
Abstract
Although laparoscopic adjustable gastric band (LAGB) placement appears as a safe and reproducible procedure, serious complications can occur. We present a patient with fever, dysphagia, epigastric pain, and port site inflammation. Esophagogastroduodenoscopy and computed tomography (CT) scan diagnosed esophageal erosion of the gastric band. An endoscopic retrieval was proposed to avoid accessing the abdominal cavity and mediastinum, reduce recovery time, and minimize complications. The patient successfully underwent the procedure with immediate improvement of symptoms and discharge on the seventh postoperative day. This article aims to report the first clinical case of an esophageal erosion of LAGB completely treated with an endoscopic approach.
Introduction
Laparoscopic adjustable gastric band (LAGB) placement has been widely adopted as a treatment for morbid obesity. Several studies proved its benefits including long-term follow-up series. The advantages of this surgical technique are its reversibility potential, low rate of intraoperative complications, reduced surgical time, and hospital stay. Known disadvantages are related to the prosthetic presence and the need for a close follow-up. 1 Although benefits have not surpassed disadvantages and there has been a sudden decline in the indication, many patients still keep their band in place. Nowadays, more effective alternatives, such as laparoscopic sleeve gastrectomy, Roux-n-Y gastric bypass, or one anastomosis gastric bypass, are preferred.
Complications such as slippage, fistulae, and abscesses have been described with varying frequencies. 2 Erosions commonly involve the gastric wall, and there are few reports of erosion of an adjustable gastric band (AGB) into the esophagus after a regular uneventful placement.3,4 Band erosion treatment consists of the removal of the device either with a surgical or endoscopic approach. Although cardial or gastric endoscopic band extraction has been published, 5 the objective of this article is to report the first medical case of an esophageal erosion of LAGB treated with endoscopic retrieval.
Case Presentation
A 40-year-old male with super obesity was referred to the bariatric and metabolic surgery clinic for evaluation and treatment recommendations in December 2001. The medical evaluation showed a remarkable history of hypertension under medical treatment, dyslipidemia, and obstructive sleep apnea hypoventilation syndrome. His initial weight was 186 kg and a body mass index of 61.3 kg/m2.
The patient underwent laparoscopic placement of an AGB (Obtech®) at the gastroesophageal junction (GEJ) using the pars flaccida technique (PFT) without a gastro-gastric suture. The surgical procedure was performed without intraoperative or early postoperative complications. During the first 24 months, he lost 93 kg with an improvement of his comorbidities and did not report any complications related to the LAGB. He did not concur to further follow-up visits during the following 8 years.
In December 2012, the patient presented to the clinic with a chief complaint of dysphagia and epigastric pain. No other symptoms were described and no medical findings were relevant in the physical examination. Simple abdominal X-rays did not show band-related complications and normal positioning. An esophagogastroduodenoscopy (EGD) was performed showing acute antral gastritis positive for Helicobacter pylori, mild esophageal dilation with grade I esophagitis, and esophageal compression at the GEJ. The patient was treated with omeprazole 20 mg and had a favorable evolution.
In April 2013, the patient returned to the clinic with dysphagia to solid food, persistent fever, and inflammation surrounding the gastric band port. A new EGD was performed and showed an esophageal erosion of the gastric band occupying 20% of the lumen, 3 cm proximal to the esophagogastric junction.
Due to the inability to puncture and deflate the gastric band because of port rotation, a surgical extraction was required. At the time of the port dissection, purulent drainage was obtained, which resulted positive for Escherichia coli in bacteriologic testing. The gastric band was completely deflated by sectioning and closing the catheter, subcutaneous drains were placed, and an antibiotic regimen was initiated. Forty-eight hours later, the patient improved his dysphagia and fever and was discharged from our service. The surgical team decided to evaluate his medical evolution before further surgical intervention with the expectation to remove the band endoscopically when a considerable percentage of the esophageal lumen was eroded.
Six months later, the patient experienced new episodes of solid dysphagia, postprandial retrosternal pain, sporadic fever episodes, and heartburn. A new EGD and computed tomography (CT) scan were performed confirming a distal esophageal erosion of the gastric band 4 cm proximal to the esophago-gastric junction (EGJ) (Fig. 1). As a result of this clinical evolution, endoscopic removal of the gastric band was decided. The patient consented to proceed with this surgical approach.
