
Abstract
Introduction:
Sleeve gastrectomy engenders weight loss and improves comorbidities at 1 year postoperatively. A relationship has not been established between liver pathology and diabetic outcomes and weight loss following a sleeve gastrectomy. This study evaluates the association between liver pathology and both diabetic remission and weight loss in morbidly obese veterans.
Methods:
A prospective database of all patients undergoing sleeve gastrectomy with simultaneous liver biopsy at a Veterans Affairs Medical Center was analyzed from 2018 through 2020. The database included patient demographics, liver biopsy pathology, laboratory values, and antihyperglycemic medications. Patient outcomes at 12 months postoperatively were analyzed specifically for diabetic resolution and weight loss. Chi-square test and Fisher's exact test were used for categorical comparisons, and one-way analysis of variance test and two-tailed t-test were used for continuous variable comparisons. Multivariate linear regression models were created to assess the association between liver pathology and changes in body mass index (BMI) and diabetic status. A two-sided P-value of 0.05 indicated significance.
Results:
Of the 77 patients included in the study, 70.1% of patients achieved diabetic remission at 12 months. After condensing steatosis and fibrosis scores into low- and high-grade categories, patients with no hepatic disease had significantly lower BMI at 12 months postoperatively than patients with low- or high-grade hepatic disease (29.2 ± 3.6 kg/m2 versus 35.1 ± 4.0 kg/m2 versus 34.5 ± 3.7 kg/m2, respectively, P = .009). On multivariate linear regression model, low-grade overall hepatic disease (β = 3.1 ± 1.5; P = .043) and preoperative oral glycemic medications (β = 2.4 ± 1.0; P = .026) were associated with a significantly increased 12-month BMI. Also, Black or African American race compared with White race was associated with a significant decrease in postoperative BMI (β = −1.9 ± 0.8; P = .023).
Conclusions:
Regardless of preexisting liver disease, most diabetic patients who undergo sleeve gastrectomy experience diabetic remission at 12 months postoperatively. Additionally, patients with no underlying liver disease lose more weight than those with low- or high-grade liver disease.
Introduction
Recent surveys reveal that a staggering 42.1% of American adults are obese, and this number is increasing annually. 1 Concurrently, the prevalence of type II diabetes (T2DM), nonalcoholic steatohepatitis (NASH), and nonalcoholic fatty liver disease is rising. Some authors suggest that insulin resistance is the denominator for the relationship between these comorbidities and a shared pathophysiology.2–4 Peripheral insulin resistance is characterized by an accumulation of lipids in skeletal muscles, elevated plasma free fatty acids (FFAs), and impaired adipose tissue lipolysis. 5 As a by-product of insulin resistance, elevated plasma FFAs are deposited in the liver and lead to steatosis, which in turn causes further systemic insulin resistance. This cycle continues endlessly with impaired glucose metabolism.2–4,6
The pathophysiological relationship between obesity, T2DM, and hepatic steatosis is substantiated by studies that demonstrate remission rates of diabetes and NASH following bariatric surgery. Following a sleeve gastrectomy, T2DM may resolve in up to 83% of morbidly obese patients at 1 year. 7 From a hepatic standpoint, NASH may resolve in up to 85% of morbidly obese patients at 1 year. 8 Due to these findings, some investigators report a link between these two processes since a preoperative biopsy documenting steatohepatitis improves a patient's chances of long-term diabetic remission following bariatric surgery. 9 This study analyzes a large series of morbidly obese Veterans to establish a potential relationship between liver pathology, weight loss, and diabetic remission following a sleeve gastrectomy.
Patients and Methods
All patients undergoing a sleeve gastrectomy with a liver biopsy from January 2018 to August 2020 were included in the study. IRB approval was obtained and maintained throughout the study. Baseline demographics and clinical features were recorded, including age, gender, race, preoperative body mass index (BMI), presence of diabetes, preoperative Hemoglobin A1c (HgbA1c), and whether the patient was on oral antihyperglycemics, metformin, or insulin. Race and ethnicity were recorded through the electronic health record. These data are acquired via self-reporting, proxy reporting, or during registration. Patients may select between the following race categories: American Indian or Alaska Native, Asian, Black or African American, Native Hawaiian or Other Pacific Islander, White, or Unknown by Patient. Individuals were categorized as Black or African American and White due to small sample sizes in the remaining racial categories.10–12
All patients underwent a sleeve gastrectomy with an intraoperative liver biopsy utilizing our technique, which has been described previously. 13 All liver biopsies were obtained using the ultrasonic shears with a typical size of 2 × 1 × 1 cm. All biopsies were sent for pathological review. BMI, HgbA1c, and diabetic medications were recorded postoperatively at 6 and 12 months.
