
Abstract
Background:
The transoral endoscopic thyroidectomy by vestibular approach (TOETVA) has been developed for thyroid microcarcinoma (TMC) treatment worldwide, with low rate of complications and excellent oncological results. However, this approach has still not been routinely performed. Thus, in this study, we aim to demonstrate the feasibility and safety of this technique in the clinical practice.
Methods:
In this prospective cohort study, 29 patients diagnosed TMC and clinically node negative underwent thyroidectomy and prophylactic central lymph node dissection by TOETVA. The clinicopathologic characteristics, surgical outcomes, and cosmetic results were evaluated.
Results:
The mean age was 34.7 ± 8.5 years. Three patients had underlying Grave's disease. Thyroid lobectomy with isthmusectomy was performed in the majority of cases (72.4%). All patients underwent prophylactic central node dissection. The mean number of retrieved central node was 7.8 ± 3.7 (3–19). Seven patients (24.1%) had lymph node metastasis in postoperative pathology. Among them, the mean number of metastatic lymph nodes was 2.1 ± 1.7 (1–5). The mean operative time was 121.2 ± 22.6 minutes. Four patients experienced transient hoarse and 1 patient had hematoma. Visual analog scale score on first postoperative day was 2.8 ± 1.4 (0–5). Most of patients were satisfied with cosmetic outcome.
Conclusions:
The TOETVA is new technique for TMC in Vietnam. The initial results of oncology, postoperative complications, and cosmetic supported the application of TOETVA in TMC.
Introduction
According to GLOBOCAN 2018, thyroid cancer has become one of the most popular malignant diseases worldwide with ∼500,000 new cases per year. The incidence of thyroid cancer ranks ninth in both sexes, and fifth in females. 1 Thanks to neck ultrasound and fine needle aspiration application, the ability of early detection of malignant thyroid nodules is better, especially for thyroid microcarcinoma (TMC). 2 Thyroid lobectomy (TL) with isthmusectomy plus ipsilateral central lymph node dissection plays an important role in management of early thyroid carcinoma with low rate of both operative complications and local recurrence.3–7
Many surgical approaches have been applied for this procedure, including open thyroidectomy (OT), endoscopic thyroidectomy (ET), and robotic thyroidectomy (RoT).8–12 In which, ET could be performed through various approaches to move the scars to other parts of the body such as the axilla, breast, and postauricular areas or without cutaneous scars, but do not affect the treatment efficacy.13–15 Moreover, ET are more suitable for developing countries due to the suitable cost and facility requirement of robotic surgery.
The transoral endoscopic thyroidectomy by vestibular approach (TOETVA), which utilizes three ports on the lower lip, has been developed for TMC treatment worldwide, with low rate of complications and excellent oncological results.9–11 Compared to other approaches, TOETVA has its own advantages, including (1) easy access to thyroid gland and central lymph nodes, 10 (2) improvement of cosmetic outcome without an visible scar, 16 and (3) acceptable cost treatment. However, this approach has still not been frequently performed in Vietnam. Thus, in this study, we aim to demonstrate the applicability and safety of this technique in our current clinical practice.
Materials and Methods
Patients
TOETVA surgery was performed on 29 patients with TMC and clinically node-negative neck, which was defined as nodes detected during preoperative neck ultrasound or intraoperative period in Department of Oncology and Palliative Care, Hanoi Medical University Hospital. Preoperative work-ups included thyroid ultrasound, fine-needle aspiration biopsy (classification according to Bethesda 2017), and hormone level assessment. All patients underwent either total thyroidectomy (TT) or lobectomy, and central lymph node dissection.
Surgical procedure
Patients were placed in supine position with neck extended by a hard pillow under shoulder. All patients were administered general anesthesia with nasotracheal intubation.
