewire (Terumo, Tokyo, Japan). After these were across the obstruction site, a 0.9 mm stiff guidewire (Cook) was inserted in the place of standard guidewire. Finally, a bare SEMS (Micro-Tech, Nanjing, China) was released at the obstruction site to cover it.
Bilateral stenting
Bilateral stent insertion was conducted using the side-by-side (SBS) technique (Fig. 2). In brief, a pair of guidewires was inserted into the left and right intrahepatic biliary tracts, with stent delivery systems individually maneuvered to the obstruction site in an SBS manner before being synchronously released.

The side-by-side bilateral stenting.
Follow-up
Patients underwent 3-day temporary drainage using an 8.5F biliary catheter (Cook), and tests of liver functionality were conducted both before and 2 weeks after inserting the stent. Abdominal CT imaging was conducted 1, 3, and 6 months after stent insertion, and then every 6 months thereafter. Patients reporting a recurrence of either jaundice or cholangitis were considered to be experiencing stent dysfunction. All patients were followed until death, and data regarding survival, adverse events, and stent patency were collected for analysis.
Definitions
Technical success was considered when stents were positioned to cross the obstruction site, enabling the contrast agent to smoothly flow through the SEMS. Clinical success was considered when total bilirubin (TBIL) levels decreased to <70% of the preoperative baseline 2 weeks after stent insertion.4,5 Duration of stent patency was defined as the interval between stent insertion and either patient death or stent dysfunction.
Statistical analysis
We used Fisher's exact test or the chi-squared tests to compare categorical variables. Continuous variables are presented as means ± standard deviation, and Student's t-tests and Mann–Whitney's U tests were used for comparisons as appropriate. Using paired t-tests, we assessed differences before and after stent insertion. In addition, patient survival and cumulative patency were evaluated using the Kaplan–Meier curves. Predictors of survival were determined using Cox regression analyses, with variables exhibiting P ≤ .1 in a univariate analysis assessed using a multivariate model. In this study, P < .05 was the significance threshold. All statistical analyses were conducted using SPSS v16.0 (SPSS, Inc., Chicago, IL).
Results
Technical success
The technical successful rates for the insertion of unilateral and bilateral SEMS were 92.2% (47/51) and 95.3% (40/42), respectively, (P = .859), with no cases of complications related to the insertion procedure. Table 1 presents the baseline data from 87 patients in whom SEMS insertion was successful. SEMSs used in this study had a diameter of 8 mm and a length of 50–70 mm. Among 6 patients in whom insertion failed, failure was attributed to an inability of the guidewire to pass through the intrahepatic biliary tracts, with these patients instead undergoing percutaneous biliary catheter drainage for treatment.
Patient Characteristics in Unilateral and Bilateral Groups
ALT, alanine aminotransferase; AST, aspartate transaminase; ECOG PS, Eastern Cooperative Oncology Group performance status; TBIL, total bilirubin.
Clinical success
Unilateral and bilateral SEMS groups exhibited clinical successful rates of 95.7% (45/47) and 97.4% (38/39), respectively, (P = 1.000, Table 2). Of note, clinical success was not assessed in 1 patient in the bilateral group, as the patient died of respiratory failure 8 days after stenting.
Comparison of Outcomes Between Unilateral and Bilateral Groups
Adverse events
The rates of adverse events were comparable between the unilateral and bilateral groups (3/47 vs. 5/40, P = .541). Patients in the unilateral group reported cholangitis (n = 2) and cholecystitis (n = 1), whereas those in the bilateral group reported cholangitis (n = 2), cholecystitis (n = 2), and liver abscess (n = 1) as adverse events. Patients experiencing cholangitis cholecystitis underwent percutaneous biliary catheter drainage and conservative treatment, respectively, whereas those with liver abscess were treated by using a percutaneous catheter to wash and drain the cavity.
Stent dysfunction
In the unilateral and bilateral groups, 8 and 3 patients experienced stent dysfunction, respectively, (P = .183, Table 2), which was attributed to either tumor in-growth (n = 9) or sludge (n = 2). Although tumor in-growth was treated by percutaneous biliary catheter drainage (n = 7) or the second round of SEMS insertion (n = 2), sludge was treated using percutaneous biliary catheter drainage.