Hepatic histopathology was graded for steatosis and fibrosis both independently and combined for a total liver disease score. Liver histology was performed according to the METAVIR classification. 14 Briefly, steatosis was scored as 0 = none, 1 = mild (<10% hepatocytes), 2 = moderate (10%–30% hepatocytes), and 3 = severe (>30% hepatocytes). Fibrosis was scored on a scale of 0–4 with 0 = no fibrosis, 1 = perisinusoidal/pericellular fibrosis only, 2 = perisinusoidal/pericellular fibrosis with periportal fibrosis, 3 = perisinusoidal/pericellular fibrosis with periportal fibrosis and bridging fibrosis, and 4 = cirrhosis.
The patients' pathological scores were also recorded as a total of their combined liver steatosis and fibrosis scores. Any patient with a total score of 0 was considered to have no liver pathology. Any patient with a combined total score of 1–2 was considered to have low-grade liver disease, and any patient with a combined total score of ≥3 was considered to have high-grade liver disease.
All patients were followed postoperatively with clinic visits every 3, 6, 9, and 12 months. Analysis was limited to those patients with at least 12 months of follow-up.
Statistical methods
Patients were dichotomized into diabetic and nondiabetic groups. These categories were assessed postoperatively at 6 and 12 months. Resolution of diabetes was determined if either (i) a patient discontinued diabetic medication (antihyperglycemic, metformin, and/or insulin) or (ii) HgbA1c reduced to ≤6.5. Primary endpoints were 6- and 12-month postoperative resolution of diabetes. Additional analysis included change in BMI over the 12-month period.
Patient demographics and clinical outcomes were stratified by biopsy results (none, low grade, or high grade) and category (steatosis, fibrosis, and overall). Chi-square test and Fisher's exact test were used for categorical comparisons with adequate cell counts and low cell counts (>25% of expected cells counts ≤5), respectively. One-way analysis of variance test and two-tailed t-test were used for continuous variable comparisons.
Multivariate linear regression models were created to assess the potential association between liver pathology and changes in BMI and diabetic status. One such model analyzed BMI at 12 months, whereas a second model analyzed BMI change over the same 12-month period. These models controlled for demographic and clinical characteristics, including age, race, sex, and preoperative variables. Corresponding parameter estimates (β), standard error, and P-values are reported. All statistical analyses were performed using SAS version 9.4 (Cary, NC, USA), and a two-sided P-value of 0.05 indicated significance.
Results
Over the 12-month study period, a total of 105 patients underwent sleeve gastrectomy. Of these patients, a total of 77 patients met the inclusion criteria, having proper glycemic follow-up with an intraoperative liver biopsy. The demographic and intraoperative biopsy scores are summarized in Table 1. Of the patients enrolled in the study, 45.5% were male, a majority were identified as Black (57.1%), the mean age was 48.5 years (±10.3), and the mean preoperative BMI was 40.7 kg/m2 (±2.8). Preoperatively, 48.1% of the patients had T2DM, of which 15.6% were taking oral hypoglycemic medications and ∼10% were using insulin. The mean HgbA1c was 6.2% ± 1.1. Most patients (57.1%) presented with low-grade steatosis or overall low-grade scoring, whereas 44.2% of patients showed evidence of low-grade fibrosis. Approximately one-quarter of patients had high-grade steatosis, fibrosis, or overall high-grade scoring.
Patient Demographics, Labs, and Liver Pathology
BMI, body mass index; SD, standard deviation.