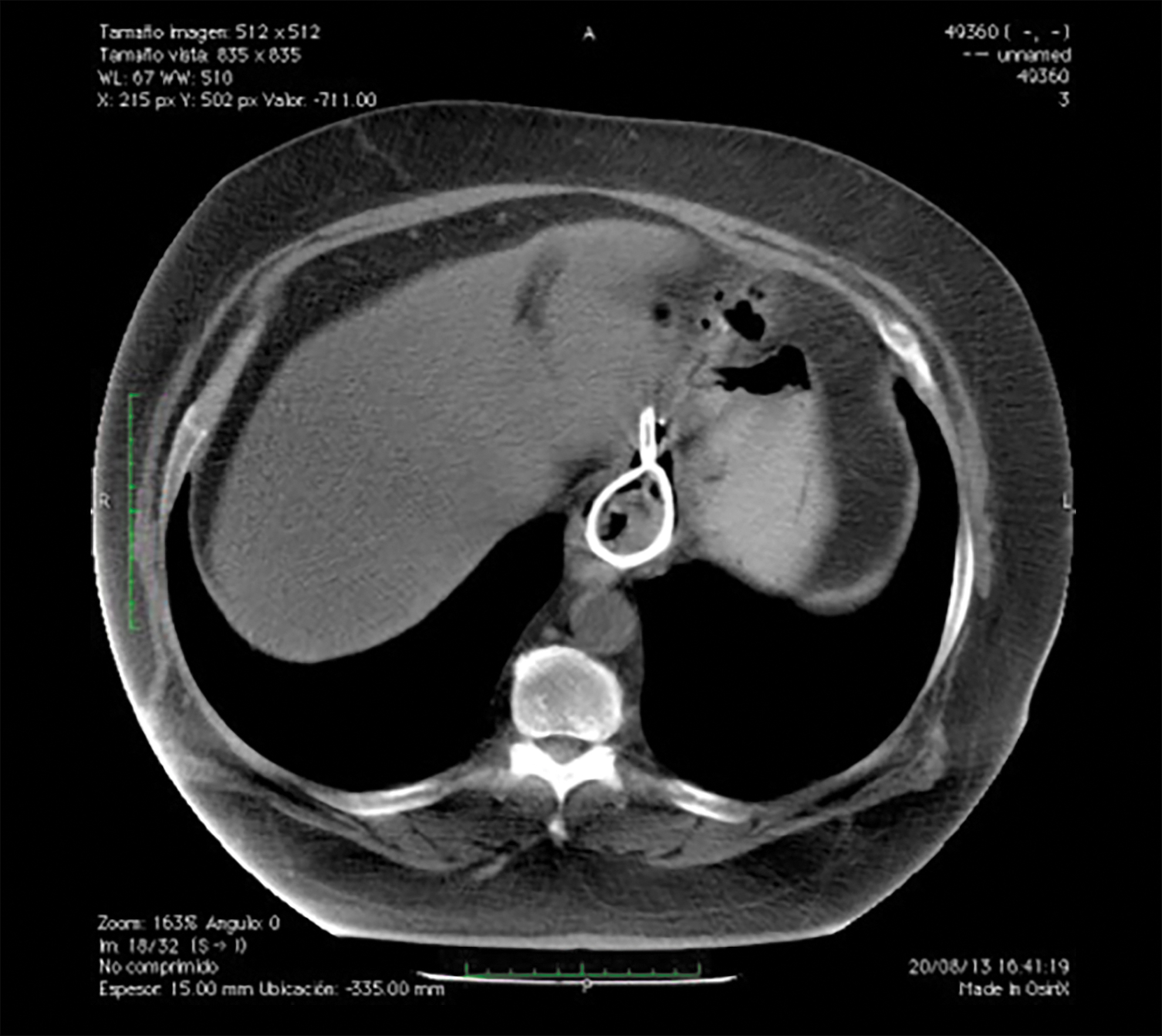
CT scan demonstrating a portion of the AGB inside the esophageal lumen. AGB, adjustable gastric band; CT, computed tomography. Color images are available online.
