
Abstract
Introduction:
Minimally invasive surgical (MIS) approaches for thoracic procedures in adults result in an improved postoperative course with less pain, but there are limited data on similar procedures in neonates. We aimed to evaluate postoperative opioid consumption and pain management practices in neonates and infants following MIS versus open repair of congenital diaphragmatic hernia (CDH).
Materials and Methods:
This was an IRB approved, retrospective study from 2012 to 2016. Demographic data, intraoperative analgesic regimen, total 7-day postoperative opioid consumption, and use of adjunctive pain medications were compared by surgery type (open versus MIS). Secondary measures included time to tracheal extubation, oral feeds, and discharge home.
Results:
The study cohort included 28 patients (13 female, median age 5 days, average gestational age 39 weeks, and weight 3 kg). MIS was performed in 8 patients. In the first 7 postoperative days, the median postoperative opioid consumption was 0.3 mg/kg of oral morphine equivalents (interquartile range [IQR] 0.2, 18.3) in the MIS group versus 32.3 mg/kg (IQR 9.9, 53.6) in the open group (95% CI of differences in medians: 8.2–42.9; P = .006). No difference was noted in intraoperative opioid administration. Among secondary outcomes, length of stay was significantly longer in the open group.
Conclusions:
Although several factors may impact the hospital course of neonates with CDH, we found that patients had a more than 100-fold difference in median opioid consumption following repair with MIS versus an open approach. The study also noted significant variation in analgesic regimens suggesting other avenues for improved care of postsurgical neonates.
Introduction
Surgical repair of congenital diaphragmatic hernia (CDH) is usually performed during the neonatal period. The procedure may be performed by either a minimally invasive surgical approach (MIS) or using an open thoracotomy or abdominal approach. Although MIS has rapidly gained acceptance in adult thoracic surgery due to smaller incisions, decreased pain, faster recovery, shorter hospital stays, and superior surgical visualization, the evidence demonstrating advantages of using such techniques in neonates is limited.1–5 However, it is recognized that poorly controlled postoperative pain can have significant adverse physiologic effects on respiratory mechanics, leading to respiratory complications, including atelectasis and pneumonia, which may lead to increased morbidity, prolonged mechanical ventilation, and prolonged hospital stays.6–8
To date, only one retrospective study has examined postoperative opioid use in neonates undergoing MIS versus open thoracotomy for repair of congenital anomalies (CDH and esophageal atresia [EA]). 9 The study did not demonstrate a difference in postoperative opioid consumption for the initial 7 postsurgical days between the minimally invasive and open surgery groups. However, we postulate that the protocolized approach to postoperative pain management in that study may have limited opportunities to significantly reduce postoperative opioid consumption for patients undergoing MIS. Therefore, we sought to determine if postoperative opioid consumption was reduced among neonates undergoing minimally invasive compared to open CDH repair at our institution. Secondary outcomes included pain scores and measures of postoperative recovery, including hospital length of stay (LOS), time to tracheal extubation, need for blood transfusion, and time to oral feeding.
Materials and Methods
This retrospective study was approved by the Institutional Review Board at Nationwide Children's Hospital with a waiver of individual consent. Electronic medical records from 2012 to 2016 were queried to identify neonates who underwent minimally invasive thoracoscopic versus open surgery for CDH repair. Current Procedural Terminology codes 39503, 32666, and 32999 were used to determine the patients who underwent CDH repair either thoracoscopically or via open approach (either subcostal or thoracotomy incision). Demographic information for each patient was obtained, including date of birth, age at time of surgery, gestational age at birth, weight, gender, and American Society of Anesthesiologists (ASA) physical status.
The analgesic regimen was recorded and opioid consumption both intraoperatively and postoperatively for 7 days was calculated. Opioid consumption was converted to morphine equivalents (MEs) per kilogram (kg) of body weight for comparison between groups (Table 1).10,11 Intraoperative analgesic management was at the direction of the attending pediatric anesthesiologist for both open and MIS patients, as there was no specific anesthesia protocol in place. As part of our routine clinical care for postsurgical neonates, postoperative pain management after these procedures was also at the discretion of the attending pediatric surgeon and neonatologist. This was not protocolized for this study in the postoperative period or as part of our usual clinical care. Typically, pain management was determined based on the patient's neonatal pain, agitation, and sedation scale (N-PASS) scores, as well as the presence or absence of an endotracheal tube necessitating continuous sedation and analgesia. Postoperative use of adjunctive medications such as acetaminophen and ketorolac were recorded. For secondary outcome measures, the time to tracheal extubation, need for blood transfusion within 72 hours, pain scores, hospital LOS, and pain scores were also obtained.
