
Abstract
Background:
Virtual reality (VR) experience is the most adopted form of video-gaming to reduce preoperative anxiety. This prospective randomized clinical trial aimed to examine the feasibility and efficacy of preoperative VR experience in children undergoing elective surgery.
Materials and Methods:
All patients older than 13 years and scheduled for elective surgery between March and June 2021 were enrolled. Preoperative VR experience consisted in watching a 5-minute video using a head-mounted display. Four parameters were evaluated and compared between the two groups: (1) patient heart rate (HR) before anesthesia; (2) patient evaluation of preoperative anxiety using facial affective scale (FAS); (3) anesthesiologist evaluation of preoperative anxiety using FAS; and (4) subjective stress scoring using a 5-item Likert-type scale.
Results:
A total of 40 patients (23 boys) with a median age of 14.5 years (range 12–17) participated in the study. The patients were randomized in two groups, each of 20 patients, according to preoperative VR experience: VR group (G1) and control group (G2). No adverse events related to VR occurred. The patient median HR was significantly lower in G1 (72 bpm) than in G2 (101 bpm) (P = .001). The very relaxed/relaxed face selection rate using FAS was significantly higher in G1 than in G2, in both patient and anesthesiologist evaluations (P = .001). Finally, the subjective patient scoring of operating room experience was significantly greater in G1 [4.6 ± 0.4] than in G2 [2.15 ± 1.07] (P = .001).
Conclusions:
Our preliminary results showed that VR is safe and effective to relieve anxiety and improve relaxation in the preoperative period in pediatric patients undergoing elective surgery. The VR experience resulted in decreased overall anxiety and increased overall positive affect during the preoperative period in VR group compared with the control group. Further studies are needed to investigate this technology in the postoperative phase and on a larger patient cohort.
Introduction
Preoperative anxiety and distress are common issues in children undergoing surgical procedures. 1 Clinical manifestations of anxiety are different, such as agitation, crying, shivering, fighting, and escape behavior, and have been associated with adverse clinical and psychological consequences for children and their families, including increased postoperative pain, delirium, nocturnal enuresis, and separation anxiety.2,3 For this reason, increasing attention is currently being paid to techniques aiming to reduce preoperative anxiety and its associated outcomes. Various methods to reduce anxiety, including premedication, parental presence during induction of anesthesia, have been evaluated for this purpose.4,5
Distraction is a commonly applied intervention before surgical procedures. For example, the use of music, books, or streamed video clips has proven to be effective in reducing distress and anxiety in the preoperative phase. 6
Virtual reality (VR) is an advanced technology that allows users to immerse themselves in a three-dimensional (3D) computer-generated world.7,8 VR gaming using head-mounted display (HMD) is currently the most adopted form of active video-gaming available on the market.9–12 This system seems extremely appropriate in children, who routinely play videogames using consoles or smartphones.
Analyzing the international literature, most of articles describing the outcome of VR experience were focused on adult patients undergoing chemotherapy for cancer or after burns or trauma.13–17 The use of VR in the pediatric population has been introduced more recently with the purpose to relieve pain during dressing change or for neuropsychological rehabilitation.18,19 Few articles reported preliminary experience about the use of VR in pediatrics in the operating room (OR) setting.20,21
Our team is working in more recent years for the humanization of pediatric OR, and we hypothesized that adopting a VR experience in our pediatric patients would improve their approach to the surgical procedure. So, we created a VR pediatric program, and the first step of this program was to adopt VR with use of HMD in pediatric patients in the preoperative phase.
This randomized clinical trial (RCT) aimed to examine the feasibility and efficacy of VR experience in the preoperative phase in pediatric patients undergoing elective surgery.
Materials and Methods
This RCT was approved by the appropriate Institute Review Board.
All children and parents/guardians received adequate explanation of the study protocol before admission.
Written informed consent was obtained from parents/guardians of all children before or the same day of surgery, and assent was also obtained from children aged 12 years or older. Parents and patients were informed that in case of pre-existing medical conditions such as binocular vision abnormalities, psychiatric disorders, seizures, or other serious medical conditions, the use of VR was contraindicated.