Surgical Technique
Under general anesthesia, the patient was placed in a supine position with the head tilted to the left. The surgeon on the patient's left side and the assistant at the patient's head with the endoscopy tower on the patients' right side.
Using an 8.6-mm-wide gastroscope, an endoscopy was performed. After the initial exploration of the esophagus and gastric cavity, cutting off the band with endoscopic scissors was attempted without success due to its thickness (Fig. 2). The band buckle was recognized in a paraesophageal cavity. A hydrophilic endoscopic guidewire was introduced through the buckle suture holes and then pulled out through the patient's mouth achieving control and traction of the prosthetics (Fig. 3). A second hydrophilic endoscopic guidewire was introduced around the band and retrieved through the mouth. Using a lithotripter, the band was cut under direct endoscopic view (Fig. 4). Finally, the gastric band was removed pulling from the guidewire placed before. After removal, a large defect of the esophageal mucosa was identified (Fig. 5), however, due to the inflammation of this area at that moment, endoscopic clipping was not possible and a nasojejunal catheter was placed to avoid oral feeding.
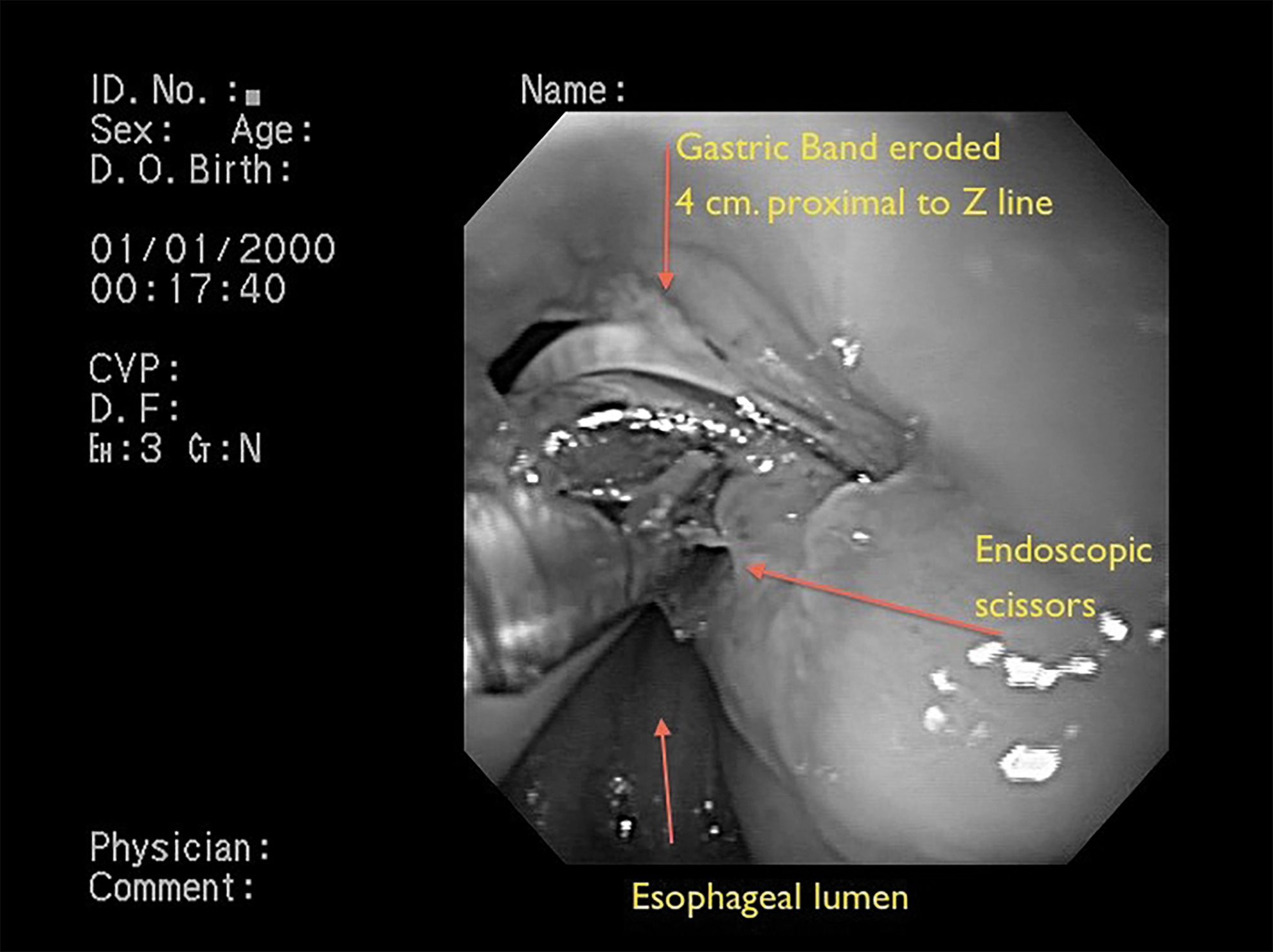
First attempt to cut the AGB with endoscopic scissors. AGB, adjustable gastric band. Color images are available online.