Thyroidectomy
A 10-mm incision was made transversely and centrally at two-thirds of the distance between the inferior labial frenulum and the edge of the lower lip. A small mosquito was used to dissect the lower lip mucosa along with lower jawbone without lip muscle injury. Gorney suction elevator, 3 mm, was inserted through the incision with a solution of 0.1% adrenaline 1 and 500 mL of saline solution into the subplatysmal plane for hydrodissection. Thus, a 10 mm blunt-tip dissector was utilized for dilating the central incision and widening the operation space. A 10-mm trocar was then introduced through the incision with a 30° camera port.
CO2 was insufflated at 8–10 mmHg pressure with a flow rate of 3.5 L/minute through the 10-mm middle trocar. Two 5-mm trocars were then introduced through the lateral incisions and the three trocars converged at the midline. Afterward, a monopolar hook was utilized to complete the dissection, and the strap muscles were dissected through the middle line to deliver the thyroid gland into the working space. A 3/0 Vicryl silk was used to pull out the strap muscles laterally through a transcutaneous insertion. The pyramidal lobe was dissected first and continued inferiorly to divide the isthmus. The superior thyroid vessels were then identified and cut by a Harmonic scalpel. Lobectomy was completed from a cephalad to caudal direction and the recurrent laryngeal nerve (RLN) and the parathyroid glands were preserved. The procedure is repeated on the contralateral side in case of TT.
Central lymph nodes dissection
Central lymph node compartment was identified by hyoid bone (superior), brachiocephalic trunk artery (inferior), carotid artery (lateral), superficial layer of deep cervical fascia (anterior), and deep layer of deep cervical fascia (posterior). The key point of this procedure was to preserve the RLN. A harmonic scalpel was used to dissect along the RLN until the point where this nerve was downward into the chest. For the better exposure of the operative field, another transcutaneous silk was sutured to pull the strap muscle.
Retrieval of specimen and closing operative field
The thyroid and lymph node specimens were placed in an endobag and retrieved through the 10-mm trocar. After that, the operative field was cleaned by 0.9% saline solution. The strap muscles are closed by VLOC 3/0 suture. Incisions were closed by Rapid 4/0 suture. Drain was used only when hemorrhage was suspected in our procedure.
Postoperative management
A gauze pressure dressing was required under the chin until discharge. Intravenous antibiotics and methylprednisolone were administered for 7 days. Patients received a liquid diet on the day of surgery (day 0) and a soft diet the following days. The surgical drain would be removed if total liquid per day was less than 20 mL.
Results
A total of 29 patients were enrolled to this study. The clinicopathologic characteristics are presented in Table 1. The mean age of patients was 34.7 ± 8.5 years (range: 17–57 years) and the male-to-female ratio was 1:28. There were 3 patients (10.3%) with underlying Grave's disease. All patients had neck ultrasound to evaluate the thyroid tumors and metastatic lymph nodes. The mean tumor size was 6.5 ± 2.2 mm (range 3–10 mm). The location of tumor was in left side with 14 (48.3%), in right side with 9 (31%), in bilateral lobes with 3 (10.3%), and in isthmus with 3 (10.3%) patients. There were 19 cases (65.5%) with unifocal lesion, whereas multifocal tumors were detected in 10 patients (34.5%). Preoperative cytological diagnoses (according to Bethesda classification 2017) were malignant (VI), n = 13 (44.8%); suspicious for malignancy (V), n = 10 (34.5%), and atypia of undetermined significance (III), n = 6 (20.7%). Pathological findings showed that 26 patients (89.7%) were diagnosed with papillary thyroid cancer (PTC), 1 patient with follicular variant PTC, 1 patient was confirmed with follicular thyroid cancer, and 1 patient with noninvasive follicular thyroid neoplasm with papillary-like nuclear features. The mean number of harvested central lymph nodes was 7.8 ± 3.7 (range 3–19 nodes). Central compartment node metastases were found in 7 patients (24.1%). Among these patients, the mean number of metastatic lymph nodes was 2.1 ± 1.7 nodes (range 1–5 nodes). However, all metastatic nodes did not invade their capsular and their maximum size was less than 5 mm.
