
Abstract
Background:
Thoracoscopic resection is the standard of care for congenital lung malformations (CLMs) in infants. However, there is rising concern that capnothorax may affect cerebral perfusion and oxygenation, carrying potential long-term effects on neurodevelopmental behavior. The aim of our study was to investigate, using near-infrared spectroscopy (NIRS), the regional cerebral oxygenation (CrSO2) in infants undergoing thoracoscopic lung resection; the secondary aim was to assess the relationship between rSO2 and standard monitoring.
Methods:
In this retrospective study, we reviewed all infants (<1 year old, ASA II) who underwent thoracoscopic CLM resection in double-lung ventilation under fixed capnothorax parameters (5 mmHg of pressure, 1 L/minute flow), standardized anesthetic protocol, standard monitoring, and multisite NIRS in our center. We focused our attention on 8 anesthetic and surgical maneuvers, potentially affecting tissue oxygen saturation.
Results:
Ten infants met the inclusion criteria. At surgery, median age was 5.5 (4–7) months, median weight 7.2 (6.6–8) kg, median operative time 110 (55–180) minutes, and median capnothorax duration 79 (34–168) minutes. No conversion to open surgery occurred. CrSO2 values remained within clinically accepted values during thoracoscopy, beside a CrSO2 drop >20% of basal value in 1 patient, during capnothorax induction. Renal NIRS added very little to standard monitoring, which appeared generally inadequate to consistently appraise end-organ perfusion. ETCO2 best correlated with CrSO2 variations, suggesting to be able to realistically predict them.
Conclusions:
The thoracoscopic treatment of CLMs under the given conditions appears well tolerated in infants, pending the continuous adjustment of ventilator settings by an experienced anesthetist, confident with NIRS technology.
Introduction
In recent years the technological and anesthetic progress in minimally invasive surgery has allowed to extend to neonates and infants the acknowledged advantages of thoracoscopy, namely shorter postoperative-assisted ventilation, better pain control, and quicker recovery. Indeed, thoracoscopy has become the standard approach to congenital lung malformations (CLMs) in referral centers. 1 However, recent studies2–4 have questioned the tolerance of capnothorax in neonates, pointing at the risk of hypercapnia, acidosis, and hemodynamic derangement, which may affect cerebral perfusion and oxygenation, carrying potential long-term effects on neurodevelopmental behavior.5,6 So far, only one study 7 has evaluated the tolerance and safety of thoracoscopic lung resection in 5 infants of a mixed cohort undergoing thoracoscopy.
In our center, since 2016, children affected by CLMs undergo thoracoscopic lung resection according to a protocol that includes fixed capnothorax parameters, standardized anesthetic management, standard monitoring, and multisite near-infrared spectroscopy (NIRS). This protocol focuses on 8 anesthetic and surgical activities, which may affect regional oxygen saturation (rSO2). We used these time points, rather than fixed time intervals,8–10 for data collection and analysis. Multisite NIRS, simultaneously monitoring blood flow distribution and oxygen delivery to organs whose perfusion depends on different neurohormonal mechanisms, reveals changes of the patients' state that may go otherwise undetected by conventional global circulatory monitoring. In addition, the present NIRS technology is more suitable in patients weighing <10 kg, making infants ideal candidates.11,12
In an invited editorial, Macchini 13 has recently quoted preliminary data regarding the general population undergoing thoracoscopy in our center. To investigate the tolerance of thoracoscopic lung resection in the vulnerable infant population,6–8 we performed a review of our case series. The primary aim of this study was to investigate the effect of the given capnothorax setting and anesthetic protocol on regional cerebral (CrSO2) and renal (RrSO2) oxygenation assessed by NIRS; the secondary aim was to assess the relationship between rSO2 and standard monitoring.
Materials and Methods
Parental informed consent for data management was acquired, and all the information was submitted and approved by the Ethics Committee of the Hospital (205_2019, March 6th, 2019).
The study population includes all consecutive infants (<1 year-old), without other comorbidity (ASA class II), who underwent thoracoscopic CLM resection in tracheal intubation and double-lung ventilation under multisite NIRS and standard monitoring between July 2016 and October 2018 at the Fondazione IRCCS Ca’ Granda, Ospedale Maggiore Policlinico, Milan, Italy.