Patients
The use of HMD adopted in this study is not advised in children under the age of 13 years. For this reason, we enrolled all patients older than 13 years of age who were scheduled for elective surgery under general anesthesia in our surgical unit for a 4-month period (March to June 2021).
Exclusion criteria included major surgery or needing for postoperative intensive care, history of prematurity or congenital disease, heart conditions, hearing impairment, pre-existing binocular vision abnormalities, cognitive deficits or psychiatric disorders, assumption of psychoactive medications, and history of epilepsy or seizure.
Furthermore, the headset and controller may contain magnets or components that emit radio waves, which could affect the operation of nearby electronics, such as cardiac pacemakers, hearing aids, and defibrillators, and its use may cause persistent interference with these medical devices.
Sample size and randomization
It was calculated that a minimum sample size of 20 participants per group was needed, with a significance level of 0.05 (α = 0.05) and an 80% power (β = 0.20), allowing for a 10% dropout rate.
Randomization and patient allocation were performed by an independent clinician not otherwise involved in the trial using simple random sampling method, which entailed an equal number of opaque envelopes prelabeled with VR experience (G1) and no VR experience (G2) and picked before the surgical procedure.
The outcome assessor was blinded to group assignment, although children and their parents/guardians were not blinded.
VR experience
A VR system consisting of a computer-generated environment, in which orientation and 3D interaction are possible, was adopted in this study. This environment was projected right in front of the patient's eyes through advanced HMD, including a wide field of view and motion tracking systems. The HMD was also integrated with an earphones system and touch controllers (Fig. 1). To reduce the risk of discomfort, the headset was balanced and centered, and the distance between the lenses (the intra-axial distance, or IAD) was appropriately set for each user.
The head-mounted display for virtual reality was integrated with touch controllers. Color images are available online.
Patients, who were candidate to VR experience before surgery, were accompanied by the parents/guardians in the OR without premedication and were always assisted by a pediatric surgeon resident during the VR experience (Figs. 2 and 3). The VR experience consisted of watching a 5-minute 360° movie using the HMD, which was chosen by the patient. The VR experience was performed at least 30 minutes before entering the OR.

A female patient wearing the head-mounted display during virtual reality experience in the operating room assisted by a pediatric surgeon resident. Color images are available online.

A male patient wearing the head-mounted display during virtual reality experience in the operating room assisted by a pediatric surgeon resident. Color images are available online.
Outcomes
A single-blinded assessor collected the scores to maintain data uniformity.
Four parameters were evaluated: (1) patient heart rate (HR) before anesthesia; (2) patient evaluation of preoperative anxiety using facial affective scale or FAS (Fig. 4); (3) anesthesiologist evaluation of preoperative anxiety using FAS; and (4) subjective patient scoring of experience in the OR on a 5-item Likert scale: (1) extremely stressing, (2) stressing, (3) indifferent, (4) relaxing, and (5) extremely relaxing. The two groups were compared regarding all parameters evaluated.
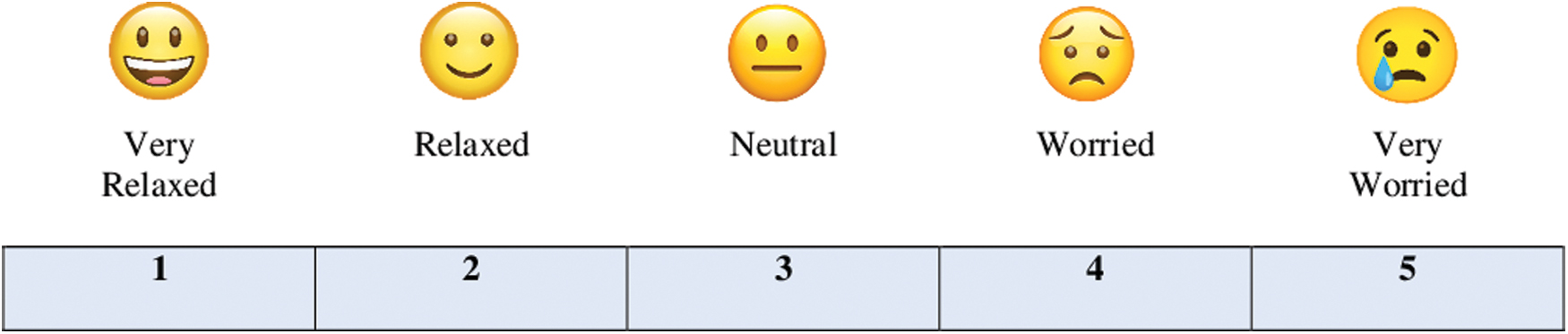
Facial affective scale for evaluation of preoperative anxiety. Color images are available online.