The vast majority (70.1%) of patients encountered some form of glycemic success (discontinued oral glycemic agents or insulin or demonstrated a decreased HgbA1c at 12 months) after a sleeve gastrectomy. When stratified by overall grade (combined fibrosis and steatosis scores), there was a significant difference in the distribution of postoperative BMI and decrease in BMI at 12 months (P = .009 and P = .037, respectively; Table 2). Patients without fibrosis or steatosis had a significantly lower absolute BMI at 12 months (29.2 ± 3.6 kg/m2) compared with overall low-grade (35.1 ± 4.0 kg/m2) and high-grade (34.5 ± 3.7 kg/m2) patients (P = .009). Additionally, patients without any appreciable fibrosis or steatosis had a significantly greater decrease in BMI at 12 months, averaging a 9.4 ± 3.6 kg/m2 decrease, compared with a 5.5 ± 2.9 kg/m2 decrease in low-grade patients and 5.9 ± 3.4 kg/m2 decrease in high-grade patients (P = .037). These findings are demonstrated in Figure 1.
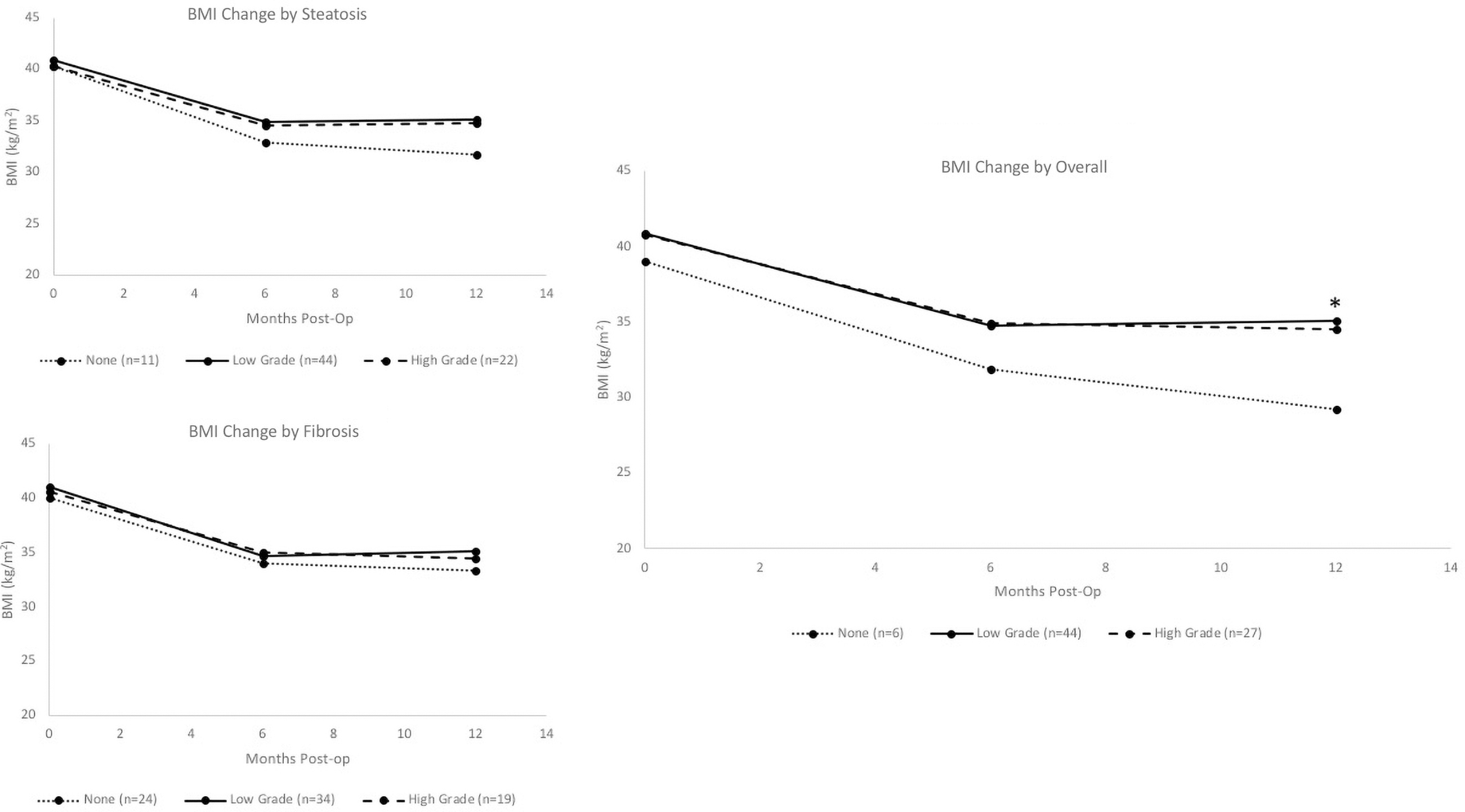
BMI change over 12 months separated by liver pathology category. BMI was significantly lower in patients without liver disease (P = .037). *Statistically significant difference, P < .05. BMI, body mass index.