Patients underwent general anesthesia (GA) according to an anesthetic protocol, including endotracheal intubation with a cuffed tube, mechanical 2 lungs ventilation, tidal volume (TV) of 6–8 mL/kg, and either volume or pressure controlled ventilation. Inhalation mask induction was performed with 6% sevoflurane and 80% fraction of inspired oxygen (FIO2), followed by fentanyl (2 mcg/kg) and propofol (2 mg/kg). We accomplished muscle relaxation with rocuronium (0.6 mg/kg) and maintained anesthesia with sevoflurane (MAC 1), fentanyl (1–2 mcg/kg/hour), and rocuronium (0.2 mg/kg/hour). After induction, FIO2 was kept at 40%–50%. Euvolemia was granted according to the 4-2-1 mL/kg universal rule +6 mL/kg per hour of anesthesia. We continuously adjusted FIO2, positive end expiratory pressure, TV, respiratory rate, and peak inspiratory pressure (PIP), within protective ventilation limits, to keep the arterial oxygen saturation (SpO2) and the end-tidal pressure of CO2 (ETCO2) in the 95%–99% and 35–45 mmHg range, respectively, and CrSO2 within clinically accepted limits. Normothermia was kept using a circulating warm air device and warm infusions.
Monitoring included cerebral and renal continuous NIRS. For this purpose, we applied one pediatric sensor to the forehead above the supraorbital ridge, and a second one to the decumbent lumbar region at T12–L2 level. NIRS monitoring was accomplished using an INVOS™ 5100 C cerebral/somatic Oxymeter (Medtronic, Covidien, Mansfield, MA). Data were analyzed using the INVOS Analytics tool. We acquired a basal CrSO2 and RrSO2 NIRS value at T0 in the operating room, at a steady state, while the patient was breathing room air, was quiet and not crying. Mean NIRS values were derived from the continuous reading at preset points (T1: induction of GA, T2: beginning of mechanical ventilation, T3: insertion of trocars, T4: induction of capnothorax, T5: specimen retrieval, T6: pneumatic check, T7: evacuation of capnothorax, and T8: emergence), as punctual values of the steady state, following completion of the index maneuver. NIRS events were defined as follows: any decrease of rSO2 between 11% and 20% below baseline lasting longer than 3 minutes was considered as mild low saturation; any decrease between 21% and 30% below baseline lasting longer than 3 minutes was defined as moderate low saturation; while any decrease greater than 30% below baseline lasting longer than 3 minutes or any absolute decrease below 50% was regarded as severe low saturation.8,14 The anesthetist was not blinded to NIRS values.
Standard monitoring included continuous ECG, noninvasive blood pressure, set at 5-minute interval, SpO2, ETCO2, and temperature control via an esophageal probe. At discretion of the attending anesthetist, either a central venous catheter or an arterial line was threaded for blood sample drawing. We performed blood gas analysis before, during and after capnothorax. The range of normality for pH was 7.35–7.45. Heart rate (HR) and noninvasive mean arterial pressure (MAP) were compared with standard values of healthy patients, stratified by age and sex.15,16 Values of ETCO2 below 24 and above 54 mmHg were regarded as severe hypocapnia and severe hypercapnia, respectively. 17 Mean values of standard monitoring were obtained from the anesthetic charts at the preset points.
At our institution, thoracoscopic lung resection is typically performed by 2 skilled pediatric surgeons, using a mean insufflation pressure of 5 mmHg, with a CO2 flow rate of 1 L/minute. CO2 insufflation can be temporarily paused to allow ventilation adjustment. Patients are operated in semiprone position. Following the completion of the procedure, all patients were admitted to the pediatric intensive care unit (PICU) for postoperative observation and extubation.
Statistical analysis
We presented mean, median, and min–max values of CrSO2, RrSO2, and ETCO2 during 8 surgical and anesthetic maneuvers over time. To take into account the intrasubject correlation over time, we fitted random intercept linear regression models, in which time was treated as a dummy covariate. To visualize time patterns of CrSO2 and RrSO2 we graphed individual and mean values and used box-and-whiskers plots to show percent changes compared to baseline. To assess relationships between CrSO2 or RrSO2 and ETCO2, MAP, SpO2, and HR, we calculated Spearman's rho coefficients and fitted random-intercept linear regression models to estimate slopes and their 95% confidence intervals. Statistical analyses were performed with Stata 16 (StataCorp. 2019).
Results
Between July 2016 and October 2018, 22 children underwent thoracoscopic resection of CLMs at our institution, 10 of which met the inclusion criteria for this retrospective study. All infants had normal hemoglobin level according to age, and none was transfused during surgery or in the postoperative period. No conversion to open surgery occurred.
