
Abstract
Background:
It has been reported that the incidence of recurrent laryngeal nerve (RLN) injury is higher in an operational procedure in the thyroid and parathyroid region. Elevating voice pitch is achieved by the cricothyroid contraction, which in turn is innervated by the external branch of the superior laryngeal nerve (EBSLN). Due to the subtle nature and clinical variability of EBSLN damage, diagnosis may be difficult. The use of intraoperative neuromonitoring (IONM) as a supplement to enhance surgical identification in thyroid and parathyroid operation appeared to have collected momentum with operators.
Methods:
IONM clinical usage rationale, efficiency, and safety profile are discussed in this overview in thyroid and parathyroid surgery.
Results:
IONM usage incurred numerous skepticisms in decreasing the frequency of EBSLN or RLN injury. However, a recent article has shown the efficacy and benefits of using IONM in thyroid and parathyroid procedures. IONM facilitates the recognition of RLN and EBSLN, verifies its functional integrity, localizes the site of a nerve injury, and gives postsurgical function feedback. This technique has been successful in reducing rates of bilateral laryngeal paralysis, with the elevated safety profile for surgical patients.
Conclusions:
It is recommended using IONM in all thyroidectomies and in high-risk parathyroidectomies.
Introduction
With serious complication from thyroid and parathyroid operations, recurrent laryngeal nerve (RLN) injury and its associated symptoms are a common sequela.1,2 Functionally, RLN enables contraction of the vocal cords by controlling the intrinsic laryngeal muscles. Bilateral RLN injuries are ominous, requiring immediate intubation or tracheostomy. By contrast, RLN injury unilaterally poses a fewer danger, causing only hoarseness of voice with the stillness of the ipsilateral vocal cord. Statistically, the incidence of temporary and permanent RLN injury was found to be 2.3% and the latter being 9.8%. 1 The mechanisms of the RLN injury include stretching, transection, entrapment, ischemia, or electrothermal injury, but the most frequent encounter is due to nonstructural functional nerve injury.3,4
Prevention is the key for patient safety, and the golden standard for the avoidance of RLN injury during the thyroid and parathyroid operation is the direct visualization—lessening the chance of lasting RLN damage. However, it does not entail the functional integrity of a structurally intact nerve.5–7 In addition, it is worth noting that even though intraoperative exposure of RLN during general open field thyroid surgery is simple to undertake, it perhaps is not as feasible during minimally invasive video-assisted thyroidectomy (MIVAT) due to limited field of view.
The use of intraoperative neuromonitoring (IONM) as a supplementary to visual identification of the RLN in thyroid and parathyroid operation has gained increasing acceptance and is becoming a standard practice around the world. The technical aid that IONM provides during surgery to consistently recognize RLN is one of the reasons for its growing recognition. Also, as the operation inches to an end, the functional integrity of the RLN can be verified. In the scenario of IONM detecting an intraoperative loss of electromyogram (EMG) signal unilaterally, staged surgery could be drafted out in advance. From the perspective of challenging cases such as variation of anatomy, reopening, and malignancy, IONM could seek out vital information to abridge the situation.8–10 IONM, according to various studies, has been shown to lessen the incidence of temporary RLN injury,11–13 through guidance during RLN dissection, and lessen the mechanical damages to its anterior branches due to excessive exposure. 14
A recent randomized article proposed temporary RLN paralysis is significantly decreased in the high-risk group with neural monitoring than only direct visualisation. 13 Other studies disclosed successful sporadic IONM usage during MIVAT can be performed without enlarging the incisional dimension, nor pose an additional danger to the operation. The technique offers adequate flexibility and space for maneuvering for isolating carotid sheath and performing vagal stimulation, thyroid lobe dissection, and exposing the RLN. 15
Based on the location of the injury and manifestation of IONM, two types of RNL injuries have been reported. Type I injury or segmentary lesion, in which IOMN stimulation partially travels down the vagus nerve (EMG positive distally) through the RLN until the injury point, thus lacking EMG signal proximally. If such occurrence is seen during the operation, lack of signal prompt surgeon to circumvent and yield additional damage diminishes lasting RLN injury. Over 70% of RNL displayed Type I injury and was frequently due to excessive shear or compressional forces on nerve tissue or electrothermal damages. Type II injury, on the other hand, devoid of any EMG signal over the entire path of stimulation, pinpoint of lesion site, therefore, cannot be ascertained.
