
Abstract
Background:
Laparoscopic sleeve gastrectomy (LSG) is the most common bariatric procedure, but it had been reported to increase the incidence of gastroesophageal reflux disease (GERD) and its consequences. Some surgeons tried to decrease that by routine hiatal dissection with hiatus hernia (HH) repair. But, hiatal dissection with HH repair is considered an important risk factor for the newly emergent complication of intrathoracic sleeve migration (ITSM). We proposed a new hiatal repair technique, which is expected to improve GERD without increasing the potential for ITSM. This study aims to evaluate the results of this technique.
Methods:
A prospective observational study was performed at the Ain Shams University Hospital between January 2016 and December 2019. It included patients with morbid obesity and one of the following: Clinical manifestations of GERD with endoscopic evidence of HH/laxity or esophagitis. Asymptomatic HH/laxity. LSG combined and HH repair with anterior phrenoesophageal ligament (PEL) preservation was performed for all patients. Patients were followed up for 12 months. Patients were evaluated after 1 year with an upper gastrointestinal (GI) endoscopy.
Results:
Thirty-two patients were enrolled in our study. After 1 year, the mean excess weight loss was 63% ± 23%. The mean GERD health-related quality of life (GERD-HRQL) score dropped to 12 ± 8. GERD-HRQL scores improved in 25 of documented esophagitis patients, worsened in 2, and did not change in 2 patients. Endoscopy showed a decrease in rate and degree of esophagitis (from 28 [87.5%] preoperatively to 8 [25%] patients after 1 year of follow-up). The improvement was better in patients with grade A and B esophagitis. Two patients were converted to gastric bypass due to persistent intractable GERD symptoms with grade C esophagitis despite medical treatment. No cases of ITSM were detected.
Conclusion:
Anterior PEL preserving HH repair combined with LSG is a safe and feasible technique that can control GERD manifestations without interference with the technique or outcome of LSG.
Introduction
Obesity is a known significant independent risk factor for gastroesophageal reflux disease (GERD) and hiatus hernia (HH). The incidence of HH increases with body mass index (BMI). 1
In 1998, the first laparoscopic sleeve gastrectomy (LSG) was performed as a component of Hess's biliopancreatic diversion with duodenal switch. 2 Since then, LSG has become very popular among surgeons as a stand-alone procedure with good long-term results. The main advantages of LSG are that it does not imply any type of anastomosis, maintaining gastrointestinal tract continuity, and it is an effective and safe and procedure when compared with Roux-en-Y gastric bypass (RYGB). 3
Laparoscopic RYGB is one of the most performed operations for morbid obesity and also controls symptoms and complications of GERD. 1 However, LSG is the most commonly performed procedure among bariatric surgeons in the Middle East region. This is mostly due to its simplicity and patient's preference. 4
It was proposed by some authors that reflux symptoms are supposed to improve after LSG due to weight loss and decrease in acid production. Others proposed the opposite, as LSG induces an alteration of gastroesophageal junction, increases intragastric pressure, and divides gastric sling fibers, hence inducing GERD. 5 A recent multicenter study from France to Italy, showed that the prevalence of GERD symptoms, erosive esophagitis, and the usage of proton pump inhibitors (PPIs) increased from 22%, 10%, and 22% before the LSG to 76%, 41%, and 52% at the time of follow-up. Moreover, the prevalence of Barrett's esophagus was 18.8% at 5 years follow-up after LSG. 6
Some surgeons tried to decrease the negative impact of LSG on GERD by routine aggressive complete hiatal dissection with concomitant HH repair even small ones. Intrathoracic sleeve migration (ITSM) is a rare complication after LSG that has been inconsistently addressed in the literature. It had been reported that preoperative GERD, central obesity, and concomitant aggressive HH repair during LSG are associated with ITSM development. 7
Our team had proposed a new modified hiatal repair technique during LSG, which is expected to improve GERD problem without having the potential to increase risk for future ITSM. This study aims to evaluate the initial results of this technique.