Table 1 summarizes the demographic and procedure-related data. During thorascopy, the highest CrSO2 value attained was 95 and the lowest 52% (Table 2). Mean CrSO2 greatly increased with induction of anesthesia (+17%, P < .001) and beginning of mechanical ventilation (+19%, P < .001), dropped to basal values at T3, and then remained stable until emergence (Fig. 1A, B). Three patients poorly tolerated the surgical maneuvers at T3–T4, and in a single patient CrSO2 declined more than 20% of the basal value (bottom value 61% = 22% decrease) after starting CO2 insufflation (T4). Mean RrSO2 greatly increased over basal values at T2 (+12%, P < .001), and persisted elevated throughout surgery (Fig. 1C, D). Severe hypocapnia was never observed, while severe hypercapnia occurred in a single patient at the beginning of mechanical ventilation (T2), lasting less than 5 minutes. Mean ETCO2 significantly declined at T3–T4 (Table 2 and Fig. 2C).
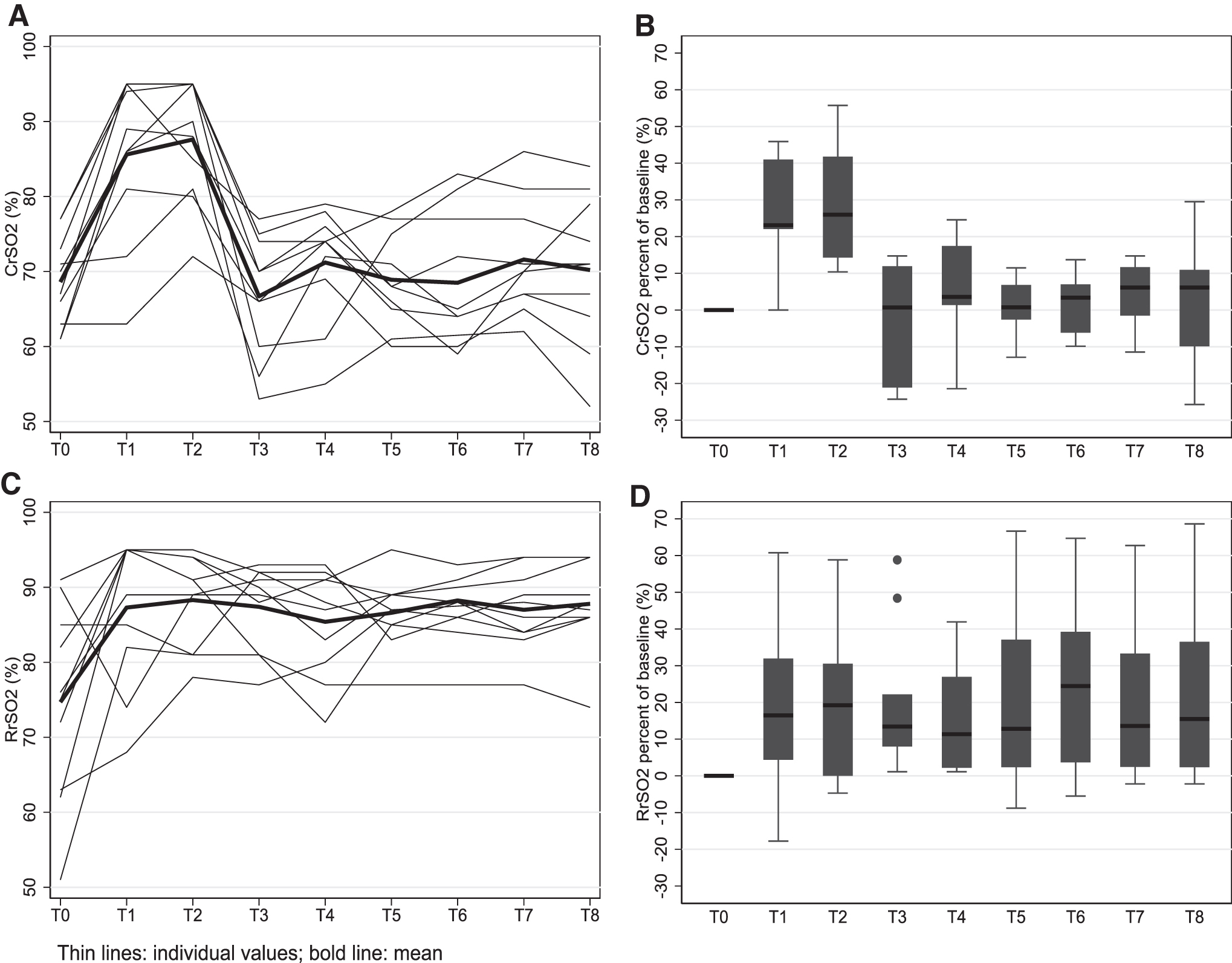
Trends of CrSO2 and RrSO2 over time.