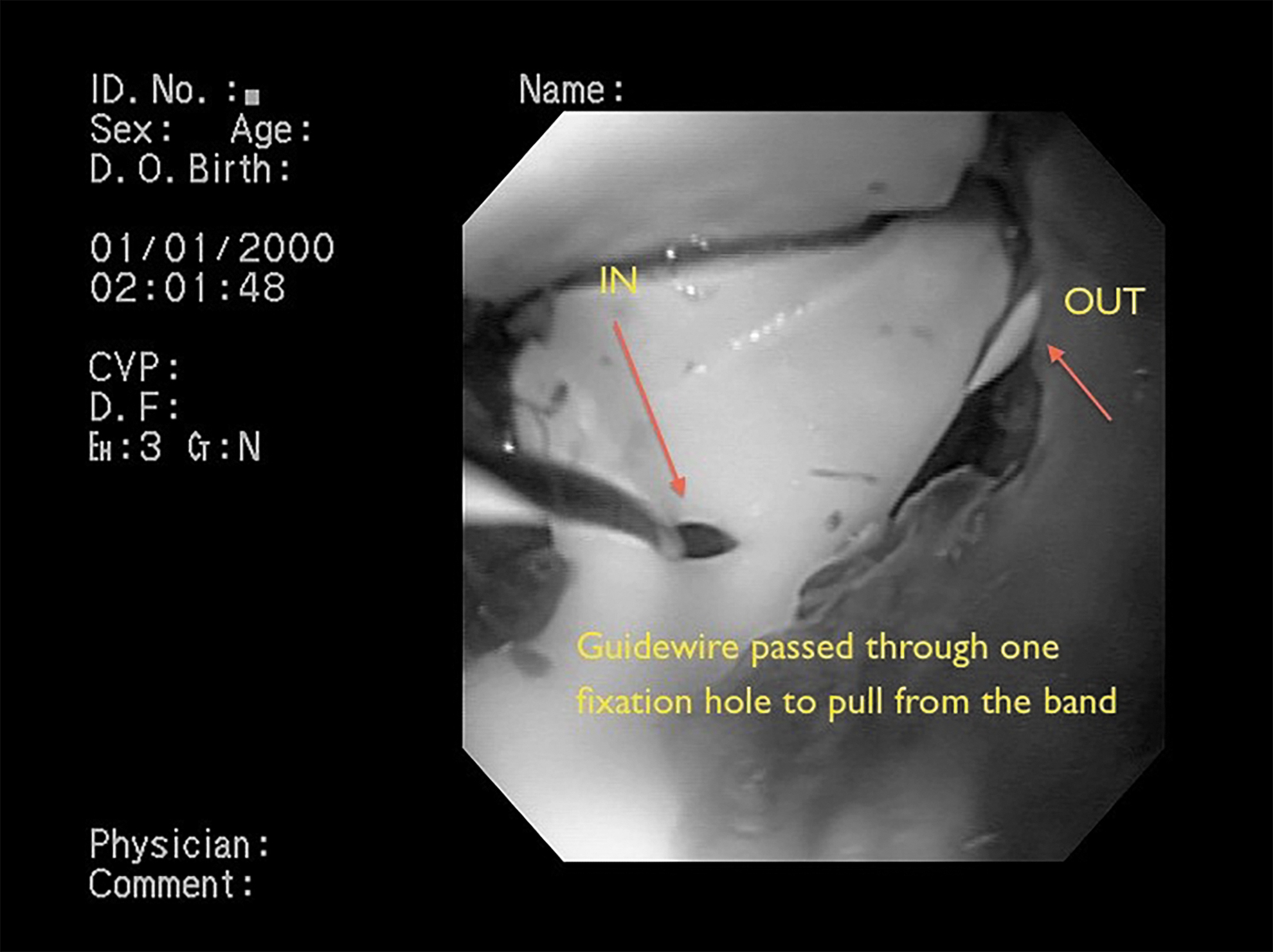
Pulling off the AGB buckle using a guidewire. AGB, adjustable gastric band. Color images are available online.