Patients and Methods
Our study was a prospective observational study performed at the Ain Shams University Hospital between January 2016 and December 2019. It included 32 patients with morbid obesity and concomitant GERD and/or hiatus hernia.
Our inclusions criteria were: patients with BMI ≥40 kg/m2 or ≥35 kg/m2 with obesity-related comorbidities plus one of the following: Clinical manifestations of GERD with endoscopic evidence of HH or hiatal laxity with esophagitis. Asymptomatic HH proved by endoscopy (our rationale for crural repair in these patients is to lower the possibility of de novo GERD). The following patients were excluded from the study: Patients with history of previous gastric, bariatric, or antireflux surgery. Patients with documented Barrett's esophagitis (as our institution's policy only offers RYGB for these patients). Patients with BMI >65.
The choice of LSG with cruroplasty rather than gastric bypass was based upon direct discussion between the surgeon and the patient exploring different aspects of each procedure. All patients were required to sign an informed consent before operation. The Ain Shams University Hospital's Ethics Committee (IRB) approval was received before the start of the study.
All patients underwent upper gastrointestinal (GI) endoscopy with assessment of the presence of HH and esophagitis. Subjective assessment of GERD symptoms using the GERD health-related quality-of-life (GERD-HRQL) score was done for all patients before surgery.
Surgical technique
All operations were performed under general anesthesia and by laparoscopic approach using the French technique (the surgeon standing between the patient's legs). The patient was put in supine position with reverse Trendelenburg tilt by 30° and with legs apart and pneumatic intermittent pressure stocking in place. Each procedure required 5 trocars. The first trocar was an optical trocar inserted 2 hand breadths below the xiphisternum and pneumoperitoneum was induced at a pressure of 15 mm Hg.
The operation was started by freeing the greater curve of the stomach from the omentum using the Ligasure 5 mm (Medtronic, Inc., Minneapolis, MN), starting 4 cm from the pylorus until the left crus, and any evident hiatus hernia was reduced at this stage by blunt dissection. Then, the left crus was dissected downward to the angle with right crus, keeping in mind not to injure the left gastric vessels, and this was facilitated by pushing of the esophagus anteriorly. The right crus was then followed upward by dissecting it from the mesogastrium, and this step was facilitated by cutting peritoneal reflection from right crus to esophagus through the pars flaccida (Fig. 1A).

The esophagus was then mobilized mainly from its posterior aspect to add more intra-abdominal length. As the phrenoesophageal ligament (PEL) bridges the space between the hiatal margin and the esophagus forming a circumferential continuation of fascia transversalis and endothoracic fascia, only the posterior/lateral aspects of the ligament were dissected in the operation to clearly expose both crura. The anterior aspect of PEL, pars condensa, and any accessory hepatic arterial or vagal branches were preserved (Fig. 1B). Posterior cruroplasty was performed using 2–3 Ethibond (Johnson-Johnson, Inc., New Brunswick, NJ) 2.0 interrupted sutures (Fig. 1C, D).
In cases of laxity of anterior part of PEL, or in cases where a hiatal defect is seen anteriorly, this technique continues to be valid. The sloping oblique nature of the crura will allow forward mobilization of the esophagus, together with increasing the intra-abdominal length of the esophagus and posterior cruroplasty, all of which will correct any laxity or hiatal defect seen anteriorly (Fig. 2). After that, a standard sleeve gastrectomy was performed over a 36 French calibration tube using an Endo GIA stapler with 60 mm tristaple loads.

A case of anterior crural defect managed posteriorly with preservation of anterior part of PEL. PEL, phrenoesophageal ligament.