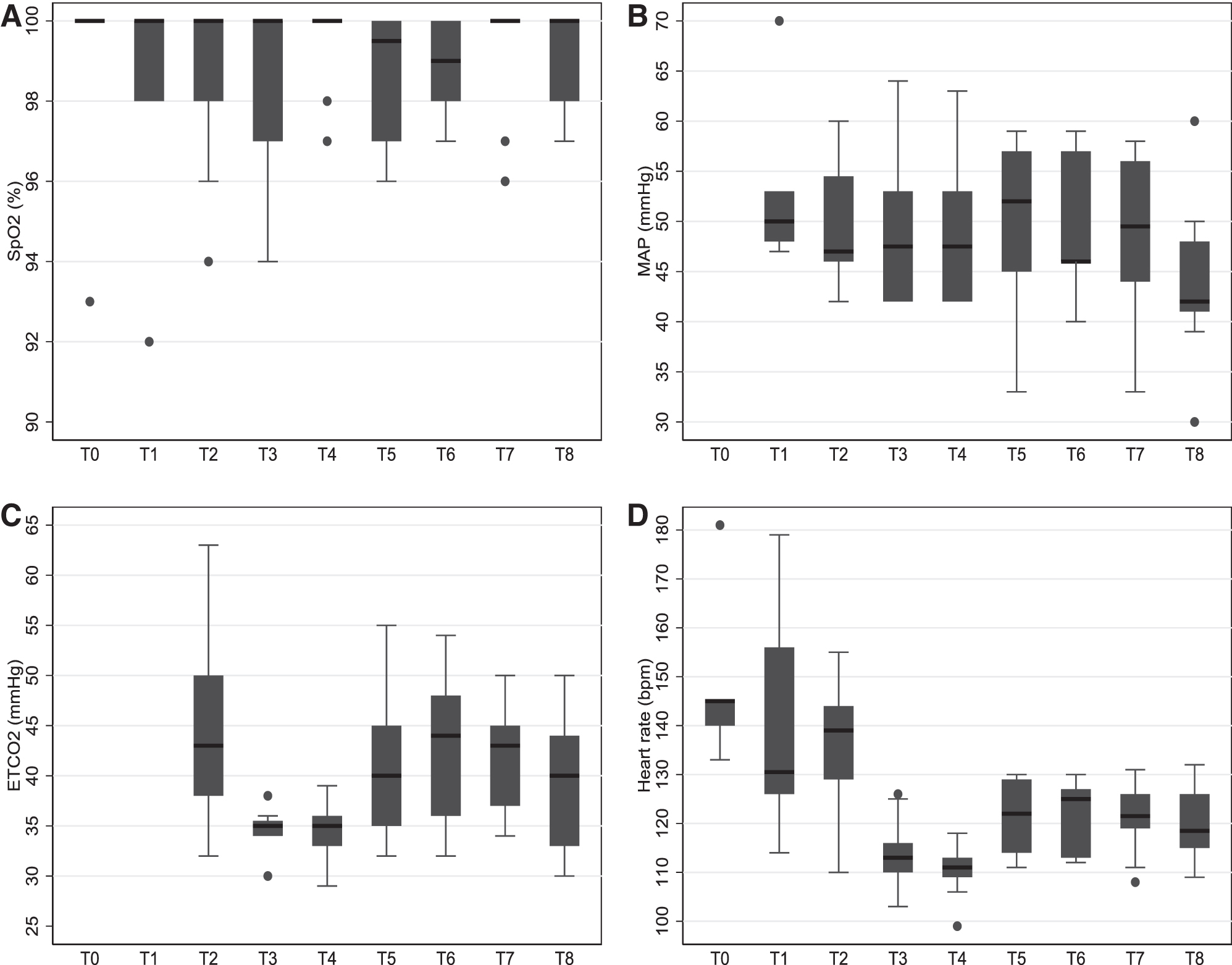
Trends over time of SpO2
Demographics of the Population at Study and Procedure-Related Data
Trends of CrSO2, RrSO2, and ETCO2 Over Time in Infants Undergoing Thoracoscopic Lung Resection
P < .001 compared to T0 (CrSO2, RrSO2), or to T2 (ETCO2), from random intercept linear regression models.
GA, general anesthesia; NA, not applicable.
Figure 2 summarizes standard monitoring. SpO2 decreased below 95% in 3 patients (once for two, twice for the third) for less than a minute each. HR dropped at T3 and T4 (Fig. 2 D). A single hypotensive episode was registered during CO2 insufflation (T4), concomitant with CrSO2 desaturation, in the above-mentioned patient.