Furthermore, both the unilateral and bilateral groups exhibited a respective 189 and 198 days of median stent patency (P = .887, Fig. 3).
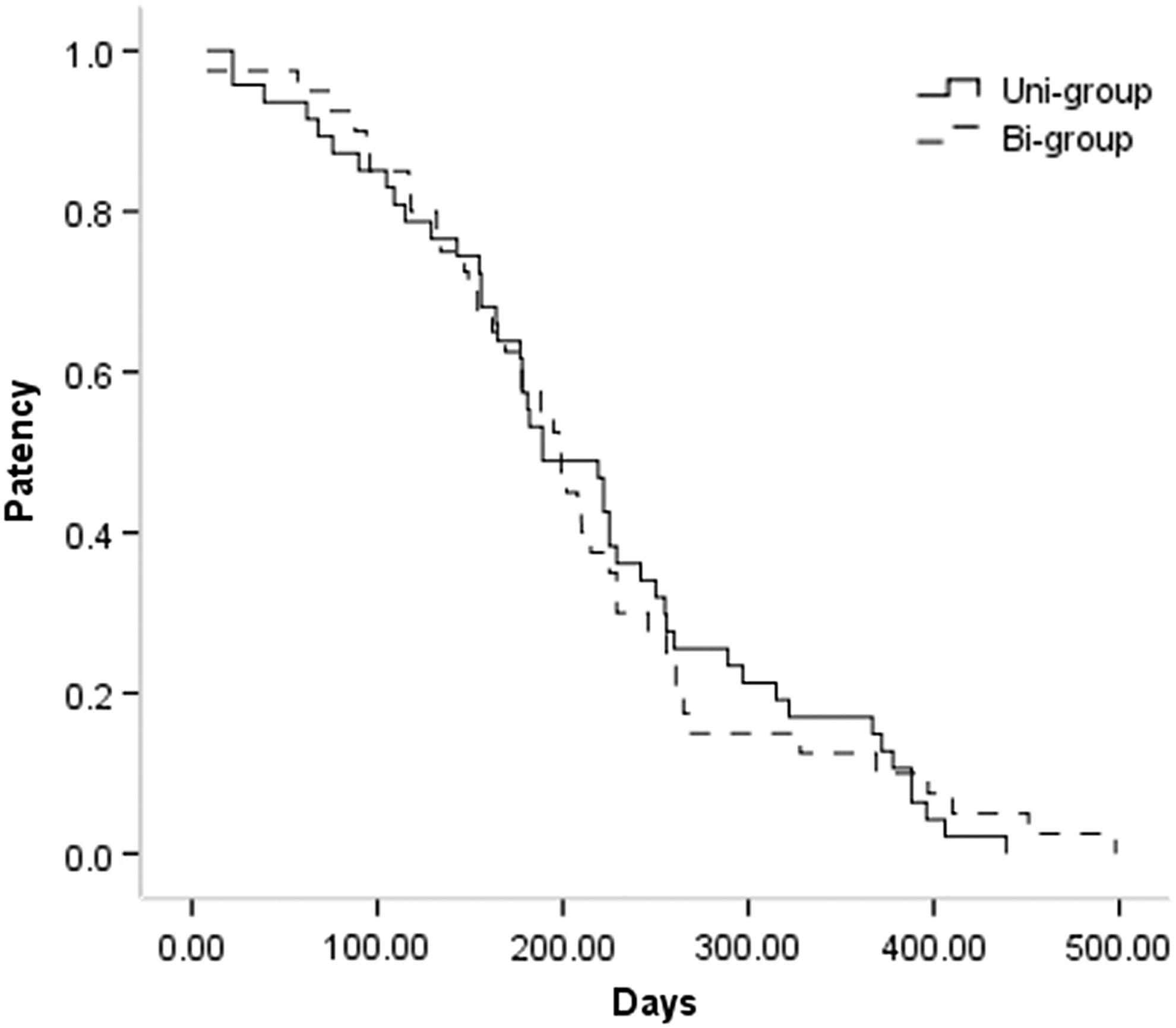
There were no significant variations in patency as shown through Kaplan–Meier curves between two groups.