However, a contralateral vagal stimulation will yield an EMG response. Mechanism of injury has not been unearthed, although theorized that vagal nerve is damaged further distally and is due to an unwarranted shear force applied when the thyroid lobe was medially retracted.16,17
The rationale of IONM usage
A multitude of rationale support IONM usage in thyroid and parathyroid operation. Neural mapping of RLN in the paratracheal region can be performed with IONM with exploratory probing then visualization, especially in complicated situations such as reoperative surgery and surgery for malignancies. Multiple studies suggested that IONM was associated with a high rate (98%–100%) of nerve identification, and a reduction in operative time due to increased speed of RLN identification.18,19 In addition, the functional integrity of the RLN can be verified by IONM.8,19 By first checking intact and functioning RLN on the operated side before proceeding to the contralateral side, bilateral RLN injury and subsequent vocal cord paralysis can be mitigated.20,21 Furthermore, IONM provides necessary aid in elucidating site of nerve damage, thus providing prognosis to postoperative functional integrity of RLN.
IONM will be able to identify the injured segment of nerve; the precise point of nerve injury is localized by serially stimulating the RLN starting from its entry point at the cricotracheal junction and moving in a distal to proximal direction until the loss of signal (LOS) occurs. The surgeon may have the opportunity to reverse the maneuver and avoid permanent RLN injury. Numerous reports exhibited high negative predictive value (NPV) associated with IONM, so in the nominal EMG, signal at the epilogue of operation is typically expected with a considerable probability of unhinged functioning vocal cord. 22 Finally, monitoring and protecting the external branch of the superior laryngeal nerve (EBSLN) are increasingly being recognized for ameliorating voice outcomes after thyroid operation and has been highlighted in the Clinical Practice Guideline. 23
IONM system and consideration for anesthesiology
Two neural monitoring systems are widely used currently; the first is an audio-only system. This system will not be able to analyze the waveforms and cannot quantify the EMG response to RLN stimulation. Thus, it is challenging to isolate noise and signal with only acoustic prompts. The latter system composed of audio plus waveform system, which adds to acoustic information; the waveform can be presented on screen. 24
EMG activities are monitored by the needle electrodes into the vocalis muscle or adhering endotracheal tube-mounted surface electrodes to the mucosa of vocal cords, although latter bestows a diminished signal amplitude compared to needle type, but, nevertheless, just as valid.25,26 On the other hand, invasive recording electrodes attribute an increased risk for trauma, infection, and incidental disunion of electrodes during operation.27,28 Endotracheal tube surface electrodes with audio plus waveform monitor systems are preferred for IONM in thyroid and parathyroid operation, both triggered and spontaneous EMGs are monitored during the procedure.