CrSO2 was strongly associated with ETCO2, MAP, and HR, but not with SpO2 (Fig. 3). RrSO2 was fairly stable during thoracoscopy and showed little or no association with standard monitoring variables (Fig. 4).
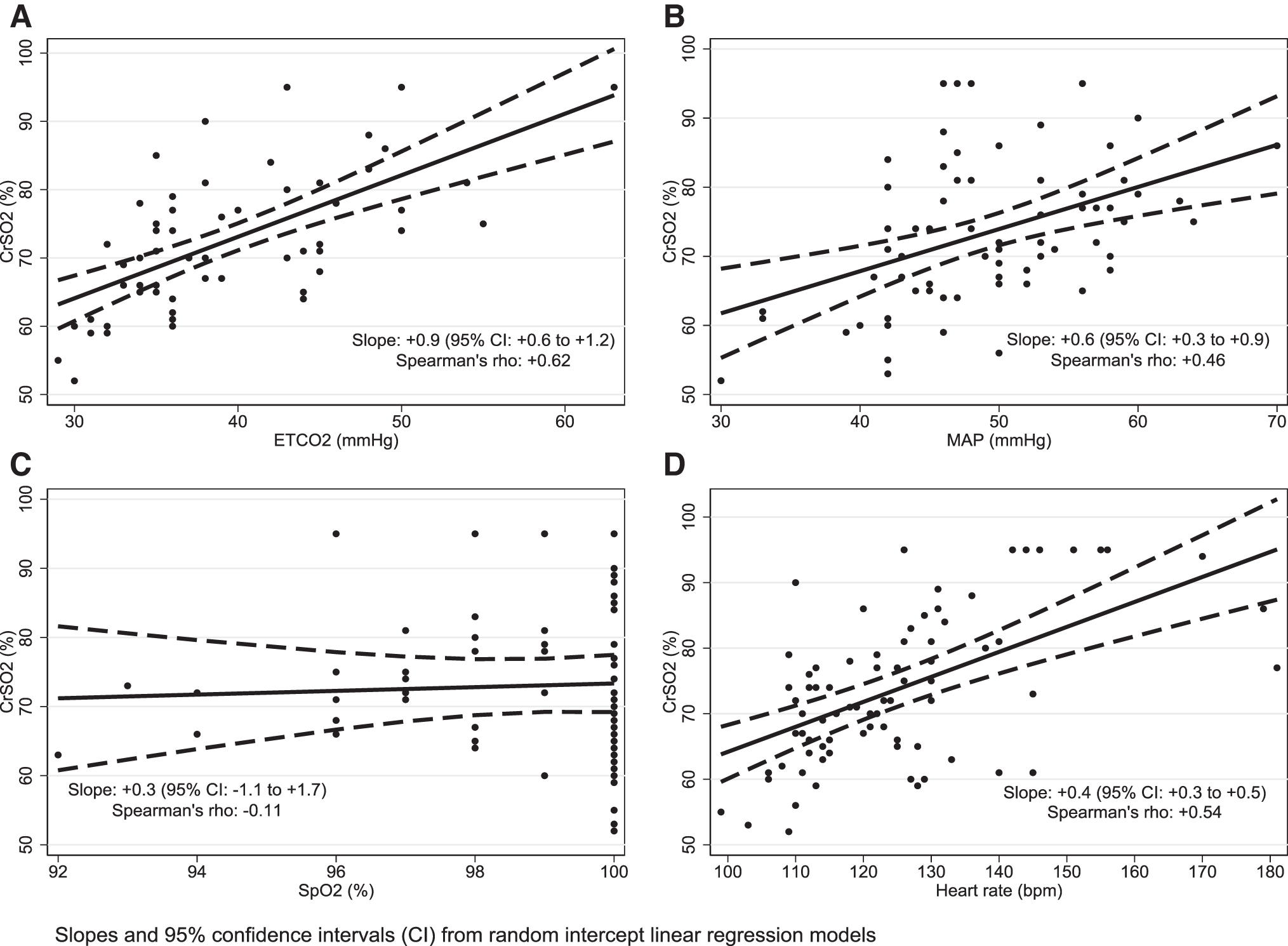
Relationship between CrSO2 and ETCO2
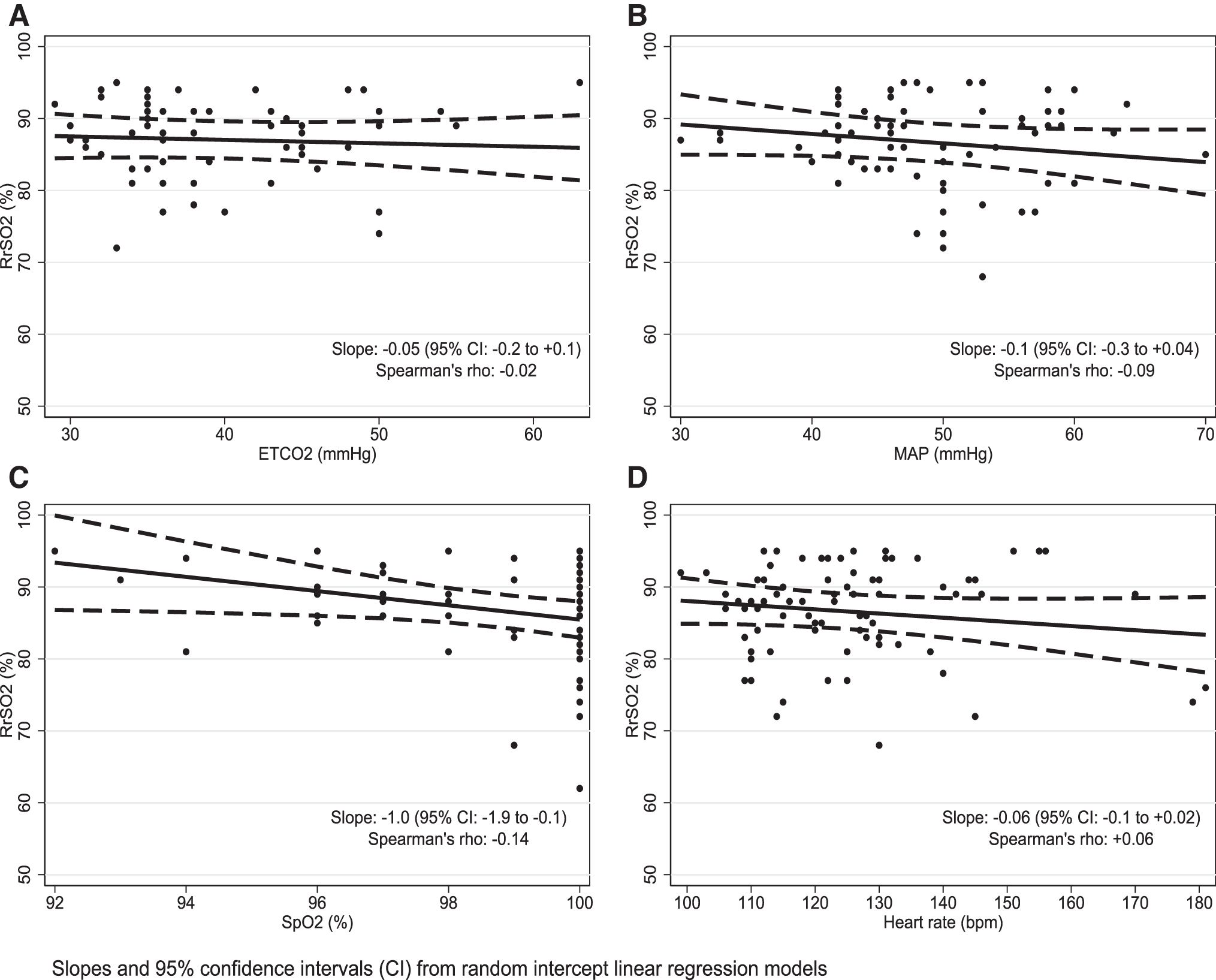
Relationship between RrSO2 and ETCO2
Mean pH values during thoracoscopy (7.27 ± 0.017, range 7.21–7.33) were lower (P = .01) than before capnothorax induction (7.35 ± 0.02, range 7.30–7.41) and than those observed at emergence (7.32 ± 0.01, range 7.29–7.38). The lowest pH value was 7.21. Mean body temperature was 36 C ± 0.3°C throughout surgery.
All patients had their tracheal tube uneventfully removed in PICU within few hours. No seizures were observed in the 48 postoperative hours.