Postoperatively, patients were allowed to drink at day 1 and PPIs were stopped after surgery. Patients were regularly followed up at 1, 6, and 12 months after discharge. At each visit, the percentage of excess weight loss (EWL) together with subjective symptoms of GERD using the GERD-HRQL score, were done and compared with the preoperative score, together with any need for antireflux treatment. Patients were also evaluated after 1 year with an upper GI endoscopy. All preoperative data, including patients' characteristics (age, gender, weight, BMI, and comorbidities); operative data, including operative time and complications; and postoperative data, including length of hospital stay, complications, and reoperation were collected.
Results
Thirty-two patients were enrolled in our study. No patients were excluded after selection. All included patients had confirmed HH/laxity in endoscopy. Four of these patients had HH without esophagitis, while the remaining patients had various degrees of esophagitis according to the Los Angeles classification (Grade A: 18 cases, Grade B: 6 cases, and Grade C: 4 cases). The general preoperative characteristics are shown in Table 1 and Figure 3.
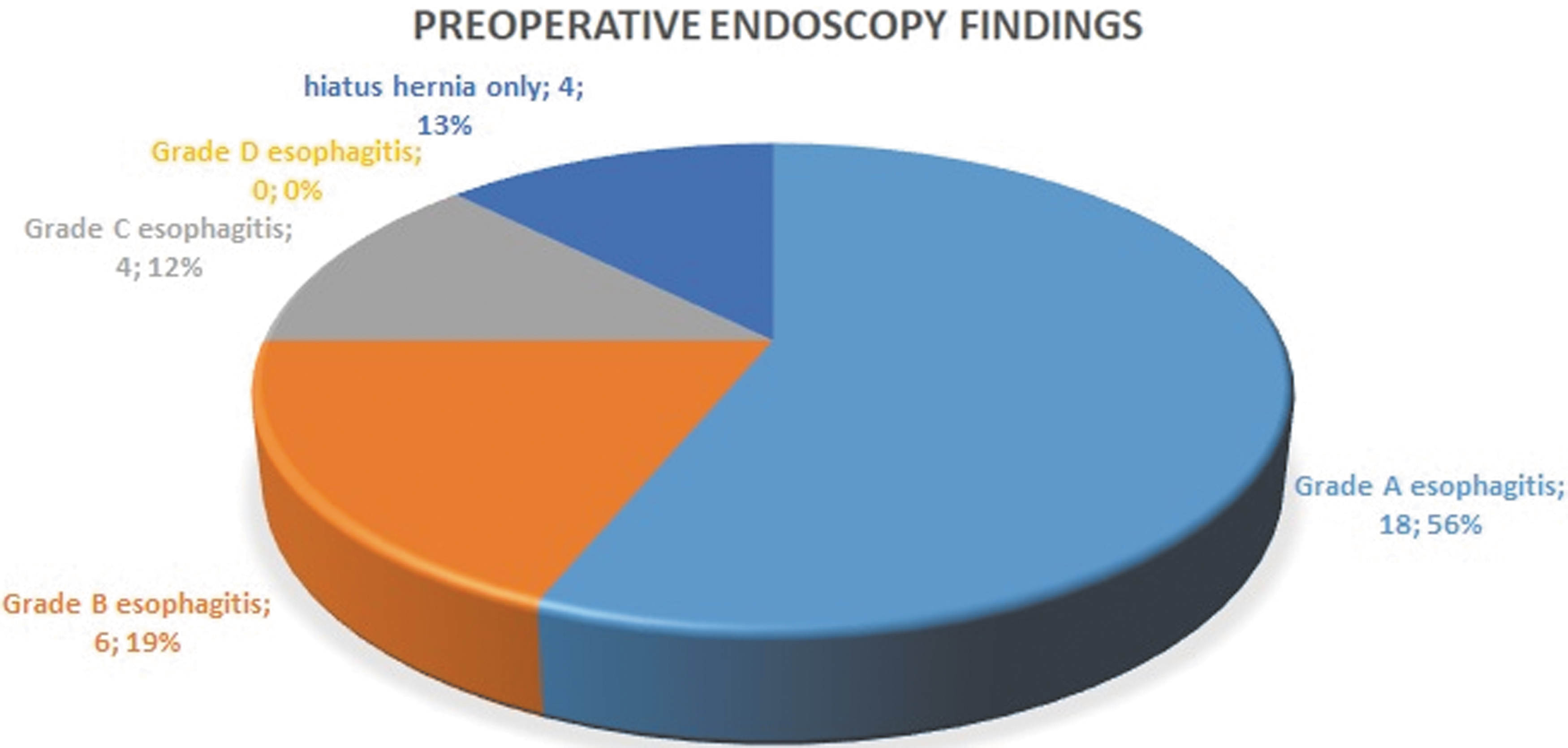
Preoperative endoscopy findings according to Los Angeles classification.