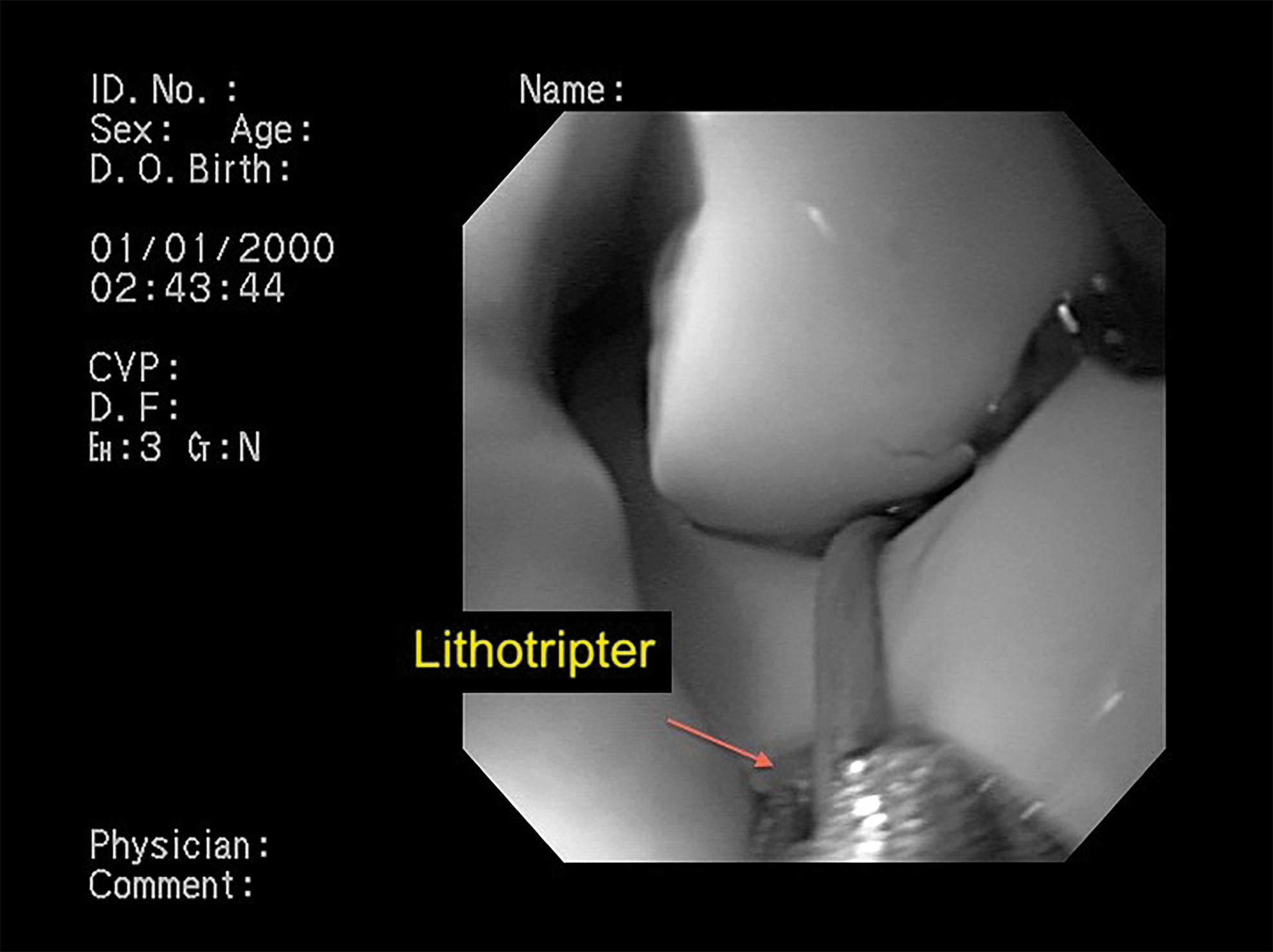
The AGB was cut with a lithotripter. AGB, adjustable gastric band. Color images are available online.
