
Abstract
The management of morbidly obese patients with a concomitant ventral hernia (VH) is a great challenge for surgeons. There is controversy over the optimal strategy to tackle both health problems, requiring an individualized approach. Obese patients have a higher recurrence rate after hernia repair, and bariatric surgery in the presence of a VH can be difficult. As morbid obesity is related with severe comorbidities, including increased cardiovascular and anesthetic risks, some advocate for a single-stage strategy. A primary hernia repair carried out during the bariatric surgery, however, may increase morbidity without definitively solving the problem. Biological meshes are expensive and also have a high recurrence rate. The laparoscopic placement of a synthetic mesh offers good results, but it is worrisome because bariatric surgery is a clean-contaminated procedure. Moreover, there is a great chance that a plastic surgery would be necessary after completing the weight-loss process, and the abdominal wall surgery could be performed at that point. There are many arguments, but the evidence is weak. We present an extensive review of the currently available literature on the management of VH in morbidly obese patients. We aim to provide objective information regarding the pros and cons of the different strategies that have been proposed, to facilitate the selection of the best approach to individual morbidly obese patients with abdominal wall hernias precising both of surgical repair.
Introduction
Obesity, defined as a body mass index (BMI) ≥30 kg/m2, has been related with a higher risk for the development of ventral hernias (VH), both primary and incisional hernias.1,2 Also, factors such as an increased BMI, abdominal circumference or visceral fat have been shown in multiple studies to increase the risk for surgical site infection (SSI) and VH recurrence after ventral hernia repair (VHR).2,3 Furthermore, morbidly obese (MO) patients associate a myriad of metabolic derangements, such as type 2 diabetes mellitus (T2DM) that could also explain many of the postoperative complications noted in this population. 4 Thus, VH repair in MO patients can be challenging, even in expert hands, and yield a high recurrence rate. Obesity and diabetes are chronic inflammatory conditions, demonstrated by the increased levels of inflammatory markers, and metabolic and bariatric surgery (MBS) has proved successful in the treatment of both. 5 Nowadays, the main MBS primary techniques are Roux-en-Y gastric bypass (RYGB) and sleeve gastrectomy (SG). 6 Obesity incidence has risen over the last decades, and bariatric surgeons must be prepared to manage an increasing number of obese patients with VH on their practice. Moreover, MBS could be an essential strategy in the management of MO patients with VH, and should be strongly considered. 7 Unfortunately, although nearly 60% of patients undergoing a VHR in the United States had a BMI >30 kg/m2 (Ref. 7 ), to date there is no consensus on the optimal timing or method of VHR in this particular population. This literature review aims to address the current evidence regarding the management of MO patients with VH.
Materials and Methods
A literature review was conducted to evaluate the evidence that support the different approaches and optimal timing in VHR for MO patients that also require BMS. Electronic searches with a combination of the terms, “ventral hernia,” “incisional hernia,” “abdominal wall hernia,” “gastric band,” “gastric bypass,” “sleeve gastrectomy,” and “bariatric surgery” were performed in MEDLINE, PubMed and Cochrane Library databases. The selected articles were reviewed by 2 surgeons, and relevant data were extracted and discussed. A manual search through the references cited by these selected articles was also performed, to identify additional relevant bibliography. Searches were restricted to English language articles. Editorials and pediatric studies were excluded.