Statistical analysis
Statistical analysis was carried out using the Statistical Package for Social Sciences (SPSS Inc., Chicago, IL), version 13.0. Continuous data were summarized and presented as median and interquartile range. The categorical variables were presented as absolute numbers and percentages.
The categorical variables were analyzed using chi-squared test and the continuous variables were measured using the parametric Student's t-test. P value <.05 was considered statistically significant.
Results
Of the 45 candidates who were asked to be enrolled in the study the same day of surgery or the day before, five declined to participate. A total of 40 patients, who fulfilled the inclusion criteria, participated in the RCT. There were 23 boys and 17 girls with a median age of 14.5 years (range 12–17). All patients were scheduled for an elective surgical procedure under general anesthesia for different surgical pathologies. The patients were randomized in two groups: VR group (G1) included patients 1–20 who performed the VR experience preoperatively and control group (G2) included patients 21–40 who did not receive the VR experience (Fig. 5).
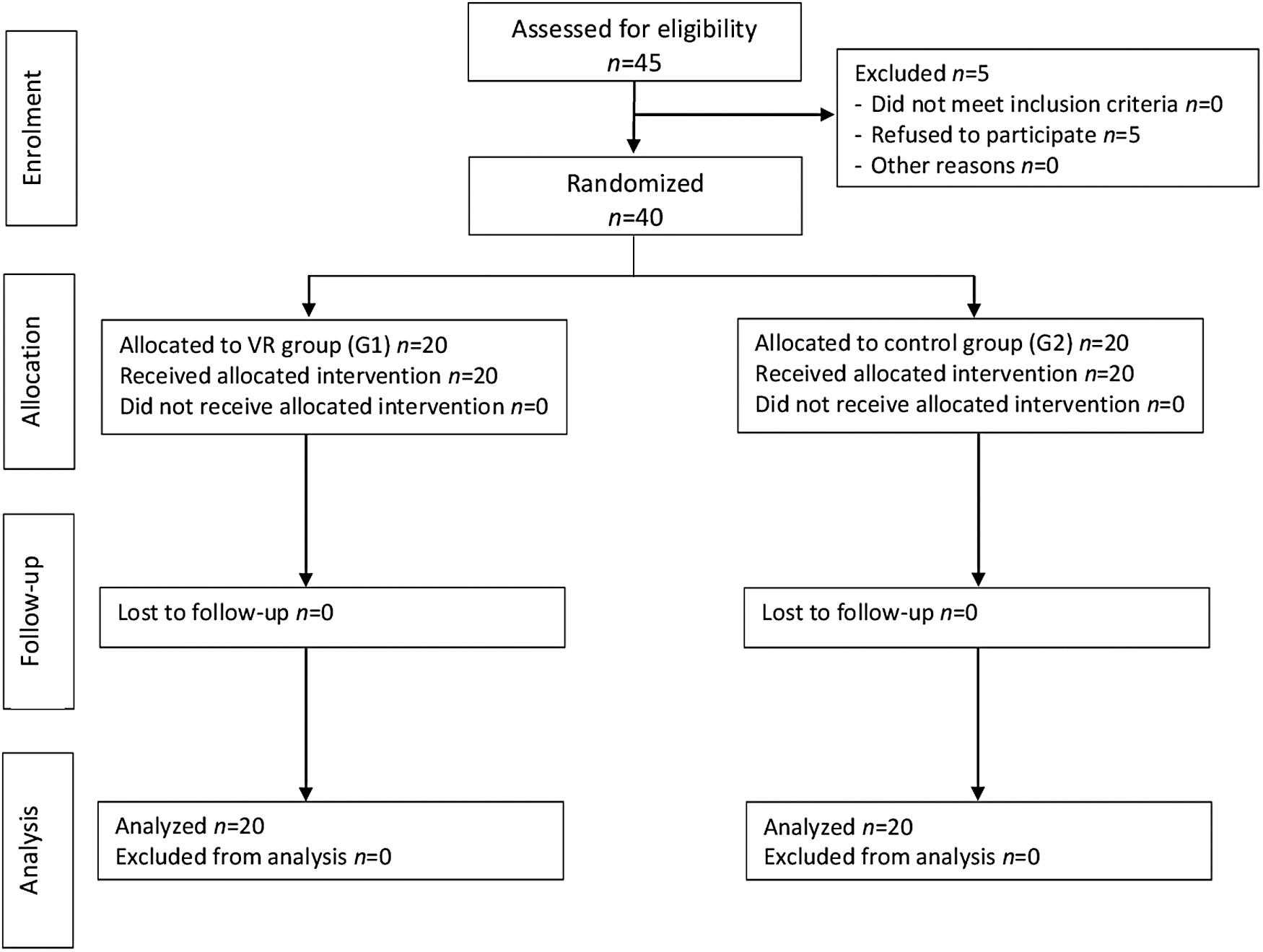
CONSORT diagram for the randomized clinical trial. VR virtual reality.
No statistically significant differences were seen in patient characteristics, including age, gender, weight, and the American Society of Anesthesiologists (ASA) Physical Class between the two groups. The median patient age was 15 years (range 14–17) in the VR group and 14 years (range 12–15.5) in the control group. Both G1 and G2 groups were similar with respect to median anesthesia time and operating time (Table 1).
Patient Characteristics
ASA, American Society of Anesthesiologists; F, female; M, male; VR, virtual reality.