Clinicopathologic Characteristics
FTC, follicular thyroid cancer; FVPTC, follicular variant papillary thyroid cancer; MLN, metastatic lymph nodes; NIFTP, noninvasive follicular thyroid neoplasm with papillary-like nuclear features; PTC, papillary thyroid cancer; SD, standard deviation.
The surgical characteristics are shown in Table 2. In general, 21 patients (72.4%) had TL with isthmusectomy plus ipsilateral central node dissection (CND); 7 patients (24.1%) had TT plus bilateral CND; and only 1 patient had TL with isthmusectomy plus ipsilateral CND and contralateral tumor resection (CTR). The mean operation time of TT plus bilateral CND, TL with isthmusectomy plus ipsilateral CND, and TL with isthmusectomy plus ipsilateral CND and CTR was 144.3 ± 23.7, 113.9 ± 16.9, and 130 minutes, respectively. The estimated blood loss in the cases of TT plus bilateral CND was 17.5 ± 4.2 mL, in the TL with isthmusectomy plus ipsilateral CND group was 12.7 ± 3.9 mL, and in the patient TL with isthmusectomy plus ipsilateral CND and CTR was 20 mL. The length of hospitalization was 6.2 ± 1.4 days.
Surgical Characteristics
CND, central node dissection; CTR, contralateral tumor resection; SD, standard deviation; TL, thyroid lobectomy; TT, total thyroidectomy.
The postoperative complications are presented in Table 3. The transient hypocalcemia was recorded in 1 patient. The transient hoarse was presented in four cases (13.8%), which improved after 2 weeks. Besides, 3 patients had numb chin syndrome after surgery. After 14 days, these patients did not report any further submental numbness. Remarkably, 1 patient was detected with hematoma in the central compartment. Furthermore, other complications such as infection, seroma, Horner's syndrome, tracheal, and esophageal injuries did not occur in any patient. No case was converted to open surgery.
Surgical Outcomes
Patient's postoperative evaluations are shown in Table 4. The mean visual analog scale (VAS) value on 1, 4, and 7 postoperative day was 2.8 ± 1.4 (range 0–5); 0.7 ± 0.9 (range 0–2); and 0.1 ± 0.3 (range 0–1), respectively. All patients were highly satisfied with the surgical outcome.
Pain Score and Satisfactions
VAS score (0–10 integers).
SD, standard deviation; VAS, visual analog scale.
Discussion
Since the report of the first 60 cases of TOETVA with the low rate of complications by Anuwong, 17 many hospitals around the world have deployed this technique and reported their initial experiences.11,18–20 In previous reports, the TOETVA was more frequently applied to benign thyroid nodules than malignant tumors. In the largest published dataset of Anuwong, TOETVA plus CND was performed in only 26 cases of TMC. Nonetheless, the authors did not report the number of harvested lymph nodes. In addition, the report of Kim et al. in the 132 patients with TMC showed the possibility to apply widely the TOETVA for TMC. 9 To prove the feasibility and safety of TOETVA in TMC, Ahn and Yi directly compared TOETVA with OT in a single-surgeon series of 150 cases. 21 In this study, the surgical and oncological outcomes were similar between the two groups. The initial successful results of mentioned reports encouraged us to perform this study. Our study included the first 29 patients of TMC who underwent TOETVA plus prophylactic CND in Vietnam.