Clinical Outcomes Based on Liver Pathology
BMI, body mass index; SD, standard deviation.
Logistic regression analysis was conducted to determine factors that predicted overall glycemic success. When controlling for age, sex, race, BMI, and biopsy status, the presence of diabetes preoperatively was the only variable that significantly predicted diabetic success after a sleeve gastrectomy (adjusted odds ratio = 6.1 [95% confidence interval 1.6–23.6], P = .008). Otherwise, there were no significant variables that predicted diabetic resolution.
Multivariate linear regression models were used to determine variables that predicted changes in 12-month BMI (Table 3). The model controlled for age, sex, diabetes, preoperative insulin, and HgbA1c. Compared with no evidence of steatosis or fibrosis, low-grade hepatic disease was associated with a significant increase in BMI (β = 3.1 ± 1.5; P = .043). Preoperative oral hypoglycemic medication was also associated with a significant increase in BMI when compared with patients not taking these medications (β = 2.4 ± 1.0; P = .026). When compared with patients who identified as White, patients who identified as Black had a significantly greater decrease in BMI (β = −1.9 ± 0.8; P = .023).
Predictive Variables for 12 Month BMI
SE, standard error.
Discussion
Glycemic improvement not correlated with liver disease
Our data demonstrated that patients who underwent sleeve gastrectomy with concomitant liver biopsy had a 70.1% chance of improvement or complete remission of their diabetes 1 year postoperatively. The improvement in diabetic status did not significantly correlate with underlying liver disease. This contrasts with other studies which found that preexisting liver disease correlated with diabetic remission. 9 Vangoitsenhoven et al. demonstrated that diabetic remission improved following a Roux-en-Y gastric bypass (RYGB) in patients with a higher incidence of liver steatosis. These results combined with our findings suggest that overall weight loss confers improvements in glycemic pathophysiology regardless of the bariatric procedure or the presence of liver disease.
Weight loss secondary to any intervention may simply break the cycle of peripheral insulin resistance by reducing lipid deposition in skeletal muscles, plasma FFAs, and adipose tissue lipolysis. Ultimately, these changes predicated through weight loss improve glycemic control regardless of liver status.
Better weight loss with a healthy liver
Although there was no correlation between liver disease and diabetes remission, there was a relationship between liver disease and weight loss. Specifically, patients without liver disease had statistically significantly more weight loss than patients with underlying liver disease. This suggests that the underlying pathophysiology of the metabolic syndrome has hormonal and regulatory centers, which are distinct from the stomach. In other words, the same restrictive procedure does not confer the same weight loss in morbidly obese patients with inflammatory sequelae of the liver. These findings are important to set patient expectations postoperatively. At this time, the data are insufficiently powered to delineate a definitive answer regarding the disparity in weight loss between morbidly obese patients with and without liver disease.
Conclusions
Compared with Roux-en-Y gastric bypass patients, morbidly obese patients undergoing sleeve gastrectomy did not demonstrate a relationship between preexisting liver disease and diabetes remission. Also, morbidly obese patients without liver disease had significantly greater weight loss than those with preexisting liver disease.
Footnotes
Authors' Contributions
All persons who meet authorship criteria are listed as authors, and all authors certify that they have participated sufficiently in the work to take public responsibility for the content, including participation in the concept, design, analysis, writing, or revision of the article. Furthermore, each author certifies that this material or similar material has not been and will not be submitted to or published in any other publication before its appearance in the Journal of Laparoendoscopic & Advanced Surgical Techniques.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.