No adverse events related to VR experience, including altered, blurred, or double vision or other visual abnormalities, dizziness, disorientation, impaired balance, nausea, discomfort or pain in the head or eyes, occurred. All patients completed successfully the VR experience.
Regarding the parameter 1, the median patient HR was significantly lower in G1 (72 bpm) than in G2 (101 bpm) (P = .001). Regarding the parameters 2 and 3, the rate of very relaxed/relaxed face (1 and 2) selected by the patient using FAS was significantly higher in G1 [18/20 (90%)] than in G2 [2/20 (10%)] (P = .001). As well, the rate of very relaxed/relaxed face selected by the anesthesiologist using FAS was significantly higher in G1 [19/20 (95%)] than in G2 [1/20 (5%)] (P = .001). Finally, with respect to the parameter 4, the subjective scoring of OR experience assigned by the patients was significantly greater in G1 [4.6 ± 0.4 (range 3–5)] than in G2 [2.15 ± 1.07 (range 1–5)] (P = .001).
All outcome parameters are reported in Table 2.
Outcome Parameters
FAS, facial affective scale; HR, heart rate; n/a, not applicable; OR, operating room; SD, standard deviation; VR, virtual reality.
Discussion
About 200,000 pediatric patients undergo surgery in Italy every year, and the majority of these children, even those well prepared and with a positive attitude, experience stress and anxiety in the OR. 22 In particular, anesthesia induction is considered to be the most anxiety provoking part of the preoperative experience.1,2 It has been reported that preoperative anxiety not only causes distress in children before surgery but is also associated with a negative postoperative behavior changes, a slower recovery, sleep disturbances, and eating difficulties.20,23
Several procedures or techniques have been described to reduce preoperative anxiety in pediatric patients as use of premedication, parental presence, and pain or anxiety management interventions,22–24 but none of them has been proven to completely relieve such issue in the preoperative phase.