Current status
Unfortunately, there is a lack of consensus on the management of MO patients with indication for MBS that also have a VH,8–10 as there are still many unresolved questions. For instance, should MBS be performed before, after, or at the same time that VHR? What is the best management for a patient that requires MBS but has a previous history of recurrent VH? Is it different if the VH is symptomatic than if it is asymptomatic? 10 Most surgeons take an individualized approach based upon the patient's symptoms, bariatric goals, BMI, comorbidities, and hernia characteristics.8,11 Moreover, it should be kept in mind that the concomitant comorbidities of MO that include T2DM, sleep obstructive apnea syndrome, hypertension, and hypercholesterolemia, confer to those patients higher anesthetic and cardiovascular risks. 12
An algorithm that guides the approach to MO patients with VH has to consider three different potential complications: risk of incarceration, risk of SSI, and risk of recurrence. According to the clinical situation, there are three possible scenarios. The first is when the patient was enrolled on a bariatric surgery program and weight loss is the priority. In that case, weight loss through MBS can prepare the patient for a later VHR (combined, or not, with plastic surgery) on better conditions. In the second, VHR is a priority over MBS. To note, depending on the VHR repair method, future surgical procedures may be limited due to restricted laparoscopic access or reduced abdominal wall compliance. The third scenario combines VHR with MBS. Some recent literature, including a consensus guideline on MBS and VH promoted and published in 2018 by the American Society for Metabolic and Bariatric Surgery (ASMBS) and the American Hernia Society (AHS), 9 suggest that when both procedures can be performed laparoscopically, a single-stage approach would minimize the anesthetic risk. Conversely, in patients with MO and a VH that is not amenable to laparoscopic repair, a staged-up approach would be recommended. However, they stated that those guidelines were not to be seen as the only standard of care, and other algorithms have also been proposed.8,11 Moreover, the fact that nowadays most patients could be suitable to laparoscopic VH surgery makes the decision more challenging. Strategic thinking must be applied to select the right pathway for each patient. A description of the evidence according to the possible scenarios in patients with MO that required VHR and MBS will be provided (Fig. 1).
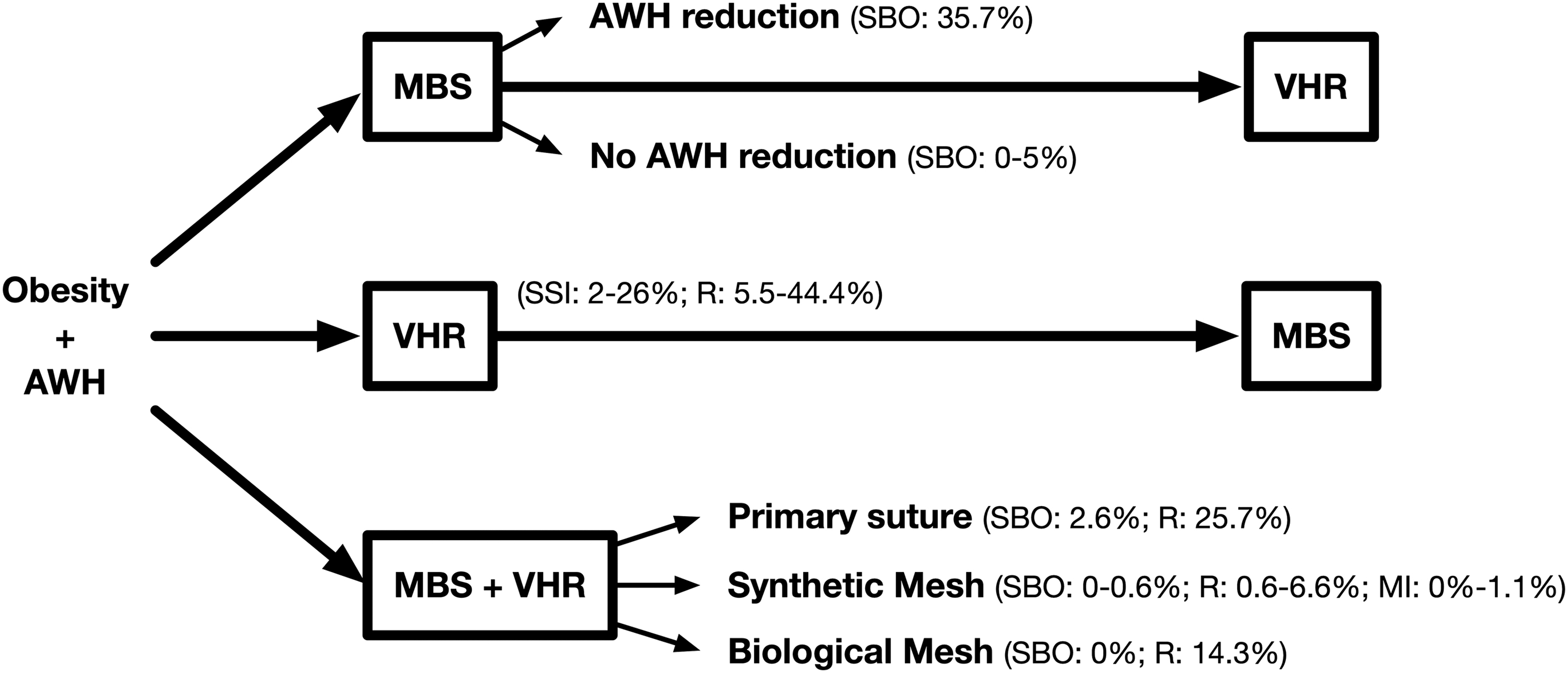
Algorithm showing possible management for AWH in morbidly obese patient, including references from the text. AWH, abdominal wall hernia; MBS, metabolic and bariatric surgery; SBO, small bowel obstruction; SSI, surgical-site infection; VHR, ventral hernia repair.