Thyroid cancers with suspicious capsular invasion or clinical lymph node metastasis were associated with increased risk of local recurrence and were excluded from this study. Besides, due to the high rate of the occult metastasis of central lymph nodes (∼45.1% according to Quang et al.), prophylactic central lymph node dissection was performed in all patients. 7
Among 29 patients, only three TMC cases (10.3%) were previously diagnosed with Grave's disease, who had TT plus bilateral CND without postoperative bleeding, permanent RLN, and hypoparathyroidism. Nonetheless, the mean time operation was significantly longer in these 3 patients (153 ± 21.6 minutes) compared to the others (117.5 ± 19.8 minutes). The difference came from hypervascularity, firmness, and enlargement of the whole thyroid gland. In fact, the largest volume of thyroid gland in this study was about 22.3 mL, higher than the mean volume of thyroid gland for females, which is ∼5.78 ± 1.96 mL. 22 According to Jitpratoom, TOETVA was a feasible and safe treatment for Graves' disease in comparison to OT. 23
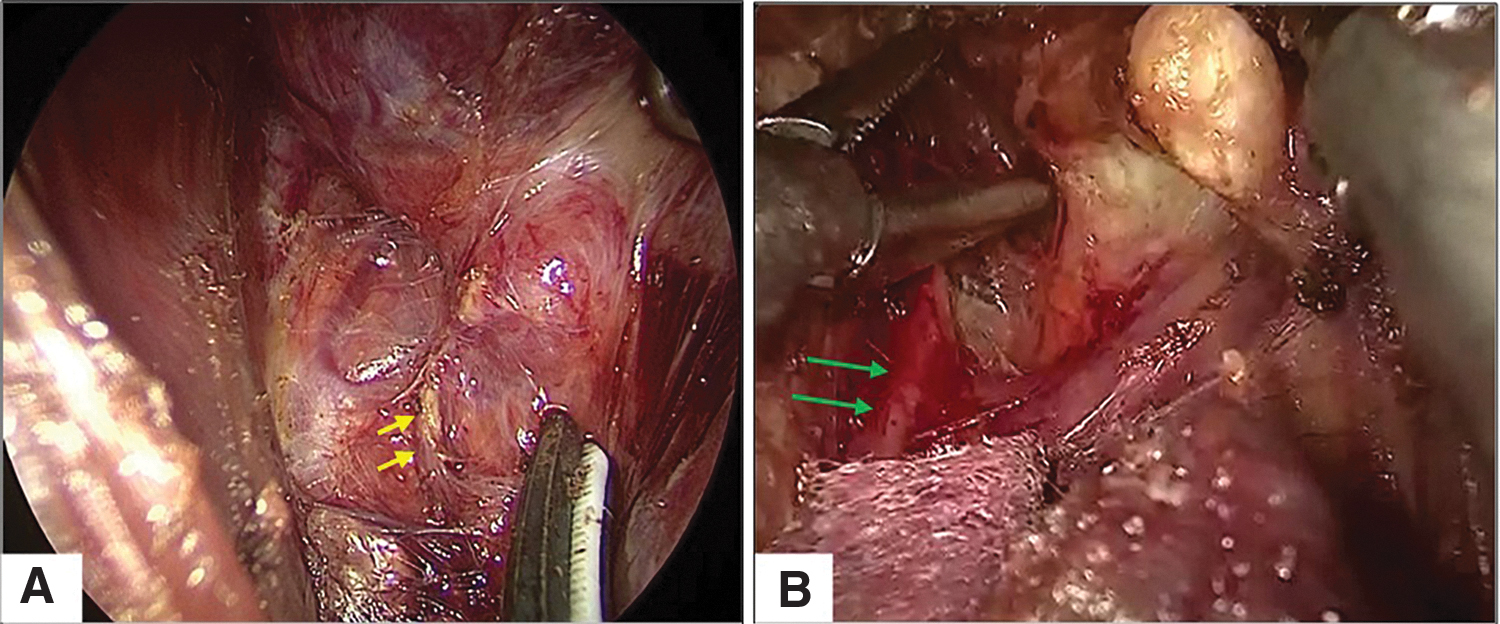
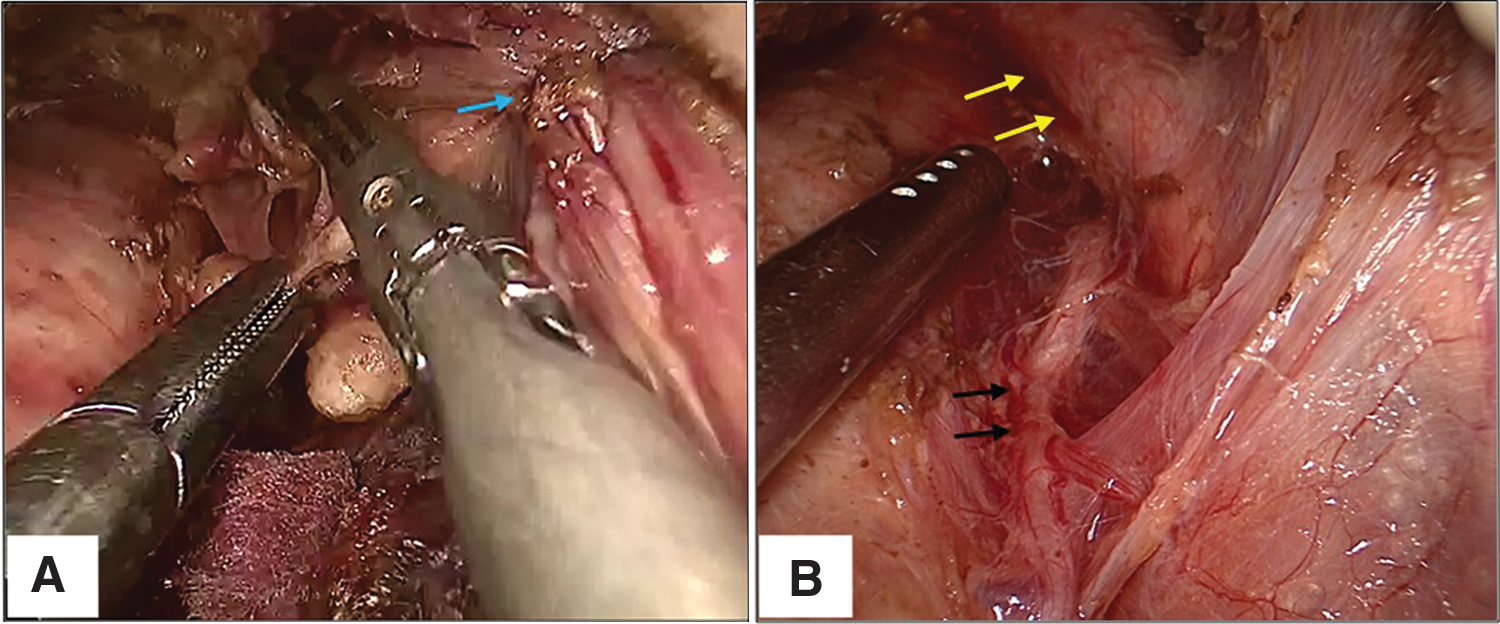
One of the advantages of TOETVA is the ability to dissect the central lymph nodes along the boundaries of central compartment (Figs. 1 and 2). In the first reports of Anuwong, the author enlarged the central compartment by inserting a silk passed transcutaneously into the working space and put around the strap muscles with the laparoscopic instruments. 16 In another report of Kim, the author used a retractor device, which could be freely shifted between the layers of strap muscle. 