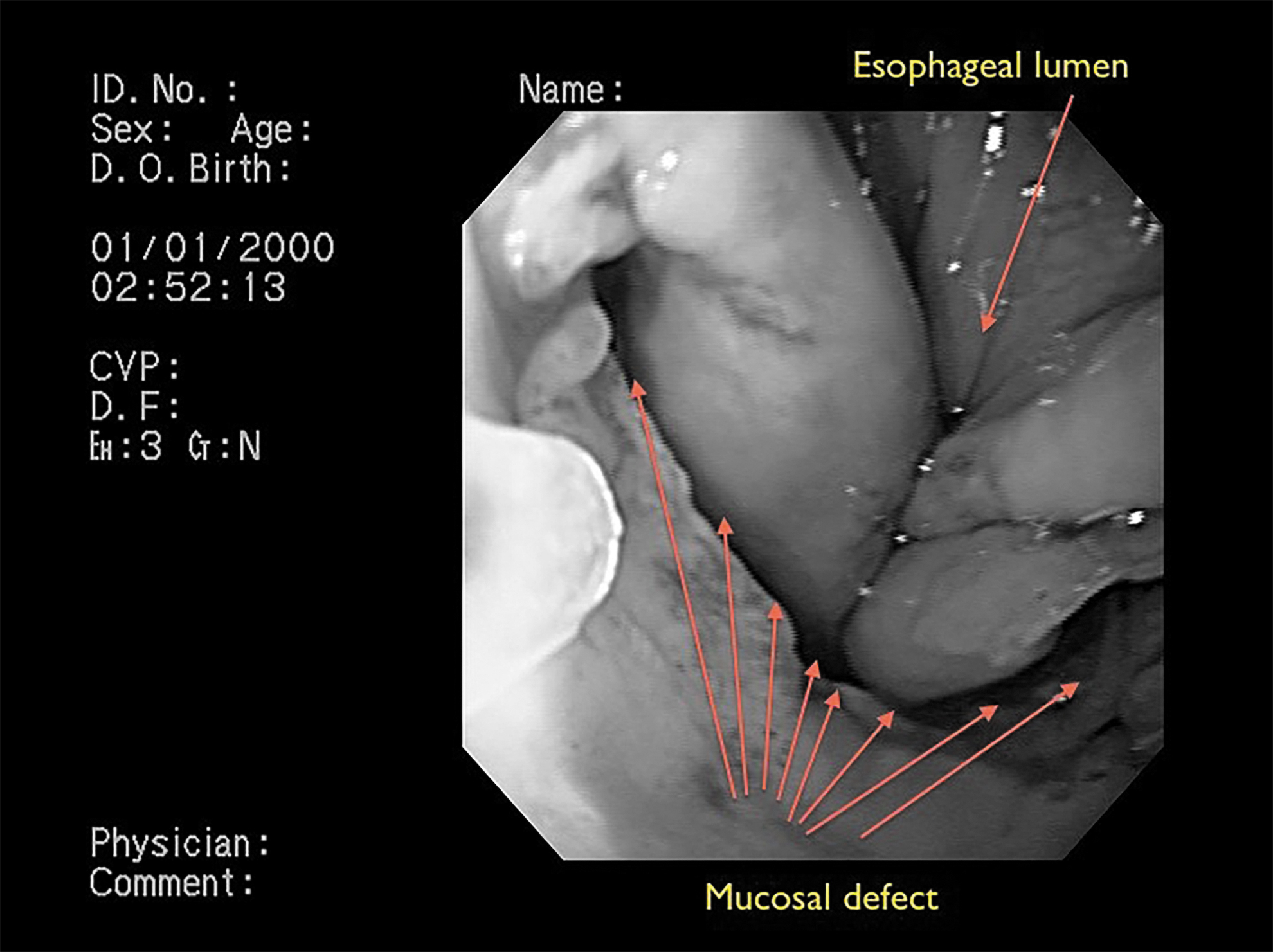
Large mucosal defect after AGB removal. AGB, adjustable gastric band. Color images are available online.