Survival
All patients died during the follow-up period, with 20 and 15 patients in the unilateral and bilateral groups treated by chemotherapy (20/47 vs. 15/40, P = .632). The median overall survival periods were 222 and 202 days post-treatment, respectively, (P = .755, Fig. 4).
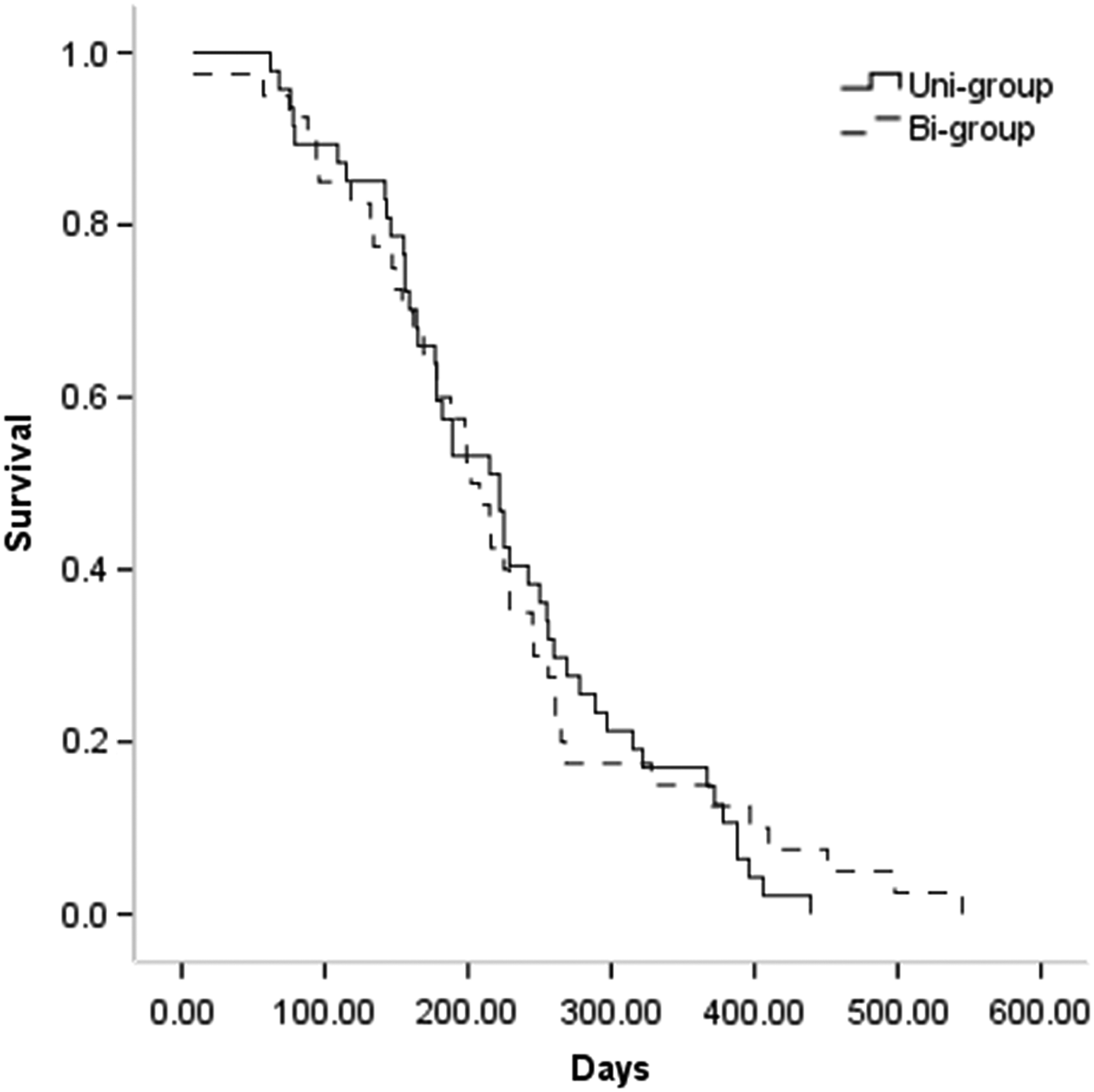
There were no significant variations in survival as shown through Kaplan–Meier curves between two groups.
