
Abstract
Laparoscopic sleeve gastrectomies (LSGs) can experience weight-loss failure and conversion to another bariatric procedure. An analysis of the bariatric literature concerning the single anastomosis duodeno-ileal bypass with sleeve gastrectomy (SADI-S) as revisional surgery after LSG in terms of safety and efficacy identified 607 studies. Fifty-nine studies were analyzed for full content review and 9 primary studies (398 patients) were included. Revisional single anastomosis duodeno-ileal bypass (SADI) was performed in 294 patients at a mean interval of 37.7 months (range 11–179). Total weight loss (%) varies from 20.5% to 46.2%. Early complications after surgery occurred in 4.1% surgeries including leak (7 cases −1.9%). Mortality was nil. SADI after LSG, after failed sleeve gastrectomy or as a sequential procedure, offers a satisfactory weight loss result. Both early and late term complications are acceptable.
Introduction
For the past decade, surgical procedures such as laparoscopic sleeve gastrectomy (LSG) have showed their utility for morbid obesity treatment. It has become the most frequently performed bariatric procedure worldwide.1,2 Also, the absence of a large knowledge base of long-term outcomes has demonstrated a need to understand its indications as a sole or combined procedure. The increased number of LSG procedures has led to an increased number of patients experiencing insufficient weight loss or even weight regain after the procedure. Some of them have been proposed for conversion to another bariatric procedure.
Mid- and long-term data are available nowadays, showing a significant increased number of patients with weight regain after LSG.3–10 Weight regain represents the most important long-term complication after LSG and bariatric surgery. 11 That gradual decline in the percentage of weight change has been observed in longitudinal studies. 11 It is also associated with the recurrence of obesity-related comorbidities, including type 2 diabetes. 12 Yet, the etiology of this phenomenon remains largely unknown. There is a lack of knowledge to determine the optimal time and revisional surgery for weight regain after LSG (Table 1). Resleeve gastrectomy (ReSG) has only one clear indication: the presence of large undissected gastric fundus. Certainly, laparoscopic Roux-en-Y gastric bypass (LRYGBP) is the best procedure to treat the reflux disease after LSG. Still, there is important amount of data that in terms of weight loss the LRYGB as revision of LSG is highly disappointing. Single anastomosis duodeno-ileal bypass with sleeve gastrectomy (SADI-S) or stomach intestinal pylorus-sparing surgery (SIPS) as a second stage procedure was introduced more recently, and few results are available for the mid- and long-term results of its utility for the management of weight regain and comorbidities after LSG.
Literature Review of Revisional Surgery After Laparoscopic Sleeve Gastrectomy
BMI, body mass index; DS, duodenal switch; EWL, excess weight loss; LRYGBP, laparoscopic Roux-en-Y gastric bypass; ReSG, resleeve gastrectomy; RYGBP, Roux-en-Y Gastric Bypass; TWL, total weight loss.
The purpose of this review was to analyze the bariatric literature concerning the SADI-S or SIPS as revisional surgery after LSG in terms of safety and efficacy.
Materials and Methods
Search strategy and study selection
PubMed/MEDLINE search was performed to identify articles reporting single anastomosis duodeno-ileal bypass (SADI) as revisional or second step procedure after LSG. Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines were followed for selecting the eligible studies (Fig. 1). The following term combinations were used: (sleeve, revisional), (SADI, SADIS-S, SIPS, sleeve), and (SADI, SADIS-S, SIPS, sleeve, revisional). The reference list of the retrieved articles was also manually checked for relevant articles. The conference abstracts considered “gray literature” were not analyzed. No publication date or language limit was considered for our search strategy.