Discussion
The technological advancement that has allowed to broaden thoracoscopic surgery to neonates and infants has required simultaneous improvements in anesthetic skills, practice, and monitoring techniques to cope with the adverse effects of artificial CO2 pneumothorax.2–4 NIRS offers a continuous, noninvasive method of monitoring regional changes in tissue oxygen saturation, using a near infrared light to measure the tissue concentration of chromophores. Chromophores are found in both oxygenated and deoxygenated hemoglobin, and NIRS measures the balance between oxygen supply and extraction, mirroring tissue oxygen consumption. 11
In our study, we observed a conspicuous increase of CrSO2 from the basal values during induction and beginning of mechanical ventilation. Vasodilation produced by anesthetic volatile drugs,18,19 reduction in metabolic rate under GA,18–20 and high FIO2 20 may explain this common observation,2,8,20 which is deemed mandatory. 21
So far, the effects of artificial CO2 pneumothorax on CrSO2 have been investigated in neonates during surgical treatment of congenital diaphragmatic hernia (CDH) and esophageal atresia (OA),2–4,9,10 and in a mixed cohort, including 5 infants undergoing thoracoscopic lung resection. 7 Our series is therefore the largest so far reported in literature.
Stolwijk et al., 9 observed that impaired venous blood return, increased central venous and intracranial pressures, as well as reduced cardiac output due to extrinsic compression and higher oxygen extraction may all contribute to transient CrSO2 decline during capnothorax, despite mild hypercapnia, favoring vasodilation. During trocar insertion (T3) 3, patients showed a CrSO2 decline below basal values, representing mild low saturation, which persisted in 2 of them during CO2 insufflation (T4) (Fig. 1A). However, this decline exceeded the 20% limit in a single patient, whose lowest value was 61%, representing mild desaturation. 8 Extrinsic compression of the supple, highly deformable infant ribcage during trocar insertion, and the increased intrathoracic pressure due to capnothorax likely contributed to the observed CrSO2 drops. Concurrent declines in HR, possibly due to vagal reflex or impaired cardiac compliance, and in ETCO2, without changes in SpO2 and MAP, suggest decreased cardiac output. An increased cerebral oxygen extraction, likely secondary to impaired venous return, further contributed to the CrSO2 decline. However, as we did not directly investigate cardiac output, we cannot further speculate on mechanisms connected to the observed derangements.
The low insufflation flow and CO2 pressure of our surgical protocol have likely contributed to limit in most patients the adverse effects of capnothorax. Indeed, Neunhoeffer et al. 7 have shown that a linear relationship exists between CO2 pressure increase and CrSO2 decline: rising the capnothorax pressure from 4 to 8 mmHg causes a predictable decline of CrSO2 greater than 20% of the basal value. The authors concluded that 4 mmHg should be the upper pressure limit of capnothorax in neonates and infants.
It is known that CO2 absorption during thoracic insufflation is higher than during laparoscopy, 22 causing severe hypercapnia and acidosis,2,3 whereas oxygenation is not altered. 3 However, a 5-mmHg-pressure capnothorax allows performing thoracoscopy with reversible arterial hypercarbia and acidosis,9,10,20 while keeping CrSO2 within clinically acceptable limits during periods of combined acidosis. 10 Hypercarbia and acidosis can be alleviated by continuous adjustment of ventilator settings such as increasing TV, 20 fine-tuning of PIP, 10 and increasing FIO2, 9 as confirmed by our experience. Indeed, pH was only marginally affected by capnothorax, and severe acidosis and hypercarbia were not observed. In summary, we confirm that the combination of low CO2 pressure and flow with an attentive anesthetic protocol, including cerebral NIRS, can overtake the expected physiologic derangements due to artificial capnothorax, keeping CrSO2 values within clinically accepted limits.
Thoracoscopy in single lung ventilation could be an alternative strategy to further improve the tolerance to the capnothorax in infants, as lower insufflation pressures are required when the ipsilateral lung is not ventilated and therefore already collapsed. Moreover, it has been suggested that single-lung ventilation with bronchial occlusion also reduces the absorption of CO2, 23 altogether improving the cardiorespiratory stability of the child. We believe that this might be of help especially when working on the upper lobes, where spaces are more limited due to the scheletric conformity of the thorax itself. No case of upper lobectomy was part of our series and all operations were managed on tracheal ventilation without complications.
Furthermore, studies have been so far conducted only in presence of higher insufflation pressures (>6 mmHg), and future studies are required to establish the benefits of single lung ventilation as opposed to tracheal intubation with low insufflation pressures (4–5 mmHg).
