
Abstract
Although >10% of surgical patients receive alternative antibiotic prophylaxis for reported penicillin allergies, it is estimated that <20% of such cases represent true allergies that preclude standard prophylaxis. Each antibiotic class has a distinct impact on the intestinal microbiota and on postoperative metabolomics. The community structure and function of the microbiota are linked to the ability to lose weight after bariatric surgery. This study demonstrates differential weight loss after laparoscopic sleeve gastrectomy between patients who received standard (cefoxitin) and alternative (levofloxacin and metronidazole) perioperative prophylaxis. Multivariate analysis demonstrates that alternative prophylaxis is significantly and independently associated with diminished postoperative weight loss.
Introduction
The pathogenesis of obesity and the biology of its surgical treatment are multifaceted. Patients with similar demographics can undergo identical operations and experience vastly dissimilar postoperative weight loss. Alterations to the intestinal microbiota are linked to both the development of obesity and the inability to lose weight, and may explain such differences. 1 Surgical trauma and the stress of the perioperative period induce durable changes to the microbiota. 2 Antibiotic-induced alterations to the intestinal microbiome are significant, highly dependent on drug class, and last up to a year after a single dose. 3 Human studies and animal models demonstrate that sleeve gastrectomy durably alters the microbiota throughout the intestinal tract, and the long-term trajectory of the microbiota is particularly sensitive to the class of perioperative antibiotic utilized.1,4
Over 10% of surgical patients receive alternative prophylactic antibiotic regimens due to reported penicillin allergies, despite evidence that <20% of such reports represent true allergies. 5 Alternative regimens necessarily change the class of antibiotic administered, and thus the microbial coverage of the regimen. Retrospective studies have linked alternative prophylaxis to divergent community structure of the microbiome, and altered glucose metabolism after Roux-en-Y gastric bypass.6,7 A rodent model demonstrated that preoperative exposure to antibiotics diminished weight loss in a manner dependent on drug class after sleeve gastrectomy. 8
Taken together, these findings suggest that perioperative antibiotics alter the biology of the gut in a lasting manner that is highly dependent on the class of antibiotics used. To our knowledge, the impact of alternative antibiotic regimens on weight loss after sleeve gastrectomy has not been investigated. Using insights derived from the mentioned studies, we designed a retrospective analysis of weight loss after sleeve gastrectomy stratified by the class of antibiotics given perioperatively.
Materials and Methods
This study is a retrospective review of electronic medical records in a case–control format. After approval by the institutional review board of Rush University Medical Center (RUMC), data were collected with the assistance of the Rush Bioinformatics and Biostatistics core facility. Patients were identified using current procedural terminology coding. Exposure to antibiotics was determined through electronic orders and pharmacy records. Patients undergoing sleeve gastrectomy at RUMC between 2014 and 2018 were included. Patients <18 years, those with prior weight loss operations, and those who had any exposure to antibiotics for any reason in the 6 months before or after the date of surgery were excluded.
On the day of surgery, all patients received either standard antibiotic prophylaxis (CEF—cefoxitin 2 g intravenous (IV), q8 hours, 2 total doses) or alternative prophylaxis due to a penicillin allergy (L/M—levofloxacin 500 mg IV once and metronidazole 500 mg IV once). Operative technique and bougie size were standardized and all cases were performed laparoscopically. Patient demographics and perioperative outcomes data were collected. Body mass index (BMI) recorded during any visit during the postoperative period was included. BMI recorded at the first follow-up clinic visit (2 weeks), 180 ± 60 days (6 months), and 365 ± 90 (12 months) days postoperatively were used for analyses. If multiple visits occurred in any of the mentioned windows, the average value was used and the average length of follow-up calculated.
Comparisons of weight loss between groups were made using change in BMI (ΔBMI) from the day of surgery. Standard comparative statistics, either two-tailed unpaired t test or Fisher's exact test, were calculated using GraphPad Prism Software, version 8.3.1. Multivariate linear regression models were used to assess factors that may be independently associated with degree of weight loss (lbs.) after bariatric surgery at both 6- and 12-month intervals. The data were analyzed using R statistical software (version 4.0, 2020).
Results
Five hundred and two patients were identified; after exclusions, 390 remained. Three hundred forty-six patients received CEF, while 44 received levofloxacin and metronidazole. Demographics including age, gender, preoperative BMI, and American Society of Anesthesiologists (ASA) classification were not significantly different between groups. Loss to follow-up and average duration of follow-up were similar at all time points (Table 1).
Baseline Demographics and Follow-Up in Patients Undergoing Laparoscopic Sleeve Gastrectomy
ASA, American Society of Anesthesiologists; BMI, body mass index; SD, standard deviation.