Preoperative Characteristics of the Study Group
BMI, body mass index; GERD-HRQL, gastroesophageal reflux disease health-related quality of life.
The mean operative time was 45 ± 9 minutes with no cases of conversion to open surgery. We were able to do a successful hiatal repair using the new technique in all patients. One patient had significant postoperative staple line bleeding that was managed conservatively. No cases of dysphagia were recorded during the follow-up period. No ITSM or any other surgical complication was recorded during the follow-up period. All patients were sent home on the second or third postoperative day.
After 1 year of follow-up, the mean EWL was 63% ± 23%, and the mean BMI was 29 ± 5 kg/m2. The mean GERD-HRQL score dropped significantly from 45 ± 13 before the operation to 12 ± 8 after 1 year of follow-up (Fig. 4). GERD-HRQL scores improved in 25 of documented esophagitis patients and worsened in 2 of grade C esophagitis patients. Two patients with Grade A esophagitis had practically no change of their GERD-HRQL scores (Fig. 5). Follow-up endoscopy showed a decrease in rate and degree of esophagitis among patients of the study group.
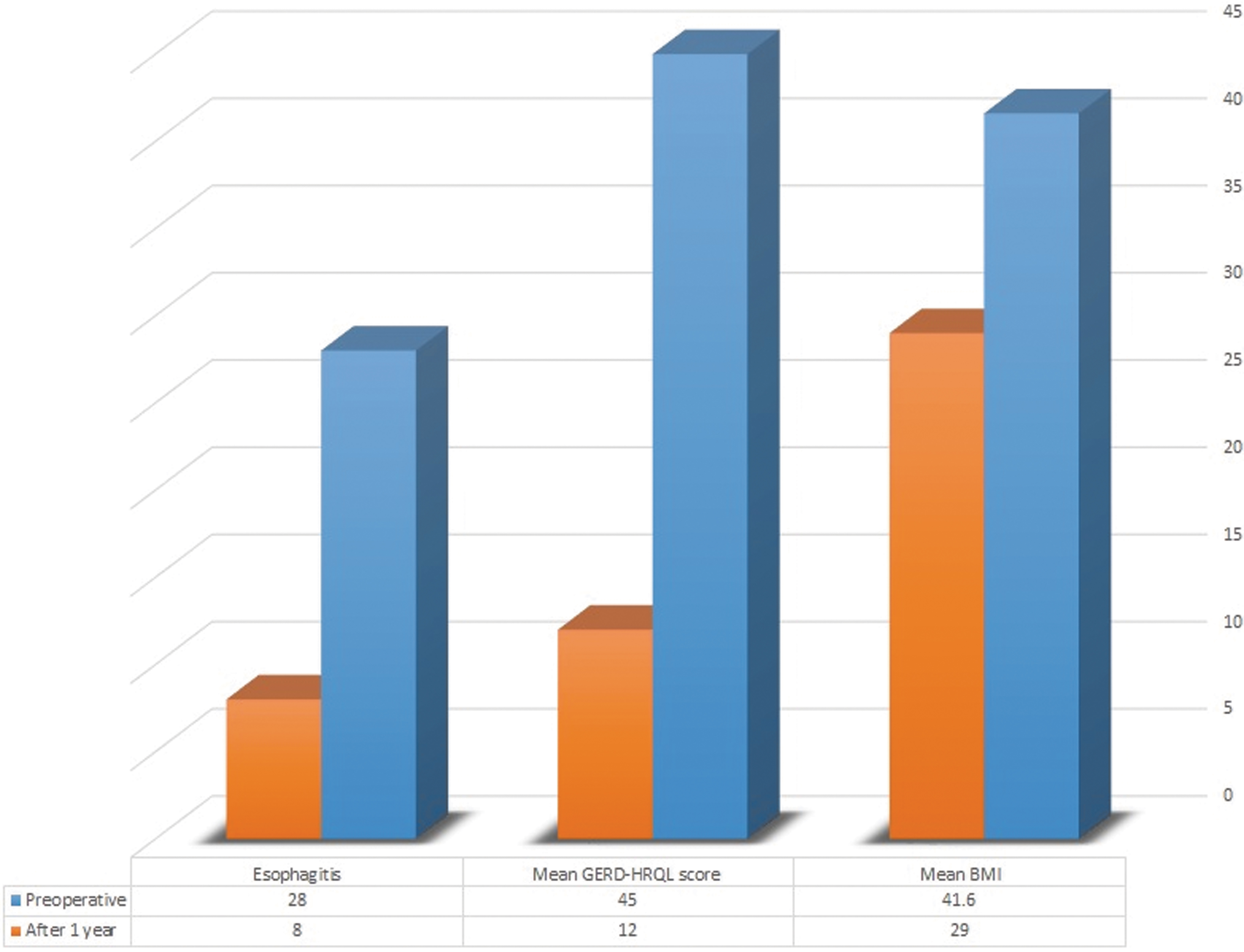
One year follow-up results.

GERD-HRQL scores after 1 year. GERD-HRQL, gastroesophageal reflux disease health-related quality of life.