9 However, in our clinical practice, we found that two transcutaneous silks on the one hand also enlarged the central compartment, and on the other hand, laterally presented central neck compartment more easily (Fig. 2). Therefore, the ipsilateral carotid artery could be clearly showed. In our study, the two 3/0 Vicryl silks were inserted at different times. The first silk was inserted after dissecting the strap muscles and near the superior pole of thyroid gland. Meanwhile, the second silk was inserted before lymph node dissection and near the inferior pole of thyroid gland. Remarkably, anterior jugular vein could be injured during transcutaneous insertion. In fact, the mean number of retrieved central nodes was 7.8 ± 3.7 (3–19), which was higher than the number reported in previous studies. According to Ahn, the number of harvested central neck lymph nodes in TOETVA was 3.67 ± 3.05, 21 which was similar to OT group (5.03 ± 3.99 nodes). As reported by Kim, this number was 2.6 ± 2.2 (1–12) nodes. 9 In another study, Kim reported a mean of 5.0 ± 3.6 retrieved lymph nodes per patient by transoral robotic thyroidectomy (TORT). 24 Other than mentioned methods, the lymph node dissection was also performed by the transaxillary approach RoT (TAA RoT) and bilateral axillo-breast RoT (BABA RoT). In general, the number of lymph nodes that were harvested by TAA RoT and BABA RoT varied among different reports 25 : the lowest value was 4.4 ± 2.1 (Lee et al. 26 ) and the highest value was 8.7 ± 5.1 (Kim et al. 27 ). In brief, the central lymph node dissection of TOETVA was comparable to TORT, TAA RoT, and BABA RoT, while, the dissection of the subplatysmal plane of TOETVA was less extensive than unilateral axillo-breast approach (UABA), BABA, or RoT techniques. The operative time in this study was comparable with Ahn's study (110.26 ± 35.74 minutes).