Before IOMN implementation, a thorough and timely discussion with the anesthesiologist is warranted. The concern mainly lay with a technical demand of sparingly used muscle relaxant, due to drug effect in reducing signal to noise ratio in EMG, dropping propensity of injury detection. Furthermore, this gives the anesthesiologist time to contemplate anesthesia titration, tailored for the individual patient, based on numerous comorbidities, and balance sedation depth, while maintaining the EMG signal at a satisfactory level. One example is to use a short-acting nondepolarizing agent with prompt intubation, and hold back further muscle relaxant dosing. Another example is to deploy intravenous-only anesthesia. Optimal electrode adherence to vocal cords demands the largest conceivable endotracheal tube that could safely be introduced, but awareness should be taken that IOMN tubes have a wider outer diameter than usual. Thus, careful selection of tube sizing should be noted. 29
Loss of signal
The international standard guideline statement confers 29 LOS in RLN neuromonitoring is defined as lack or markedly diminished EMG signaling (<100 μV) with stimulation, without signs of laryngeal twitch, and carefully ruled out any equipment problem or neuromuscular blockade.29–31 The interpretation of LOS is only valid and is dependent on clear EMG signal with an amplitude above 100 μV. After obtaining such a signal, further decrease in magnitude below the threshold, even with a substantial suprathreshold level of stimulation between 1 to 2 mA, hints an indication of a true LOS and neural injury must strongly be suspected, especially when amplitude decrease is connected with prolonged latency EMG responses.29–31
During the situation, when intraoperative LOS arises, a flowchart protocol shall be followed to isolate the root cause of signal loss (Fig. 1). If the stimulation of RLN produces either no EMG activities or unusually low amplitude EMG waveforms lower than 100 μV, surgeon shall investigate the laryngeal twitch response. If present, a negative LOS most commonly caused by malposition of the endotracheal tube electrode may be the culprit. In addition, grounding electrodes ought to have separated, severing the electrical connection. Thus, grounds should be repositioned. All connections of the electrodes should also be tested in this scenario.29,32
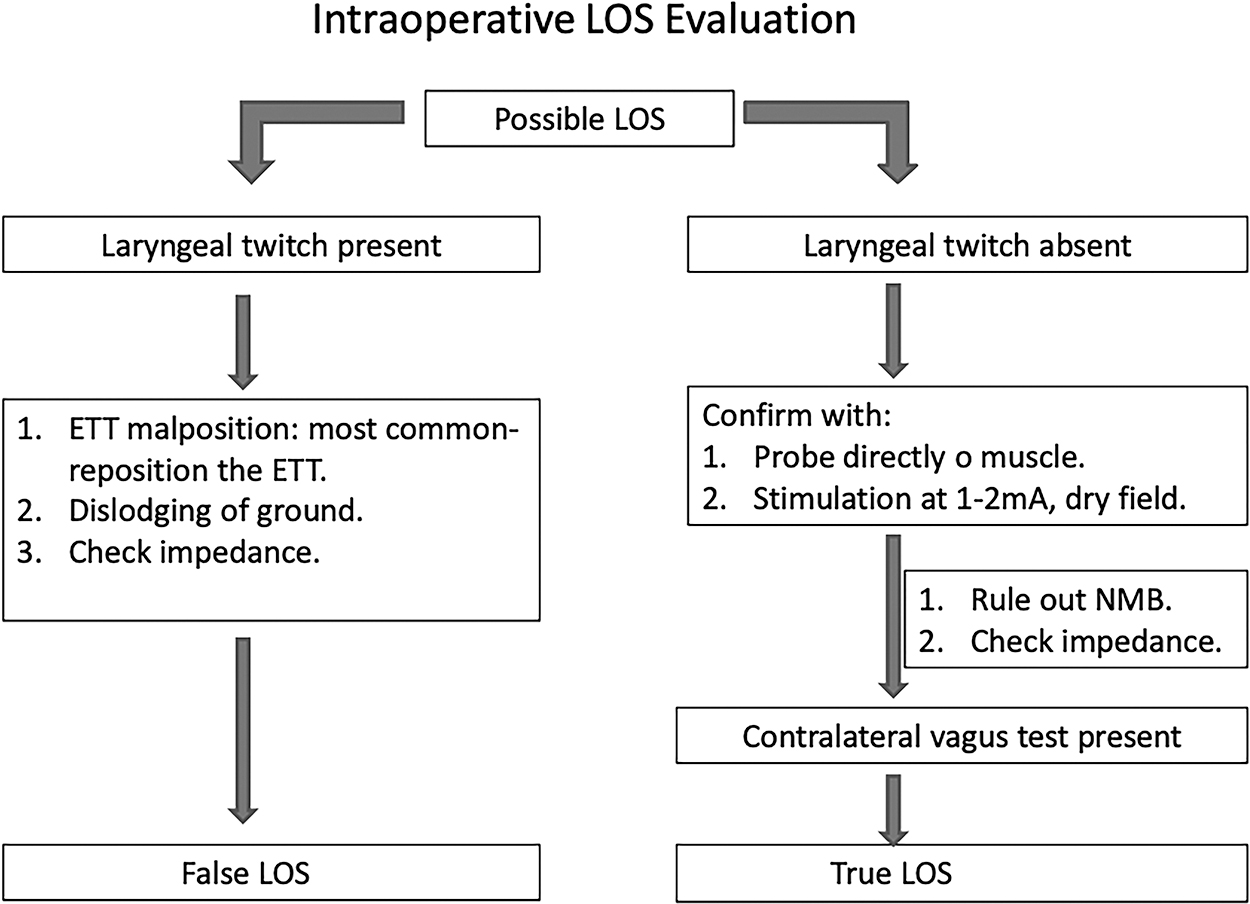
Algorithm of evaluation of LOS during surgery. ETT, endotracheal tube; LOS, loss of signal; NMB, neuromuscular blocker.