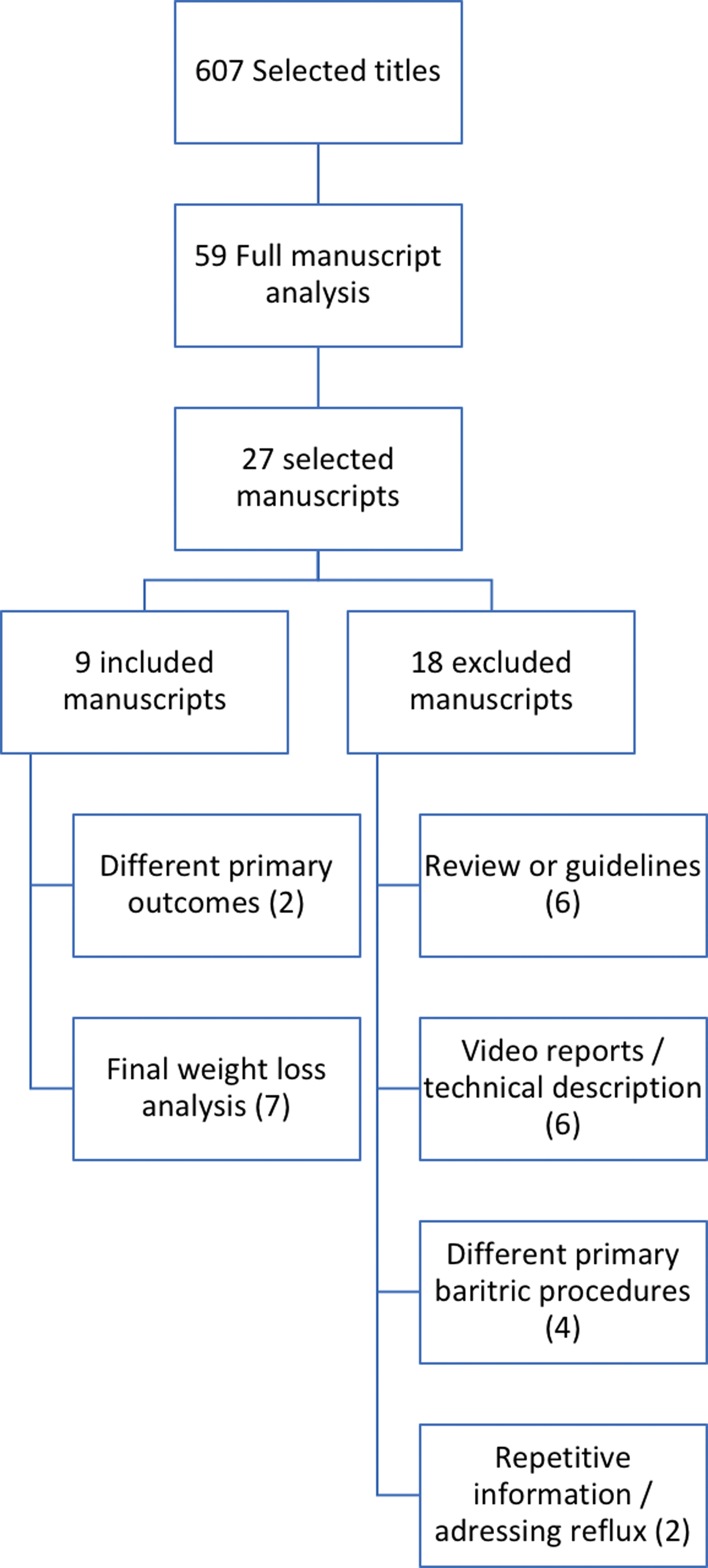
Flowchart of article selection for the review. Color images are available online.
After the literature search, 607 records were identified. Of these, 548 articles were not included after initial screening. All studies of any design that included references of SADI after LSG from 2009 to 2020 were included. A prescreen was included to identify the clearly irrelevant reports by title, abstract, and keywords. Study assessment was performed by 2 other independent authors/reviewers (A.T. and P.N.) reviewing relevance, inclusion, and methodological quality. Reviewers graded as relevant (all specified inclusion criteria met), possibly relevant (some but not all inclusion criteria met), and rejected (not relevant) all extracted titles. Finally, 2 other reviewers (M.N. and R.V.) reviewed the full-text versions of all studies classified as relevant or possibly relevant. Whenever a disagreement appeared, a repeated extraction was done.
Data extraction and management
The reviewers performed a data extraction. Extraction included data from methods (e.g., retrospective case series), demographic characteristics (e.g., age, gender), number of patients, clinical characteristics, rate of conversion, postoperative outcomes, follow-up, and weight loss results. All repetitive information was excluded.
Statistical analysis
An analysis of the data from the included studies was performed including descriptive statistics and treatment-level data. Total number of patients enrolled in the review was used and described. Efficacy outcomes of interest were synthesized. A meta-analysis was not deemed appropriate due to the complete lack of randomized control and the heterogeneity among the studies and trials. All calculations were performed using Stata software (StataCorp, version 10, College Station, TX).