Opioid Conversion Ratios Used to Calculate Total Daily Opioid Use
Continuous data were summarized using medians with interquartile range (IQR) and compared using the rank-sum tests; while categorical data were summarized using counts with percentages and compared using Chi-squared or Fisher's exact tests. Since all cases eligible for analysis were included in the study, there was no a priori power analysis. As a subanalysis of the data, we focused on comparing patients in the two groups who did not have vasopressors started preoperatively or during the case, as patients undergoing open surgery without requiring vasopressors could have been chosen as candidates for MIS and therefore represent a better-matched comparison group. In addition to account for surgical bias for an open versus MIS approach, analysis was performed on those patients who could have been MIS candidates but underwent an open procedure. MIS candidacy criteria were based on surgeon assessment, not needing a patch closure, absence of severe cardiopulmonary disease, minimal ventilatory settings, and absence of high-dose vasoactive agents and nitric oxide use. Data analysis was performed using Stata/IC 14.2 (StataCorp, LP, College Station, TX), and two-tailed P < .05 was considered statistically significant.
Results
There were 43 patients who underwent CDH repair between 2012 and 2016. Patients without intraoperative records (9 patients), those too unstable to travel to the operating room (1 patient with bedside procedure), and those who died during their hospitalization (5 patients) were excluded from the data analysis. The remaining CDH cohort included 28 patients with 13 females and 15 males. The median day at the time of surgery was 5 days, median gestational age was 39 weeks, and the median weight was 3 kg. Of these 28 patients, 8 patients underwent MIS (Table 2). There were no statistically significant differences in demographic characteristics between the two groups apart from a higher prevalence of ASA IV status in the open surgery group.
Characteristics of Patients Undergoing Open and Minimally Invasive Surgery for Congenital Diaphragmatic Hernia Repair (N = 28)
Bold values signify P < 0.05, considered statistically significant.
ASA, American Society of Anesthesiologists; IQR, interquartile range.
Postoperative study outcomes are summarized in Table 3. Intraoperative opioid use did not differ between the two groups. Among patients undergoing CDH repair, the median postoperative opioid consumption was 0.3 mg/kg of oral ME (IQR 0.2, 18.3) in the MIS group versus 32.3 mg/kg (IQR 9.9, 53.6) in the open group (95% CI of differences in medians: 8.2, 42.9; P = .006). On further analysis of postoperative pain management, only 4 of 8 patients in the MIS group had a continuous opioid infusion, compared to all 20 patients in the open group.
Postoperative Outcomes of Patients Undergoing Open and Minimally Invasive Surgery for Congenital Diaphragmatic Hernia Repair (N = 28)
IQR, interquartile range; LOS, length of stay; ME, morphine equivalent.
Postoperative nonopioid analgesic use was not different between the two groups. Acetaminophen was used postoperatively in all MIS patients and 14 of the patients in the open group (P = .141). Ketamine was used postoperatively in 4 patients in the open group and none of the patients in the MIS group (P = .295). Comparing the median acetaminophen dose between groups (Table 3), there was no significant difference between patients undergoing MIS and patients undergoing an open procedure (95% CI of difference in median dose: −22 to 103 mg/kg; P = .286).
The postoperative pain scores did not differ significantly between the two groups (Fig. 1). On postoperative day (POD) 1, both groups had a median pain score of 3 (95% CI of difference in medians: −3 to 1; P = .784). The largest difference in pain scores was seen on POD 2 (open group median = 5, MIS group median = 1), although this difference failed to reach statistical significance (95% CI of difference in medians: 0–4; P = .129) even without adjustment for multiple comparisons. Among secondary outcomes, time to tracheal extubation, oral feeds, and discharge were significantly reduced with MIS compared to open surgery for CDH repair (Table 3).