For the first time, we added renal NIRS monitoring during thoracoscopic lung resection in infants. In children weighing less than 10 kg, renal NIRS gives an accurate, noninvasive, real-time measurement of renal oxygenation, which can be used as an indicator of global perfusion. 12 Actually, during low cardiac output, CrSO2 may not represent end-organ perfusion because of the sympathetic activation, which shunts blood away from somatic beds to the brain. Instead, the somatic-cerebral difference, which normally fluctuates around 10 points in favor of the kidney, will be reduced, thus providing a window on the changes in distribution of the cardiac output. 12 Our mean renal rSO2 values were just slightly higher than the cerebral ones at baseline, increased consistently at induction, and remained stable thereafter. This clinical behavior recalls that of moderately dehydrated infants, whose RrSO2 significantly increases following rehydration, as well as the somatic-cerebral SO2 difference, as shown by Hanson. 24 We speculate that hydration during induction likely contributed to the increase of RrSO2 in our patients, who arrive in the OR faintly dehydrated due to preoperative fasting.
In their article, Neunhoeffer et al. 7 remarked that CrSO2 drops were not detectable by standard monitoring, as SpO2 steadily remained within normal limits. Our experience confirms this observation (Fig. 3C). In addition, MAP spotted a single associated CrSO2 drop during capnothorax induction. Of the additional main contributors of NIRS-derived cerebral rSO2, 20 ETCO2 best correlated with CrSO2 variations, suggesting that this monitoring can realistically predict CrSO2 variations.
The clinical and hemodynamic stability of our patients during thoracoscopy is mirrored by the standard monitoring variables, which consistently fell in the range of normality with sparse outliners (Fig. 4), and poorly correlated with RrSO2. Indeed, renal NIRS added very little to monitoring, likely because no major hemodynamic derangement occurred in this series.
The main limitation of this study lays in the small number of patients enrolled. However, the low incidence of lung malformations suitable for thoracoscopic resection in infants limits recruitment. Our conclusions should also be tempered by the retrospective nature of the study, which adds possible biases due to selection criteria, and by the lack of a control series, which prevents us from arguing about safety of thoracoscopy in the given settings. Another limitation is the absence of shared definition of what constitutes desaturation in NIRS, although we used the currently available reference criteria.8,14 Indeed, a consensus has not been reached regarding the lower limit of NIRS CrSO2, and the baseline-bottomline approach suggested by Weber 20 has not been validated yet.
So far, only in cardiac surgical patients, viability-time thresholds to define hypoxia and ischemia and predict long-term neurological outcome have been determined using NIRS. Moreover, the relationship between decreased CrSO2 and neurodevelopmental measures appears not to be linear. 25 Animal studies have shown that impairment of the neurophysiologic function occurs only when CrSO2 remains lower than 40% for up to 2 hours. 26
Neurocognitive follow-up in noncardiac surgical patients is currently poor. So far, only one study investigated the relationship between cerebral desaturation and neurodevelopmental outcomes of neonates undergoing thoracoscopic correction of CDH and OA. 10 The authors concluded that the outcome in such patients was favorable at 24 months follow-up. A recent large multicenter study 8 using cerebral NIRS in infants undergoing general surgery revealed that during anesthesia, mild cerebral deoxygenation is common, while severe cerebral desaturation is both rare and brief. Thus, GA and surgery would be unlikely the cause of learning and behavioral abnormalities putatively associated with them. However, continuing follow-up with Bayley's scoring scales in the first 3 postoperative years could be valuable.
Conclusions
Our study suggests that the thoracoscopic resection of CLMs, using a CO2 pneumothorax pressure of 5 mmHg and a low CO2 flow, is well tolerated in infants, pending the continuous adjustment of ventilator setting by an experienced anesthetist, confident with NIRS technology. Trocar insertion and capnothorax induction appear to be the most threatening maneuvers. Standard monitoring appears inadequate to consistently appraise end-organ perfusion, with the exception of ETCO2, whose reading can address CrSO2 derangements in infants. Further studies are required to confirm our findings and the value of NIRS as additional monitoring device for infants undergoing thoracoscopy.
Footnotes
Authors' Contributions
S.F., A.M., F.P., F.M., and E.L. gave substantial contribution to study conception and design. S.F. and F.P. performed the data acquisition. Analysis and interpretation of data were performed by S.F., A.M., F.P., and D.C. and F.M., S.F., F.P., and D.C. contributed to the first draft of the article; all the authors critically revised the text for intellectual content. All authors read and approved the final version of the article.
Acknowledgments
Thanks to Doctor Paolo Setti Carraro and to Professor Giorgio Conti for reviewing the article and for the great support. Thanks to Doctor Sergio Cereghini for contributing in data acquisition. Thanks to Doctor Simona Neri and to Doctor Valerio Gentilino for the technical contribution.
Disclosure Statement
Congress where the article was presented: 23° Congresso Nazionale S.A.R.N.eP.I, Ferrara 12/14 settembre 2019.
Funding Information
No funding was received for this study