MBS as a first-stage procedure
Given that, as previously mentioned, obesity significantly increases the risk of recurrence and SSI after VHR, a recent consensus guide from the ventral hernia outcomes collaborative recommended to avoid surgery in patients with BMI ≥50 kg/m2. In patients with BMI between 30 and 50 kg/m2, they advised to undertake some weight loss intervention before the elective VHR. 13 These strategies include diet, lifestyle changes, pharmacological interventions, endoscopic procedures, and MBS.
Rosen et al. 14 reported their experience providing a very-low-calorie diet (<800 kcal/day) and a tight follow-up program to 25 patients before VHR. BMI lowered from 48 (±10) kg/m2 to 39 (±7) kg/m2 in 17 months, allowing 24 patients to undergo a subsequent VHR with decreased risk. Moreover, weight loss was maintained by 88% of the patients for a postoperative average of 18 months. 14 Nevertheless, preoperative diet has provided mixed results in other studies. 9 Theoretically, weight loss-approved drugs could offer some mild benefit, although to date no studies have been conducted to test that strategy. The placement of an intragastric balloon, or other related endoscopic techniques, could be an alternative option. However, these procedures are not risk free and have transient effects, raising the question if any advantage is offered over conventional diet interventions.15,16 MBS, on the other hand, has shown good long-term outcomes with an acceptable risk profile, and could be the optimal strategy to minimize VH recurrence while resolving the metabolic condition.
However, judging by the few reports that describe this strategy, the use of MBS as a bridge to VHR has not been the most common alternative.8,11,17 Insurance obstacles, or the patient's indisposition to MBS, could have been involved in these findings. Otherwise, as good candidates to laparoscopic MBS are also good candidates to laparoscopic VHR, a single-stage procedure could have been preferred in most cases. Nevertheless, some VH characteristics (extensive wall defects, loss of abdominal domain, incarcerated proximal bowel, or poor-quality skin, for instance) might make a combined approach unfeasible. 9 Those complex cases could benefit from an aggressive weight loss before VHR is attempted, as SSI and recurrence risk may decrease to that of lean population. Besides, the involvement of an abdominal wall expert in the surgical team before MBS seems advisable.
Although the evidence is weak, limited to retrospective case series, when performing a MBS as the first step of a two-stage strategy, it is recommended not to reduce the content of the hernial sac. Eid et al. 17 reported the postoperative evolution of 14 patients that, during a laparoscopic RYGB, underwent adhesiolysis and reduction of a VH with omental incarceration, with no subsequent repair. Five of those patients (35.7%) developed small bowel obstruction (SBO) due to incarceration on an average of 63 days (range 10–150) after surgery. Conversely, Newcomb et al. 8 described 20 patients with large defects that were not reduced during RYGB, of which only 1 (5%) required a surgical repair of the incarcerated hernia 11 months after surgery. Moreover, Datta et al. 11 also identified 8 patients with a VH that was left untouched during laparoscopic RYGB, with none of them developing any complication during the 14 months of follow-up. It is possible that the fresh scar produced by adhesiolysis could increase the chances of bowel incarceration, thus explaining the previous results. Based on these findings, a “no-touch” approach would seem to be the safest option.8,11
Hernia repair before MBS
Delaying the repair of a symptomatic VH may result in the need of an emergency VHR. According to the Danish national patient register, there is a 3.2% risk of incarceration when a watchful waiting strategy is adopted. 18 This is a critical factor that may influence the surgeon's timing of VHR and could be a sound argument against deferring VHR while MBS is considered. In fact, the previously referred consensus guidelines from the ASMBS and AHS 9 accepts the possibility of approaching VHR as an initial and separate procedure, preceded by some weight-loss strategy and followed later on by bariatric surgery, generally in a short time to minimize the risk of recurrence. The same strategy is proposed by Eid et al. for patients with clinically accessible symptomatic hernias, with excellent clinical results. 17 Thus, one of the critical elements to select the appropriate treatment modality for these patients is to evaluate their symptoms and individually tailor each strategy.