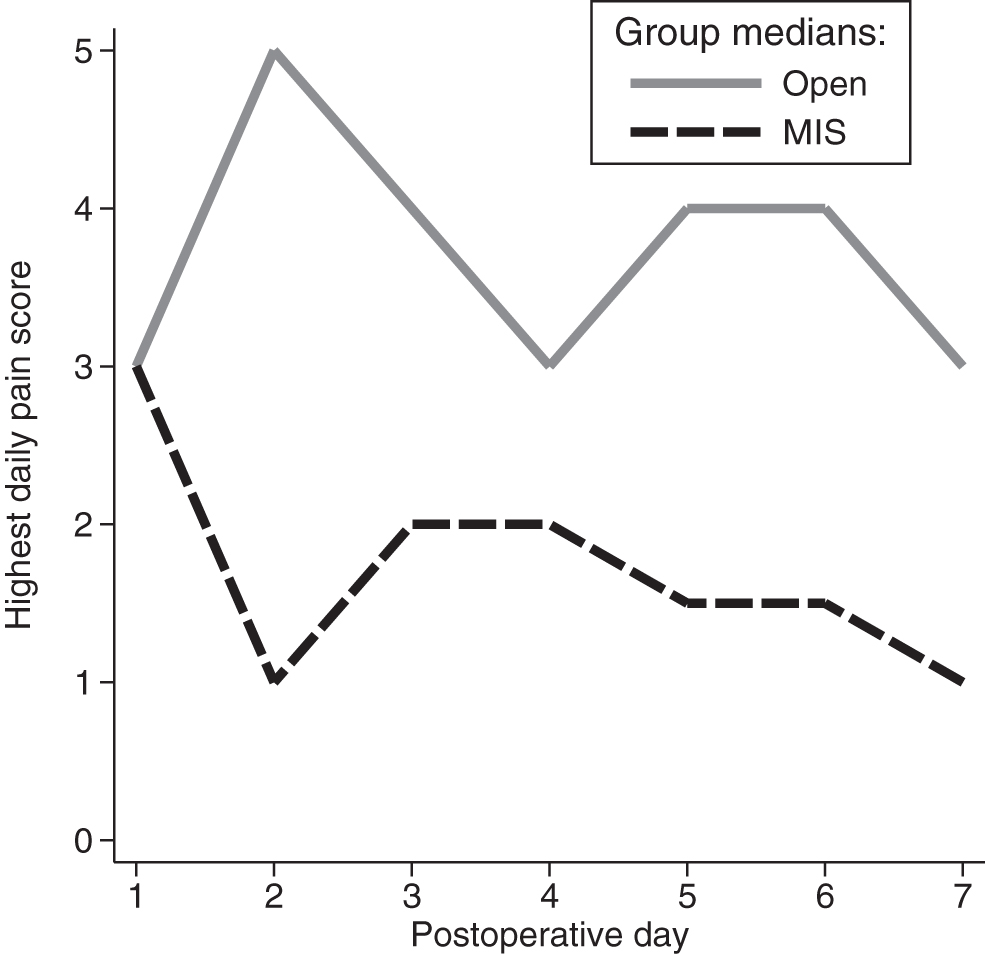
Highest daily postoperative pain scores in patients undergoing open and MIS CDH repair. CDH, congenital diaphragmatic hernia; MIS, minimally invasive surgical.
As a supplemental analysis, we reanalyzed the statistically significant outcome differences in Table 3 among 7 patients in MIS group and 7 patients in the open group who did not have vasoactive agents started before or during the procedure. This analysis confirmed a reduction in postoperative narcotic dose in the MIS group (95% CI of difference in medians: 1.4–37.6 mg/kg; P = .035), as well as reduced time to tracheal extubation (95% CI of difference in medians: 1–8 days; P = .004) and reduced time to oral feeding (95% CI of difference in medians: 1–7 days; P = .009). The reduced LOS in the MIS group did not reach statistical significance on this subanalysis (P = .063).
There were 3 patients who were identified as MIS candidates based on MIS criteria, but underwent open procedures due to surgeon preference. Patient demographic characteristics and study outcomes are summarized in Tables 4 and 5. No significant differences were noted between the three groups with regard to demographic data, although a higher prevalence of ASA IV persisted in the open group (Table 4). Although the use of vasoactive agents was seen in 2 of 3 possible MIS candidates, these medications were documented to be low dose and weaned before the patients' surgical intervention due to hemodynamic stability.
Characteristics of Patients Who Had an Open Versus Open/Possible MIS Versus MIS Repair
ASA, American Society of Anesthesiologists; IQR, interquartile range; MIS, minimally invasive surgical.
Postoperative Outcomes of Patients Who Had an Open Versus Open/Possible MIS Versus MIS Congenital Diaphragmatic Hernia Repair
Intraoperative opioid use did not differ among the three groups. However, the 3 possible MIS candidates were exposed to MEs of 9 mg/kg (IQR 4, 10), 30-fold more than in the 8 patients who actually underwent an MIS procedure. When the 3 MIS candidates were removed from the open group, median MEs for the open group increased to 38 mg/kg (IQR 17, 59) (P = .006). No differences were seen in postoperative acetaminophen use. Postoperative pain scores in the possible MIS candidates were lowest on POD 1 and then were noted to oscillate through the week with peak pain scores on POD 3 and 5 when compared with the open and MIS groups

Highest daily postoperative pain scores in patients undergoing open versus open/possible MIS versus MIS CDH repair. CDH, congenital diaphragmatic hernia.
Discussion
MIS techniques have gained popularity in the adult population due to the advantages provided both intraoperatively and postoperatively. These include better intraoperative visualization, improved postoperative pain control, decreased LOS, and fewer pulmonary complications. Our retrospective review indicates that these advantages may also apply to neonates undergoing CDH repair as we noted a decrease in postoperative opioid consumption, time to tracheal extubation, time to resuming of oral feeds, and hospital LOS in the MIS cohort.