Two weeks after surgery, ΔBMI in patients receiving CEF was 2.62 kg/m2 with a standard deviation of 1.48, compared with 2.30 ± 0.9 kg/m2 in the L/M group (P = .17 student's t-test). Six months after surgery, ΔBMI was 8.24 ± 2.74 kg/m2 in the CEF group versus 6.49 ± 2.85 kg/m2 in L/M group (P = .001). Twelve months after surgery, ΔBMI in CEF group was 9.53 ± 4.20 versus 7.74 ± 4.21 in L/M group (P = .024) (Fig. 1).
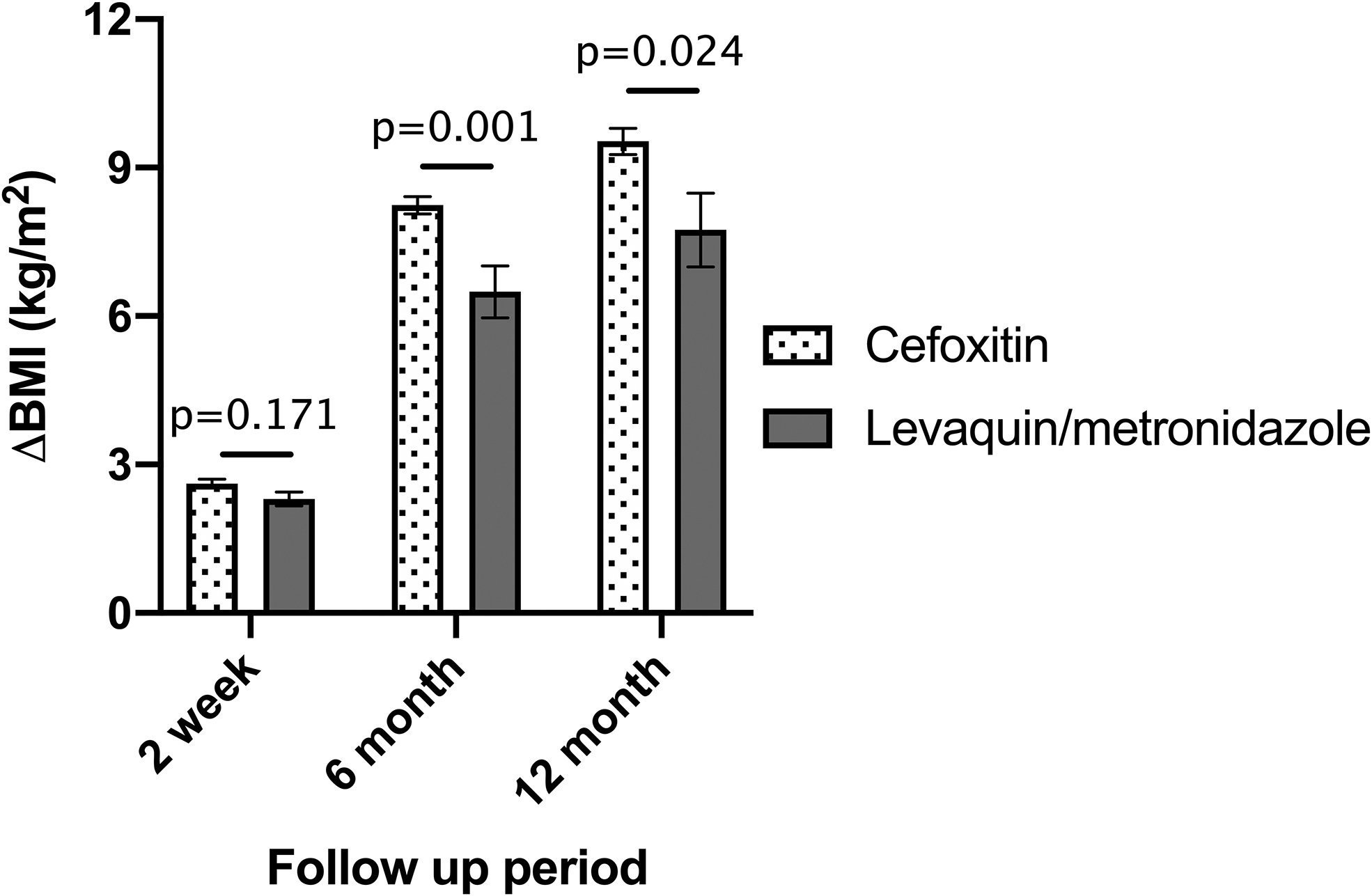
Weight loss after sleeve gastrectomy differs between patients receiving standard and alternative perioperative antibiotic prophylaxis. Error bars indicate standard deviation.
To determine the demographic factors that were independently associated with differential weight loss, multivariate analysis was performed. Alternative antibiotic prophylaxis was significantly and independently associated with diminished weight loss at 6 months. By 12 months postoperatively, the effect trended toward but did not reach significance. Age >50 years was the only other factor negatively associated with postoperative weight loss (Fig. 2).