Conversely, if the laryngeal twitch is absent during suprathreshold stimulation, again, the first step is making sure all connections of the electrodes are secured, and check that the stimulator probe is working by directly stimulating any muscle to obtain a twitch confirmation. Then stimulate the vagus nerve on the contralateral side. Responsive signaling entails IOMN is not faulty, and a true LOS episode shall be contemplated.
As soon as LOS is confirmed, two matters ought to be pondered. First, one shall localize the injury site, or known as neural injury site mapping, serially testing the whole sector of nerve, from the laryngeal nerve entrance point distally, inches proximally until the site of injury is found. In the scenario of Type I RLN injury, surgeons might have opportunities to possibly reverse the lesion to avoid lasting damage. Second is a review of ideal contralateral scheduling in a two-stage operation. The most feared sequelae of thyroid operation are bilateral vocal cord palsy; temporary or permanent tracheotomy is often undertaken. One study described the blanketed usage of a neural monitoring device in nonmalignant thyroid operations, and along a sensible staged procedure could result in minimal bilateral RLN injury. 33
Staged operation is vital as postoperative transient RLN paralysis tends to occur in high rate with true LOS with minimal recovery by the conclusion of the operation. This held true even in circumstance of malignancies, as bilateral RLN paralysis poses more of immediate concern.
At the end of operation, true LOS based on EMG signaling has three outcomes, continued LOS without recovery, incomplete signal recovery, and full signal recovery. Vocal cord flexibility can be classified as normal, weakened, or fixed.29,32 One study reported 16 RLN nerves with true intraoperative LOS, and 15 out of 16 RLNs had reentry signals, and only with 3 nerves developed temporary vocal palsy. 34 Another study reported a detailed observation of 13 nerves with true LOS caused by Type I injury. Three nerves had a full recovery, all with normal cord mobility, 3 incomplete recoveries, 2 with weakened cord, and 7 without any improvement, all with fixed mobility. 3 The verdict to plan a staged thyroidectomy requires 20 minutes of rest.30,31,34 A proportion of LOS exhibits temporary mild nerve block, the return of function may resume before the conclusion of surgery. 35 Hence, the waiting period serves to avoids possible superfluous staged surgery.
Diagnostic accuracy of laryngeal nerve monitoring
Consistently, IONM in thyroidectomy scored a high NPV in various studies, varying from 91% to 100%. 36 When a positive signal was attained with stimulation of the RLN at the conclusion of the operation, it was almost unvaryingly linked with a nominally functioning vocal cord at the postoperative laryngoscopic examination. In a pooled meta-analysis, an aggregate of 7366 nerves at risk (NAR) cumulated in a mean NPV of 99.15%. However, due to a lack of positive predictive power, resulted in a mean positive predictive value (PPV) of only 61.3% based on 4700 NAR from the same study. 37 Thus, applying stricter criteria and standardization can reduce technical pitfalls, thereby improving future PPV of neuromonitoring. IONM during thyroidectomy standard outline has been proposed to improve the diagnostic accuracy of IONM. The guideline encompasses monitoring device setup processes, endotracheal tube insertion, and unity of a sequence for diagnosing signal issues.