The univariate Cox regression analyses identified Bismuth type III HCCA and absence of chemotherapy as predictors of poorer overall survival, whereas a multivariate analysis established that both Bismuth type III HCCA (P = .025) and the lack of chemotherapy (P = .000, Table 3) were independent predictors of poorer survival.
Univariate and Multivariate Cox Regression Analyses of Survival
CI, confidence interval.
Discussion
HCCA is the leading cause of MHBO.1–6 Currently, SEMS insertion is standard treatment for biliary obstructions, as they offer better advantages for clinical success, stent patency, and patient survival than plastic stents.8–11 However, whether MHBO and HCCA are best managed by using a unilateral or bilateral stent insertion approach remains debatable.
Unlike most previous studies considering stent insertion as a treatment option for patients with MHBO,1,2,4–7 this study solely focused on HCCA. We observed no significant differences in either technical (P = .859) or clinical (P = 1.000) success contrary to patients treated through unilateral and bilateral SEMS insertion; this finding corroborates the literature regarding treating MHBO through percutaneous stent insertion.1,4,5 Unilateral stent insertion adequately relieves MHBO-related jaundice, as TBIL levels could be normalized by facilitating the drainage of just 25%–30% of the liver. 12
Bilateral stenting as a treatment option for MHBO has been previously conducted using SBS and stent-in-stent (SIS) approaches.1–6,13,14 The SBS technique has been often preferred, as it offers dual drainage pathways in the hilar region, thereby enabling one stent to continue draining even if the other is occluded.13,14 In a comparison of unilateral and bilateral stent insertion for the treatment of MHBO, Naitoh et al. 15 reported that bilateral stenting correlated with a significant increase in the cumulative stent patency (488 vs. 210 days, P = .009), especially among patients with HCCA. However, we observed no significant difference in patency (189 vs. 198 days, P = .887) or occlusion rates (17% vs. 7.5%, P = .183) between the unilateral and bilateral groups. This difference in research findings may be attributed to the limited sample size in Naitoh et al. 15 (unilateral: 17; bilateral: 29), or the inclusion of Bismuth type I patients and a range of cancer types in this previous study.
Liberato and Canena 9 retrospectively reviewed the results from 480 patients with HCCA who underwent endoscopic stenting, revealing markedly increased patency for patients implanted with bilateral stents; however, bilateral stenting was conducted only in Bismuth type II patients, and both SIS and SBS techniques were used for insertion. Although our study examined only 87 patients, it offered some advantages as follows: (a) patients in this study were diagnosed with Bismuth type ≥ II HCCA and (b) the SBS technique was the only approach used for bilateral stent insertion.
In this study, we found survival to be comparable between the unilateral and bilateral groups (222 vs. 202 days, P = .755); consistent with this finding, prior studies have failed to detect any increase in survival related to bilateral stenting of patients with HCCA.4,9 Liberato and Canena 9 demonstrated that the use of plastic stents or SEMS did not affect HCCA patients' survival. Indeed, survival mostly depends on the tumor progression and any anticancer treatments being administered. 16 In the same line, this study found that chemotherapy prolonged survival after stent insertion, with Bismuth type III HCCA (P = .025) being an additional predictor of decreased survival. Of note, a higher Bismuth type can correspond to more advanced diseases. Although this study did not detect any link between Bismuth type IV HCCA and shorter survival, it could be attributed to the small number of Bismuth type IV HCCA patients in this study.
This study has some limitations that need to be addressed. First, this study was a retrospective study, and although a multivariate Cox regression analysis was conducted, the potential for selective bias persists. Second, this is a single-center study. Finally, as performing chemotherapy depended on patients' condition, it could have introduced further selective bias into the study results.
In conclusion, although further research is warranted to validate the findings, this study suggests that both unilateral and bilateral SEMS insertion into patients with HCCA offer similar clinical efficacy and long-term outcomes. Furthermore, chemotherapy could increase patient survival after stent insertion.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.