The overall number of patients with esophagitis decreased from 28 (87.5%) preoperatively to 8 (25%) patients after 1 year of follow-up. Patients with grade A and B esophagitis had better response than those with grade C. Out of 18 patients with grade A esophagitis, 16 patients (88.9%) improved to have no esophagitis. Out of 6 patients with grade B esophagitis, 2 patients improved to have grade A esophagitis and rest of the patients (66.7%) improved to have no esophagitis. One of grade C esophagitis patients improved to grade A and the other to grade B esophagitis. The remaining two grade C patients who had persistent intractable GERD symptoms on maximum dose of PPIs with esophagitis on endoscopy after 1 year follow-up, gastric bypass was offered for both. Neither Barrett's esophagitis nor de novo esophagitis or recurrent HH was found in any patient that had undergone endoscopy after the follow-up period (Fig. 6).
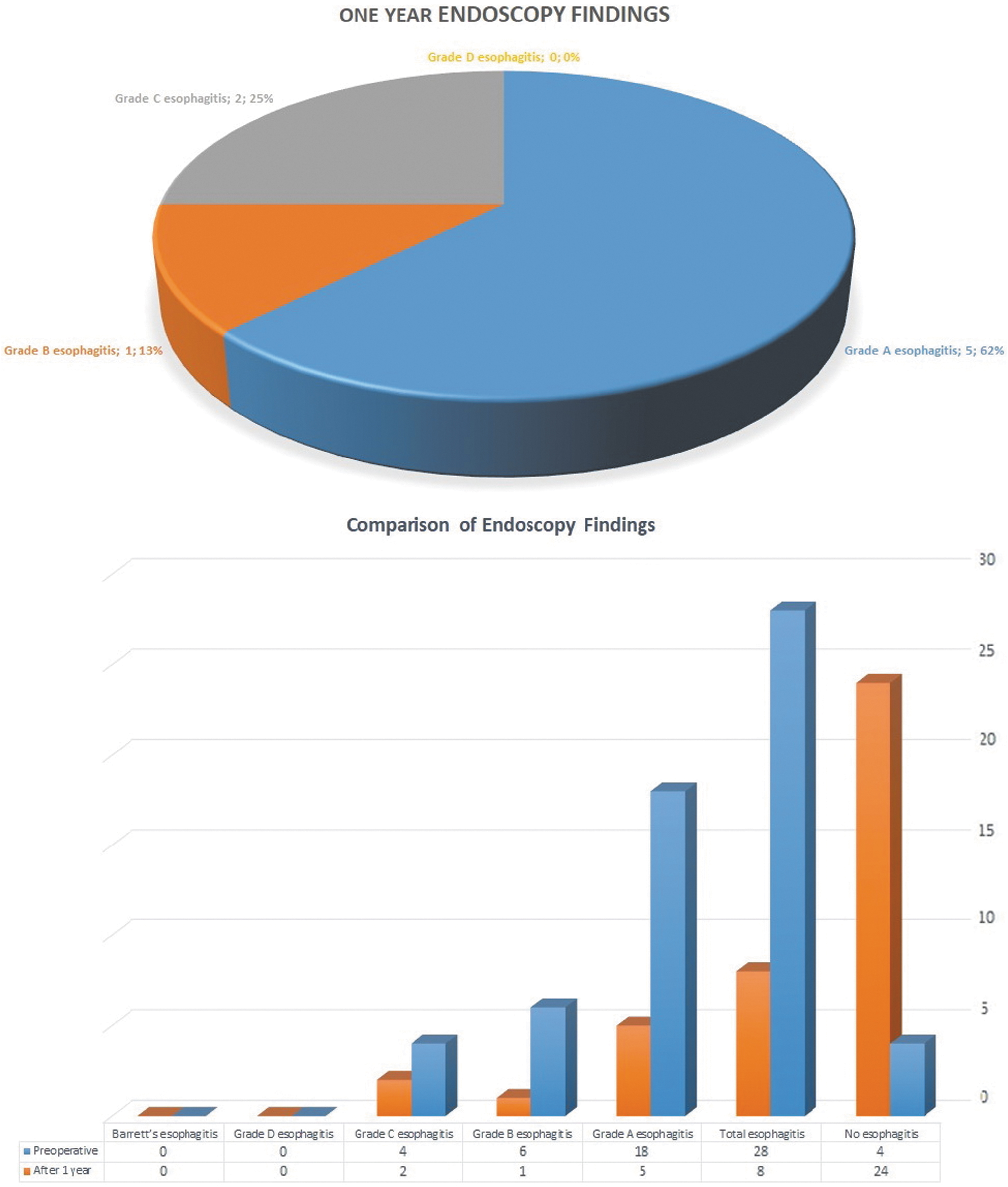
Endoscopy findings after 1 year and their comparison with preoperative endoscopy.
No other cases of reoperation were detected during the follow-up period. No patients were lost during the follow-up period.
Discussion
Both GERD and HH are highly prevalent among the morbidly obese population with prevalence rates ranging from 39% to 61% for GERD. 8
In the past, many surgeons prefer to avoid performing sleeve gastrectomy in patients with GERD especially if a large hiatal hernia is present. This practice had seen some changes recently with more surgeons performing hiatal hernia repair concomitant with sleeve gastrectomy. Their rationale for doing so is that the repair of the HH helps in amelioration of GERD symptoms and prevents new onset of GERD. 9
Many options have been proposed as a solution to address GERD with LSG, such as performing a modified Nissen fundoplication, performing cruroplasty alone, utilizing the Linx device, and performing cruroplasty with reinforcement using synthetic or biologically derived material. All of these options include complete hiatal dissection and severing of PEL, which may predispose to intrathoracic migration and jeopardize partially the antireflux mechanisms by disrupting that complex. 10
The PEL has been considered an important contributor to gastroesophageal competence. Although the mechanism responsible for gastroesophageal competence remains controversial, available evidence suggests an important role for the inferior esophageal sphincter. The PEL is considered to be an important component of this sphincter. 11 It is highly suggested that the PEL serves to prevent the superior displacement of the esophagus into the thoracic cavity by drawing it down by its elastic recoil. 12 Smith et al. demonstrated that the primary etiology of the sliding HH is thought to be degeneration of the PEL. 13
Our team proposed a modification to the technique of hiatal repair during LSG, which works through preserving the anterior part of the PEL, to decrease GERD without predisposing to ISTM. Furthermore, we believe that weight loss induced by the LSG would lower the abdominal pressure and the chance of HH recurrence. This study was done to evaluate these assumptions.