We encountered four cases (13.8%) with transient hoarseness, which was slightly higher compared with Ahn and Yi 21 (4.7%) and Kim et al. 9 (4.5%). However, all cases fully recovered within 14 days after the surgery. This may again be related to the learning curve of the surgeon. The transient RLN injury rate might be reduced by more meticulous dissection and avoiding thermal injury from harmonic scalpel. 11 After performing initial cases, we started to use a wet endoscopic gauze to reduce the heat from the harmonic scalpel, while dissecting the RLN, which improved the rate of transient postoperative hoarseness. The rate of transient hypoparathyroidism in our study was 3.4%, which was comparable to Ahn's study in TOETVA group (3.3%). The rates of transient hoarse and hypoparathyroidism in our study were lower than in the OT technique.28,29 Our study illustrated a 10.3% incidence of numb chin. To limit the rate of mental nerve injury, it is necessary to identify mental foramen. Based on Kqiku's report, the frequent position of mental foramen was between the first and second mandibular premolars. 30 Therefore, the position of the 5 mm trocar should be behind the sagittal line located between the first and second mandibular premolars. The 5 mm trocar was parallelly inserted with this line and passed over the lower border of mandibular. Then, this 5-mm trocar was directed to the middle line. In addition, another cause of mental nerve injury was the usage of electric cautery for bleeding control at the lateral port site, which could stop spontaneously without electric cautery. 9 In this study, we encountered only 1 patient (3.4%) with postoperative hematoma. However, the patient did not have symptoms of airway obstruction (e.g., dyspnea, stridor, and hypoxia), and no intervention was necessary. The hematoma disappeared after 30 days on neck ultrasound. Other complications such as tracheal and esophageal injuries or infection did not occur in our patients.
Patients in the TOETVA had lower VAS score on 1st, 4th, 7th day than those in UABA, 8 because the flap dissection of TOETVA is less extensive compared with UABA, BABA, or RoT techniques. In general, most patients were highly satisfied. The satisfactions in TOETVA group were slightly higher than those in UABA group 8 because the traditional endoscopic approach still left a small scar outside the neck zone (Fig. 3).

Postoperative outcome after TOETVA. TOETVA, transoral endoscopic thyroidectomy by vestibular approach.
Conclusion
The TOETVA is a new technique for TMC in Vietnam. The initial results of oncology aspect, postoperative complications, and cosmetic outcome supported the use of TOETVA in TMC.
Footnotes
Acknowledgment
We really appreciate the help of our colleagues in Hanoi Medical University Hospital with our project.
Ethics Approval and Consent to Participate
The study was approved by our research committee in Hanoi Medical University Hospital. These patients have been provided with sufficient information about this publication.
Consent for Publication
Both patients provided written consent for the case details and accompanying images to be published.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.