Although several factors may impact the hospital course of neonates undergoing CDH repair, we found that patients undergoing a MIS CDH repair had close to a 100-fold reduction in median postoperative opioid consumption compared to those who had an open approach. This was primarily due to the lack of a continuous postoperative opioid infusion in the majority of patients in the MIS group. These findings should be taken in the context of the limitations of a retrospective study. Our review of pain practices in these patients revealed no standardization regarding the analgesic regimen, which resulted in variations in opioid administration among the NICU providers. These findings provide the foundation for future improvements in postoperative management of CDH patients, which may involve a more protocolized approach to minimize continuous opioid infusions where appropriate.
Ceelie et al. retrospectively evaluated the impact of MIS versus open surgery in neonates with CDH and EA. 9 The authors included two control patients for each MIS patient, matched by diagnosis, gender, and age at surgery. Opioid dose titration was based on pain scores (VAS and COMFORT behavior) and administered using a previously reported nursing-applied protocol. They noted no difference in opioid needs (expressed as intravenous MEs) or pain scores between the two groups. The authors concluded that MIS for the repair of EA or CDH was not associated with decreased opioid use. Other outcome parameters were not reported. Various differences may explain the discordant results when compared to our findings. The majority of the patients in the cohort reported by Ceelie et al. were still receiving mechanical ventilation at 48 hours (75% in the MIS group and 80% in the control group). In addition, per their opioid protocol, many were receiving a continuous morphine infusion at 10 μg/kg/hour.
With little available evidence on minimally invasive surgical approaches and postoperative opioid consumption in neonates, we set out to determine if a difference existed in patients undergoing MIS for CDH at our institution. Since our institution lacked a standard protocol for postoperative pain management for these patients, their pain management varied depending on provider unlike the data reported by Ceelie et al. 9 However, the MIS group was less likely to receive a continuous opioid infusion, which was always used in the open thoracotomy group.
The reduced postoperative opioid consumption may be, at least partially, responsible for the decreased time to tracheal extubation, to resuming oral feeds, and to hospital discharge. The patients in the MIS group were able to achieve the same pain scores as the open group, but required a significantly decreased dose of opioids which may limit adverse effects of opioids, including decreased respiratory drive, ileus, sedation, and nausea, which can all lead to prolonged hospitalization. In examining the subgroup analysis of those patients who underwent an open procedure but could have undergone the MIS approach to address surgeon preference, the possible MIS patients demonstrated a 30-fold increase in postoperative opioid consumption and experienced a delay in time to tracheal extubation, oral feeds with increased LOS when compared to patients who actually underwent an MIS repair. These findings may suggest in patients who are MIS candidates despite surgeon preference, a thoracoscopic approach should be considered to minimize opioid consumption and optimize postsurgical recovery variables.
While our study demonstrated a statistically significant difference in the postoperative opioid consumption of patients undergoing CDH via the minimally invasive technique, there are limitations which must be taken into consideration. First, this was a retrospective review with a limited sample size, which precludes the ability to perform multivariable analysis. In addition, there were multiple patients who were excluded from the study because of missing intraoperative data, due to the transition from paper charting to the electronic medical record in the operating room. Other data errors may be present with respect to postoperative pain scores. The timing or interval for the assignment of pain scores was not standardized and interprovider variability may exist in the assignment of scores. Finally, the difference in ASA status between the MIS and open groups may have biased results in favor of the MIS group due to the sicker patients being in the open group. Patients with higher ASA status were not necessarily undergoing the open approach due to the severity of their illness, but rather due to the preference of the surgeon performing the operation. During the period reviewed, many of the surgeons were more comfortable performing the open approach versus the minimally invasive approach, which may have biased their decisions to perform the open approach in the higher ASA status patients. Although the use of ASA categorization has been used as a proxy of disease status, specifically in patients with CDH, 12 the authors note the subjectivity inherent with ASA classification as its designation may be provider dependent. In the current study, one patient in the MIS group was designated as an ASA II, whereas in the views of the authors, a diagnosis of CDH would be a minimum designation of an ASA III.
Overall, our study suggests a benefit to performing MIS for CDH repair in neonates with respect to postoperative opioid consumption, time to tracheal extubation, time to restarting oral feeds, and hospital LOS. Provider variation in postoperative pain management for these patients provided an opportunity to detect decreased need for continuous opioid infusions, but may also illustrate the need for a standard approach to pain management after MIS procedures. It is possible that patients who undergo the MIS approach may have satisfactory pain control with only bolus dosing of opioid pain medications rather than continuous infusions. Future studies are needed to determine the best perioperative management strategies to optimize postoperative outcomes in minimally invasive neonatal surgery with respect to pain management, which may include the use not only of opioids but also of adjunctive agents (acetaminophen) and regional anesthetic techniques.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.