The surgical technique also seems to be a relevant factor. While open VHR in MO patients has been clearly associated with a fairly higher recurrence rates, laparoscopic VHR may have better results. 9 Moreover, laparoscopic surgical procedures offer the benefits of lower postoperative pain, quicker recovery, and lower wound complication rates compared with open surgical procedures. Several studies have demonstrated the feasibility of laparoscopic VHR in patients with MO. In one of the most extensive series, a laparoscopic VHR was performed in 163 patients with a mean BMI of 38 kg/m2. It found a very low rate of wound complications (1.2%) and a recurrence rate of only 5.5% at a mean follow-up of 25 months. 19 Furthermore, a retrospective, nonrandomized study by Ching et al. found no significant differences in the complications rate, including recurrence after laparoscopic VHR, when MO and non-MO patients were compared with a median follow-up of 19 months (range 6–62). 20
Simultaneous VHR and MBS
Since nowadays MBS is almost exclusively performed laparoscopically, and laparoscopic VHR seems to have good results in MO patients, a single-stage approach is very appealing. Moreover, there are cases where an unplanned reduction of a VH must be performed during MBS, or a small VH that had previously gone unnoticed is discovered intraoperatively (Fig. 2). Many retrospective case reports, as well as one large-scale registry data analysis, demonstrate the safety and good short-term results of simultaneous laparoscopic VHR and MBS. In one of the first published case series, Eid et al. reported 85 patients with VH (mostly umbilical) who underwent a RYGB. 17 All patients had at least 6 months of follow-up. Fifty-nine patients received a primary sutured repair, 12 biological mesh, and 14 had the repair deferred. Early morbidity was minimal in all groups, and LOS was not affected by the concomitant umbilical VHR. At a mean follow-up of 26 months, the authors reported a 22% recurrence rate in the group of patients that underwent the primary suture and no recurrences in those repaired with a biological mesh, suggesting that mesh repair was preferable. Furthermore, as previously noted, 35.7% of patients with the deferred hernia repair developed SBO due to incarceration.
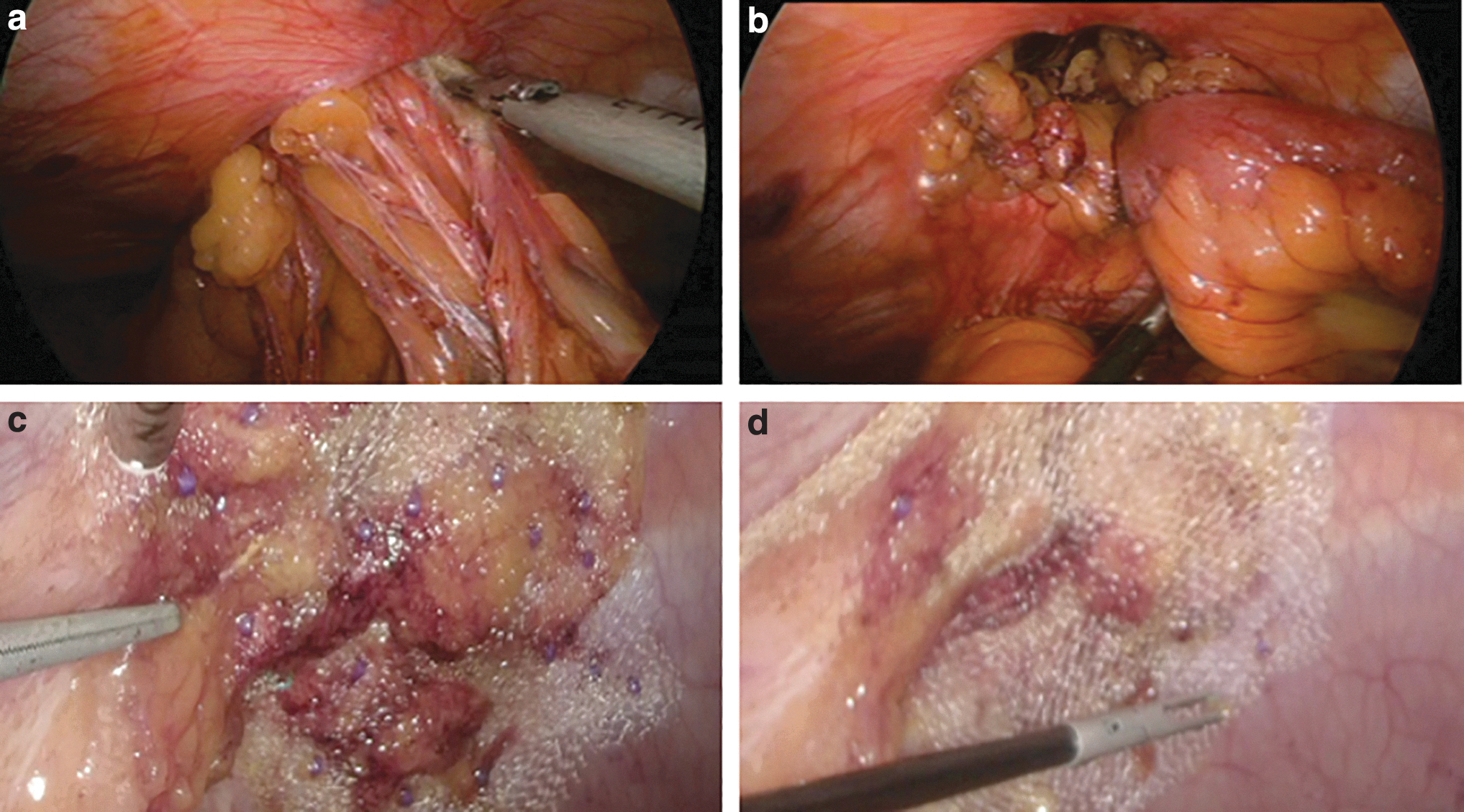
Images showing the intraoperative treatment of an abdominal wall hernia defect during a bariatric procedure.