Results
Search results
In the first data extraction, 607 studies were identified applying our search criteria for screening (Fig. 1). Title and abstract were assessed according to our exclusion criteria and 548 articles were removed. Fifty-nine studies remained for full content review. Of the 59 studies, 27 were retained -1 was excluded for repetitive information, 21 1 was excluded for addressing the reflux disease, 22 6 for video reports or technical description.23–28 In the same way, other studies were excluded 6 for their design of literature review or bariatric society statement29–34 and 4 for containing different primary bariatric procedures (gastric banding or Roux-en-Y gastric bypass [RYGBP]).35–38 Thus, a total of nine primary studies meeting the inclusion criteria were identified after a careful screening and summarized in Table 2. Two retrospective studies39,40 included cases of revisional SADI for failed LSG, but the primary outcomes of the studies included incomplete or mixed data regarding the weight loss and their outcomes concerning the weight loss were retrieved. Consequently, in the final weight loss analysis, six retrospective case series41–47 were included.
Literature Review for Single Anastomosis Duodenojejunal Bypass
BMI, body mass index; DS, duodenal switch; EWL, excess weight loss; F, female; LSG, laparoscopic sleeve gastrectomy; M, male; MGB, minigastric bypass; N/A, not available; Pts, patients; LRYGBP, laparoscopic Roux-en-Y gastric bypass; SADI, single anastomosis duodeno-ileal bypass; SADI-S, single anastomosis duodeno-ileal bypass with sleeve gastrectomy; TWL, total weight loss.
Included studies
A total of 398 patients were assessed in 9 studies, and the number of patients included in the different articles ranged from 9 to 96. For 368 patients, the average patient age was 43.7 years old (range 18–66). The gender was analyzed for 241 patients, and 182 out of the patients were women (75.5%). The revisional SADI after LSG was performed at a mean interval of 37.7 months (range 11–179) after the primary procedure for 294 patients.
Analyzing the initial body mass index (BMI) before the primary procedure, the number of superobese patients (BMI >50 kg/m2) was clearly reported in only two articles and it represented 56 patients out of 72 (77.8%). After SADI, the total weight loss (TWL) is highly variable from 20.5% reported by Zaveri et al. 39 for 27 patients out of 51 at 24 months after the revisional SADI to 46.2% at the same interval when the results of LSG are also included. 36 A total of 13 patients (only two studies reported it) underwent resizing of the gastric tube with concomitant resleeve with the SADI.
Analyzing 368 patients for the occurrence of early complication after surgery, we have identified 15 patients (4.1%) with early complications after revisional SADI. The most common reported complication was the leak (7 cases −1.9%). The mortality rate was nil.
Discussion
To our knowledge, this is the first review of the literature grouping clinical data from patients who underwent SADI as revisional procedure after failed LSG or two-step procedure. The definition of failure in bariatric surgery is quite challenging. In their survey, Rogula et al. 48 reported a lack of clear definition to describe weight regain after LSG. The common definition is an increase of at least 10 kg from nadir weight. However, that increased weight gives poor information and significance of the amount of weight regained for a patient. Other measurements such as BMI, percentage excess weight loss (%EWL), or total weight change (ΔTW) may be more clinically meaningful and useful in giving clear results toward the effectiveness of a bariatric procedure and socially when deciding a revisional procedure after a primary procedure. A clear distinction must be made between two types of weight loss failure: progressive weight regain after successful weight loss (nadir weight acceptable) and insufficient weight loss (18 months after surgery). Progressive weight regain occurs after achievement of an initial successful weight loss (defined as %EWL >50%) and insufficient weight loss represents a %EWL of <50%. Authors should be encouraged to refrain from grouping together patients with insufficient weight loss and weight regain.
SADI-S was initially proposed as a simpler procedure due to its lower perioperative complication rates and to its hypothetically favorable impact on nutritional status compared with duodenal switch.21,49,50 Even though performed as a revisional procedure, our review found a leak rate of only 1.8% that will probably decrease even more with time and experience. Three studies39,44,46 reported a 0% leakage rate both for duodenal stump and duodenoileal anastomosis. The low complication rate could be explained by several factors: a good standardization of the technique (especially after the learning curve), the anastomosis is performed in a previous undissected area, and easier technical conditions on a patient who has lost a significant amount of weight after LSG.