Postoperative management consisted of nil per os, total enteral nutrition using the nasojejunal catheter, and an intravenous antibiotic regimen of clindamycin and gentamicin. The patient progressed with no symptoms and was discharged on the seventh postoperative day. Fourteen days after the procedure, a new EGD observing closure of nearly 80% of the esophageal erosion and the absence of a stricture. Swallow tests showed a small cavity next to the esophageal erosion with no further progression of contrast. On the 21st postoperative day, oral intake was resumed and the patient did not present any complications, and so, the nasojejunal catheter was withdrawn. After 6 months, endoscopic surveillance showed only a tortuous distal esophagus without stenosis.
Discussion
Several complications related to AGB have been described and visceral erosion is among the most serious, requiring the extraction of the prosthetics. Incidence varies between 1% and 11%6,7 and presentation is mostly in the long term. Inflammation, infection, and the presence of the prosthesis can cause excessive pressure in the gastric wall and migration into the lumen. Since this is an atypical presentation, doubts arise if the pathogenesis remains the same as with gastric erosion, or other mechanisms such as thoracic negative pressure or band herniation are involved.
Four approaches have been reported to remove the band, endoscopic, laparoscopic, laparotomic, or hybrid. 8 With a laparoscopic or laparotomic approach, adhesions can complicate the reaching or sectioning of the band. Also, the visceral wall needs to be repaired, and a significant risk of postoperative leak or peritonitis arises. Endoscopic extraction has minimal risks of a leak, it is a safe and efficient procedure with a high success rate, low morbidity, and no mortality, but if less than 50% of the band or the buckle is not eroded, the failure rate is high. Overinsufflation of the band has been suggested to achieve further erosion. 5 In our clinical case, the patient presented with significant dysphagia, and treatment was necessary at the time of presentation. A surgical approach with dissection of the distal esophagus and EGJ, although feasible, would have been risky, and it can be assumed that the leak rate of an esophageal closure after band extraction can be high. This complication being very rare, the patient had a prolonged hospital stay, but without any signs of complications whatsoever. An early discharge with nasojejunal feeding could have been done in an outpatient setting. The cavity and adhesions formed minimize the risk of leaks or peritonitis when eroded bands are removed endoscopically from the stomach. Similarly, this happened in our case without mediastinal repercussion. Nowadays, we would probably use EndoVac to accelerate the closure of the cavity. The favorable result of the treatment exposed does not justify that every esophageal erosion of a gastric band should be treated the same way. Clinical presentation, radiologic, and endoscopic details should be considered with each patient. The absence of a fluid collection next to the band, for instance, discouraged the necessity of drainage, and band retrieval was the only priority.
AGB erosions will continue to arise since many have been placed globally. Endoscopic treatment has proven to be safe after different clinical presentations. This case report shows that the applicability can be extended to esophageal erosion.
Conclusion
Although long-term complications related to the placement of an AGB have been described, this is the first case report of an esophageal erosion. Its management will depend on the clinical presentation and erosion characteristics, but successfully treating this case utilizing only an endoscope highlights the importance of this approach.
Footnotes
Authors' Contributions
L.A.: writing, original draft. P.A.: review and editing. L.B.: review and editing. P.R.: review and editing. M.A.: review and editing. M.G.: writing, original draft, visualization.
Acknowledgment
This article is dedicated to the memory of M.R.G.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.