IONM of EBSLN
The importance of protecting EBSLN is increasingly being recognized and has been highlighted for improving postoperative voice outcomes. 2 The EBSLN innervates the cricothyroid muscle, which is accountable for lengthening and tensing vocal folds to bring higher pitch phonation and volume. Thus, dysphonia, secondary to injury of the EBSLN, is likely to affect professionals who push their vocal intonation.38,39 Thyroid artery and superior pole of thyroid are variable landmarks, anatomical EBSLN classification with visual identification relies on these structures. Therefore, there seems to be an inconsistency between individuals. 38
In one metadata analysis of 56 studies, which comprised 13,444 EBSLNs, the data showed a 95.9% identification rate with the usage of IOMN than 76.5% through direct visualisation. 39 Other studies also confirmed EBSLN identification improves with IONM devices compared to conventional methods. In a total of 189 expected EBSLN, 155 (82.01%) were identified with the traditional method, whereas 181 (96.76%) with IONM device. Therefore, the article suggested all thyroid operations should routinely use IONM device for identification of EBSLN. 40
Naytah et al. reported metadata analysis of seven studies from January 1, 1995, to July 1, 2018, and the results showed higher identification of EBSLN at risk than the conventional control. 41 Gurkeyik et al. showed that IONM-mediated cricothyroid muscle twitch is useful for functional integrity identification of EBSLN. Also, a high-amplitude waveform can exist, summarizing intrinsic laryngeal muscles are innervated by EBSLN as an alternative source.38,42
Usage of IONM also contributes to the mapping of anatomical nerve identification. Although EBSLN can be easily identified by seasoned thyroid surgeons visually, functional status requires IONM, and especially in malignancies, or reoperation, where structures were altered. It is recommended to use IONM as an excellent supplementary technique for surgical exploration, identification for primary, reoperation, and verify EBSLN functional integrity. 43
Diagnosing EBSLN injury is challenging, and contributed to unclear incidence rate. However, the cricothyroid dysfunction proportion of up to 58% has been reported.41,43,44 Immaculate separation of tissues and care taken throughout the surgery, particularly around the superior pole, seem to lead to lowered incidence rate to EBSLN damage, thus providing a better vocal clinical outcome. 45 Liddy et al. assessed outcome for EBSLN damage during operation with and without IONM, results demonstrated in eight injured patients with nine damaged nerves without IONM, but only a single injury with solely damaged nerve with IONM intervention. Most of the gross and functional nerve detection was made by IONM (P < .001). The authors concluded that IONM usage during superior pole dissection of thyroidectomy has seen a significantly lower incidence of harmed EBSLN, and hence recommend IONM for all thyroidectomy to prevent unnecessary incidence. 46
Conclusion
Although the usage of IONM in lessening the occurrence of RLN or EBSLN injury is unconfirmed and remains controversial, the use of IONM as a supplement to enhance surgical identification in thyroid and parathyroid operation appeared to have collected momentum with operators. IONM is an exceptional device for its role in nerve identification, functional integrity verification, and injury site localization, and can produce clinical prognosis by the end of the operation, leading to enhanced safety profile. The professional training session could make use of IONM device, identifying anatomical variants of the RLN and EBSLN. In addition, information collected from cases contributes to further research. It is recommended using IONM in all thyroidectomies and in high-risk parathyroidectomies.
Footnotes
Disclaimer
No competing financial interests exist.
Disclosure Statement
The authors, their immediate families, and any research foundation with which they are affiliated did not receive any financial payments or other benefits from any commercial entity related to the subject of this article. None of the authors have any conflicts of interest with regard to this research.
Funding Information
The authors received no financial support for the research, authorship, or publication of this article.