All cases were successfully completed laparoscopically without conversion, in a reasonable operative time and with low perioperative morbidity comparable to standard LSG. This proves that successful hiatal repair is feasible and safe through posterior approach to the hiatus preserving the PEL.
The recorded 1 year EWL (63%) in our study was satisfactory and compares well to our standard LSG patients and is comparable to the published literature. The meta-analysis done by Fischer et al., involving 123 articles describing 12,129 patients had shown the EWL percentage after 12 months to range from 30% to 83.3% with a mean of 59%. 14 This shows that our technical modification did not jeopardize the efficacy of sleeve gastrectomy as a bariatric procedure.
After 1 year of follow-up, the mean GERD-HRQL score had dropped significantly from 45 to 12. Also the rate and severity of esophagitis had significantly decreased (from 87.5% to 25%). Only 2 patients had persistent intractable GERD symptoms on maximum dose of PPIs and grade C esophagitis after 1 year follow-up; for such patients with severe peptic esophagitis, we recommend gastric bypass from the start. These results show a good antireflux effect of the procedure, which is comparable to previously published data.
Soricelli et al., reported significant improvement of GERD symptoms after LSG with concomitant HH repair. They described repair of a posterior crural defect with two interrupted nonabsorbable sutures, approximating the right and left diaphragmatic pillars. HH repair was shown in their study to be feasible and safe with no postoperative complications related to the procedure. The authors suggested that approaching the diaphragmatic crus from the left reduced damage to the anterior vascularization of the esophagogastric junction, which, if impaired, could be involved in the development of staple-line leaks. In addition, they showed that the postoperative development of de novo GERD was significantly greater in patients who did not undergo HH repair compared with those with HH repair (22.9% versus 0%). 15
Soliman reported favorable results in 20 patients who had concomitant LSG and a posterior crural repair. Thirteen patients reported resolution of GERD symptoms and five reported improvement leading to minimal doses of PPIs at a mean follow-up of 7 months. 16 Gibson et al., analyzed the results of LSG and HH repair in 500 patients. An anterior repair was performed in 265 patients and a posterior repair in 30 patients. The prevalence of GERD was reduced from 45% preoperatively to 6% postoperatively, and postoperative GERD was well controlled in all patients with PPI therapy. 17 Daes et al., found that concomitant LSG and HH repair in 34 of 134 patients resulted in resolution of GERD symptoms in 94% of patients after a mean follow-up of 12 months. 18
The initial results of our study are promising, but longer follow-up of patients is needed to assess the long-term results of the technique. Also randomized controlled studies involving larger patient number comparing classic hiatal repair versus posterior repair only with LSG will be needed to draw more solid conclusions.
Conclusion
Anterior PEL-preserving HH repair combined with LSG is a safe and feasible technique that can control GERD manifestations without interference with the technique or outcome of LSG. Our study had several limitations, including the small number of the sample, absence of a control group and lack of objective pH testing and manometry. A larger randomized comparative study with a large number of patients and longer follow-up will be needed to confirm our initial results.
Ethics Approval
All procedures performed in this study were in accordance with the ethical standards of the Institutional and/or National Research Committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The approval of the Ethics Committee of Ain Shams University Hospital was obtained before the start of the study.
Informed Consent
Informed consent was obtained from all individual participants included in this study.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this study from any source.