VR has emerged for the past years as a promising alternative to drugs to relieve preoperative anxiety and distress in both adults and pediatrics.20,21,25 VR provides the patient a visual, auditory, and tactile stimulation within a 3D environment, allowing child to perform an immersive experience in another world and forget to be into the OR. The patient has two main possibilities: to watch movies in a 3D environment or to use 1 or 2 touch controllers and interact with his hands in the 3D videos or playing 3D videogames in a VR environment.
Analyzing the international literature, several applications of VR for different medical purposes have been described in adults,13–17 but only few pediatric reports have been published.20,21
In particular, VR was adopted in pediatric oncology patients.26,27 There is emerging evidence that VR technology may improve patient emotional well-being, reduce medical procedural distress through realistic and educative exposure to actual procedures through virtual simulation, and provide a great support to prepare child and families for radiation therapy and chemotherapy.26,27 Other studies showed that VR was an effective distraction tool and increased satisfaction from anxiety management in children undergoing intravenous catheterization in the emergency department or dressing changes. 19
In view of the humanization program of our Pediatric Surgery Unit, supported by General Health Management of our University Hospital, we established a VR program in our surgical practice. We decided to adopt VR technology in the OR because, after a careful literature review, we found that VR has been proven to reduce both pain and anxiety in pediatric patients receiving both surgical and medical procedures.18–21
In our study, VR experience was provided using a HMD, which is the most adopted tool for VR intervention-based studies. The main finding of our study was that the use of a VR experience during the access to the OR significantly reduced anxiety and improved compliance during the induction of anesthesia in children compared with the conventional method. It is also important to underline that this technology was clinically safe with no adverse events related to VR experience occurred in this series.
All patients, who experienced the VR in our study, were overwhelmingly enthusiast of this experience. The efficacy of the VR experience to reduce patient anxiety and discomfort before anesthesia and surgery was assessed using objective parameters such as the HR, which was significantly lower in VR patients compared with control patients, from the entry in the operative theatre until the induction of anesthesia. The preoperative anxiety was assessed by both patient and anesthesiologist, and an inter-evaluator similarity was found in the results. In fact, the rate of very relaxed/relaxed face (1 and 2) using the FAS score was significantly higher in VR patients than in control patients, in both patient and anesthesiologist evaluations.
Finally, all VR patients defined their experience in the OR using the VR technology as relaxing or extremely relaxing whereas the majority of patients, who accessed to the OR in the conventional way, defined their surgical experience as stressing.
Based on our preliminary experience, we can provide some recommendations for implementing the HMD VR experience in the pediatric patients. Before starting the VR experience, the patient may need positive verbal encouragement to enhance his/her motivation to try this experience. During HMD game-play, the patient requires the support from a pediatric surgery resident and should begin the VR experience, playing an introductory game or more exploratory games with minimal required activity or movement. It is also important during the introductory session, to set accurately the movement boost and location of the controllers within the VR software while the person is playing the game.
This study has some limitations. First, preoperative anxiety and satisfaction scores of patients were assessed without evaluating their background and abilities to understand anesthesia and surgical procedures. Second, the effects of VR experience on postoperative agitation, pain, or maladaptive behaviors were not investigated in this study. Finally, children in this study performed their VR experience at least 30 minutes before entering the OR; further research on the optimal timing of the VR intervention should be performed.
However, this is only the first step of our program of application of VR technology in pediatric surgical patients and next steps of our program will be to use VR in the postoperative period and in patients recovered in pediatric intensive care unit.
Conclusion
Our preliminary results showed that VR is safe and effective to relieve anxiety and improve relaxation in the preoperative period in pediatric patients undergoing elective surgery. The VR experience resulted in decreased overall anxiety and increased overall positive affect during the preoperative period in VR group compared with the control group. However, further studies are needed to investigate this technology in the postoperative phase and on a larger patient cohort.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this study.