There is no consensus about which technique should be performed after LSG as a second-step procedure. However, LRYGBP, minigastric bypass—one-anastomosis gastric bypass and resleeve are commonly considered as “easier” alternatives for SADI. Few reports13–20 are comparing all these procedures with a clear superiority concerning the weight loss results for SADI. The overall results appear to be positive, especially considering that our series includes both super obese and sleeve gastrectomy (SG) failed patients. These types of patients are those who have a poor response to bariatric surgery. This particular observation could explain the better results reported when SADI-S is performed as a single-stage procedure 51 and confirmed with long-term (6 years) follow-up. 52 Weight loss after revision of LSG to LRYGBP is so disappointing, with a TWL varying from 6.5% to 19.3% at 36 months after the revisional surgery.16,17
Isolated ReSG represents an option as revisional procedure after LSG only in case of undissected fundus as it has been described by Noel et al. 20 with an excess BMI loss of 63.7% at 5 years follow-up. In our review, concomitant ReSG with SADI was reported in two studies40,41 for 3 and, respectively, 10 patients, but it was highly unreported in the other studies.
The term of SIPS was advocated by Cottam et al. in different publications.53,54 The surgical technique is similar to the SADI and for both of them variations exist only for the length of the common channel and the bougie size used to perform the LSG. In one of their articles, 53 they have compared the SIPS with RYGBP, finding a similar weight loss result up to 18 months, past that SIPS showed statistically significant better results. They have reported more long-term classes IIIb–V complications, classes I–IIIa complications, reoperations, ulcers, small bowel obstructions, nausea, and vomiting with the LRYGBP than the SIPS. In another article, 54 they have compared SIPS with classical duodenal switch having similar results in terms of weight loss but fewer complications for SIPS after 2 years.
The main concern about adding a hypoabsorptive technique after LSG is achieving an acceptable weight loss without provoking denutrition. Considering a follow-up rate ∼10% (only 1 patient at 36 months) 39 or results reported at only 12 months, 42 any discussion about denutrition should be taken into account very carefully and consecutively our current review is not analyzing the nutritional deficiencies. Certainly, SADI is a hypoabsorptive procedure, and patients should be adequately supplemented and followed for life. The relationship between common channel length and nutritional disturbances could seem to be clear. Meticulous total bowel length measurement, especially in revisional cases, could represent a solid recommendation. During the initial phase of the experience with SADI, many teams have modified the length of the common channel with no severe nutritional abnormalities observed if a 300-cm common channel was created. The need to revise a SADI procedure was identified in two studies, for 1 patient with chronic liver disease 46 and 3 patients with severe hypoalbuminemia. 41 Different technical options have been proposed, such as tailoring a common channel and converting SADI to normal anatomy. For clear malnutrition, the SADI-S procedure will require an elongation of the common channel, adding 100 to 150 cm. When performing that procedure, newer duodenoileostomy should not be considered close to the Treitz ligament, in which case weight regain will be present. The conversion to LRYGBP, as a successful revisional surgery option in complex cases, has been published recently by Vilallonga et al. 55 The overall idea is that we need to tailor the small bowel to the need of each patient, considering 200 cm too short and 300 cm maximum for SADI.
One of the major limitations of our review is represented by the impossibility to clearly identify the patients who were scheduled for a planned second stage procedure or patients with weight regain and revisional surgery. Timing of the revisional surgery should be better analyzed in future studies as it might impact on the overall result, as well as the initial BMI before the primary LSG. Only three articles have reported the initial BMI and the number of superobese patients (BMI >50 kg/m2). Also considering the enormous disparities for the weight loss results, no attempt of analysis was done to assess the comorbidities. Moreover, as the majority of patients included in the analyzed studies are patients with revisional surgery, the percentage of presence of comorbid conditions is less important than for the primary cases. Finally, there is an important heterogeneity of the measurements of the limb length according to each author and the historical time when SADI was performed.
Few other limitations of our review were identified, and they can be used as recommendations for further publications that will report the results of SADI as revisional or second step surgeries after LSG. One of the publications 40 with important number of procedures (181 cases) is mixing the results in terms of complications or weight loss results for the primary SADI with the revisional or second stage procedure. Equally important the definition of complications is highly variable with no clear distinction between early and late complication. Late complications related to weight loss are difficult to define. As an exemple, some authors consider ReSG after a SADI a late complication. 43
Conclusions
SADI after LSG, either as a secondary procedure after failed SG or as a sequential procedure in super obese patients, offers a satisfactory weight loss result. Neither early nor late complications should represent a limitation to offer this revisional procedure for patients with weight loss failure after LSG, especially in the absence of gastroesophageal reflux disease.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.