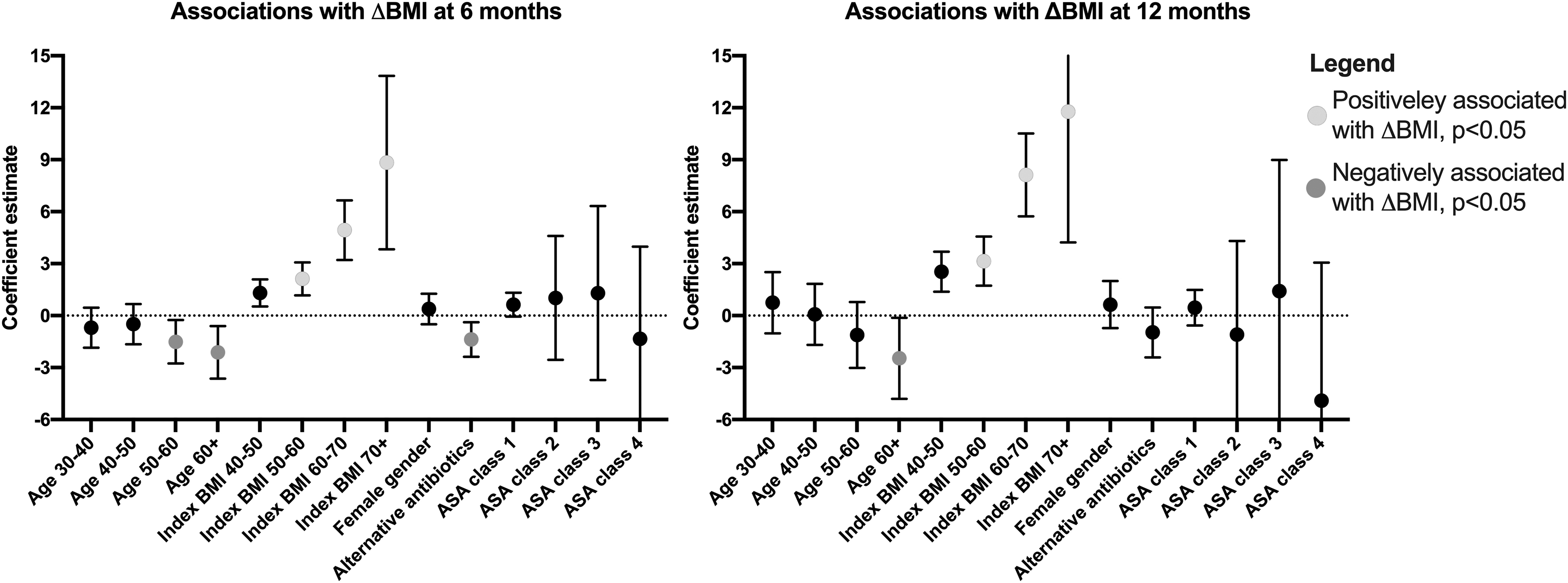
Multivariate linear regression of patient factors associated with postoperative weight loss. Alternative antibiotic prophylaxis was independently associated with diminished weight loss at 6 months postoperatively.
Discussion
Our data indicate that by 6 months postoperatively, patients who received alternative prophylaxis at the time of surgery experienced significantly less weight loss than those who received the standard regimen. This trend persisted at 12 months postoperatively. On multivariate analysis, as expected, higher index BMI was independently associated with increased postoperative weight loss. Age >50 years was negatively associated with postoperative weight loss, consistent with prior study. 9 Alternative prophylaxis was independently associated with diminished weight loss at 6 months, but the independent effect was lost at 12 months. Demographics were similar between groups, whereas rates of penicillin allergy and loss to follow-up rates were similar to those of previously published work. 10
Observations from this study suggest a role for antibiotic-induced dysbiosis in weight loss after sleeve gastrectomy. Although there is overlapping coverage between the two regimens utilized, levofloxacin and metronidazole have significantly broader gram negative coverage than CEF alone. 11 Weight loss after bariatric surgery has been clearly linked to neurohormonal changes, genetics, diet, and more recently the composition of the intestinal microbiome. The impact of prophylactic antibiotic class has been studied exhaustively in the prevention of surgical site infection; however, the “off target” effects of antibiotic prophylaxis in bariatric surgery are only beginning to come to light.
This retrospective study was designed as hypothesis-generating work. The study is limited to a year of follow-up as longer term data were not available in our data set. Further investigation is indicated to (1) confirm our findings in a long-term prospective multi-institutional setting and (2) investigate the impact of standard and alternative perioperative antibiotic regimens on the colonic microbiome in humans. The intestinal microbiota is a significant and targetable factor that impacts outcomes on many fronts after gastrointestinal surgery. Given the low rate of true allergy among patients with reported penicillin allergy, consideration should be given to the described strategies that promote the use of standard antibiotic prophylaxis, such as preoperative beta-lactam allergy screening.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.