In a comprehensive systematic review from 2018, Lazzati et al. 10 summarized the outcomes of the three most common strategies of VHR during MBS (primary suture, synthetic mesh, and biological mesh use). The primary suture has a lower cost and shorter operative time compared with any mesh. However, postoperative SBO risk is not neglectable (2.6%), and long-term recurrence is high (25.7%). 10 The use of biological meshes has been advocated in clean-contaminated environments, like MBS, but they are more expensive than nonbiological alternatives. Moreover, although no postoperative SBO had been reported, VH recurrence reached 14.3%. Synthetic meshes, on the other hand, had a recurrence rate of only 1.1%, with no SBO cases found in that review. Other recent studies have also described good outcomes with synthetic meshes. In its limited series of 15 patients, Marzouk et al. had 1 recurrence (6.6%). 21 Furthermore, Praveen et al., on its retrospective series of 156 patients, had also only one recurrence (0.6%). 22
However, no discussion will be complete without evaluating the safety concerns of using a synthetic mesh simultaneously with stapled bariatric procedures, where the gastrointestinal tract is divided and the mesh could be contaminated. Published data report that no more than 1.1% of cases presented with complication, and none required mesh removal.10,21,22 An interesting study in which peritoneal fluid samples were obtained before and after 51 SG and 26 RYGB, found that 0% of SG and only 15% of RYGB cultures had a positive result. 23 According to these results, it should be considered to adapt the MBS technique, opting for a SG in super-obese or borderline cases. A second bariatric procedure, such as single anastomosis duodenoileostomy, could be added later in case of insufficient weight loss during follow-up. In that case, however, it has to be considered that the risk of a laparoscopic injury increases twofold in the reoperation of a patient with a previous intraabdominal synthetic mesh. 24
Conclusion
Weight loss must be an integral treatment element in a MO patient with VH, not only to reduce the risk of SSI and recurrence after VHR, but also to improve the longevity and quality of life of the patient in the long term. To date, three options have been proposed: MBS first, VHR first, and a combined strategy. All three have their advantages and disadvantages, and an individual approach is warranted. Although the evidence is limited, a single-stage laparoscopic strategy with the placement of an intraabdominal synthetic mesh seem to have good results, and it should be considered whenever possible.
Footnotes
Acknowledgment
The authors would like to acknowledge Dr. Mariano Palermo ICYLS (International Club of Young Laparoscopic Surgeons) for the invitation.
Disclosure Statement
No competing financial interests exist.
Funding Information
There are no sources of support to be reported from any organization.