
Abstract
Introduction:
Staple line oversewing (SLO) is a prophylactic alternative due to its low cost and its effect of decreasing the incidence and severity of bleeding complications in sleeve gastrectomy (SG). However, this approach significantly increases the surgical time and may be associated with stenosis. The study aims to identify whether its usage was sufficient to optimize the surgical time in patients whose screening for the risk of occult bleeding was negative.
Materials and Methods:
The study enrolled 103 patients. Having the systolic blood pressure goal of 140 mmHg, the staple line is checked for bleeding points, counting as follows: >5 bleeding points proceed to SLO, <5 bleeding points are managed using clips, and if no bleeding points are found, the procedure can be completed.
Results:
The bleeding test was positive in 79.6% of the cases and oversewing was necessary for 44.7% of the total. The bleeding test result was significant for the increased surgical time. The mean surgical time in SLO was 16.4% higher than in clipping. There was a significant difference in surgical time between SLO and clipping; however, no significant difference was identified between clipping and continuing the procedure without further measures. No postoperative complication related to staple line bleeding was identified.
Discussion:
In a scenario with limitations for the use of high-cost homeostatic agents, the stratified protocol to prevent bleeding in SG stapling line was able to significantly reduce surgical time without significant added risks.
Conclusion:
A stratified protocol to prevent bleeding in SG stapling line was able to significantly reduce surgical time.
Introduction
Bariatric surgery is the most cost-effective intervention in severe obesity.1–4 Among the surgical treatments for obesity, sleeve gastrectomy (SG) stands out, approved to treat obesity in 2007 and currently surpasses the Roux-en-Y gastric bypass in terms of the number of surgeries in the world. 5 Although systematic reviews have pointed out a significant decrease in complications associated with SG,6,7 there are still serious complications that should be carefully managed. Fistulas and postoperative bleeding are the most common complications. 8 Among the bleeding complications, up to 20% of cases have the staple line as a source of bleeding. This value can be even greater if cryptogenic hemorrhages are considered. 9
Bleeding through the staple line significantly increases costs due to the longer hospitalization and possible surgical new interventions. Analyses indicate an additional cost of, on average, $5261 per bleeding complication, ranging from 1879 to 49,350 dollars. 10
The main strategy to reduce the risk of postoperative bleeding in SG is prevention. The use of homeostatic materials in the staple line has been associated with a lower risk of bleeding and new intervention without a significant increase in surgical time. 11 However, this type of material entails costs of, on average, 580 euros per patient, 10 making it difficult to be used on a large scale in the health system.
Staple line oversewing (SLO) is the most used alternative due to its low cost and its effect of decreasing the incidence and severity of bleeding complications in SG. 12 However, this approach significantly increases surgical time 13 and is not risk free as it may be associated with a higher incidence of stenosis. 12 Wang et al. 14 reported no clear advantage of oversewing the staple line, becoming a controversial hemostatic strategy.
It is essential to develop protocols that allow the rational use of available resources to prevent bleeding in the staple line. This study presents the results of the use of a rational protocol to optimize the outcomes and prophylaxis of bleeding in staple line in SG. The objective was to identify whether its usage was sufficient to optimize the surgical time in patients whose screening for the risk of occult bleeding was negative.
Materials and Methods
The present study corresponds to a prospective analysis of patients undergoing SG using the stratified protocol of rational use of staple line bleeding prophylaxys.
Patients with an indication for SG were subjected to the procedure between July 2020 and March 2021 at a Santa Casa de Misericórdia de Porto Alegre hospital in Brazil. Patients subjected to the procedure under the criteria of the optimization protocol performed by a single team, to avoid potential learning curve bias, and that they completed the minimum postoperative follow-up period of 15 days were included. Patients with an ongoing anticoagulation therapy for up to 1 month before surgery and patients who needed SLO due to defect in the staple line formation or increased risk of fistula were excluded from the sample.
The population was evaluated for the presence of characteristics and comorbidities, namely, gender, body mass index, systemic arterial hypertension (SAH), type 2 diabetes mellitus, dyslipidemia, hepatic steatosis, and heart disease. The evaluated intraoperative variables included the following: surgical time (including time between skin incision and removal of the last trocar, including an SG and routine liver biopsy) and systolic blood pressure (SBP), as well as the need to clipping or SLO of bleeding points. The follow-up assesses the length of hospitalization and the presence of signs indicative of hemorrhagic complications, such as melena, blood transfusion, and need for surgical reintervention.
SG was performed under intravenous general anesthesia with minimization of opioid use. The patient was operated on in the French anti-Trendelenburg position. The standard technique used trocar placement was as follows: 11 mm inserted in the left supra-umbilical region of the midline, 12 or 15 mm in the right flank, 5 or 12 mm in the left hypochondrium, and 5 mm in the left flank. A French Fouchet 32 probe is inserted into the pylorus to guide the stapling. The procedure starts with the ligature of the gastric branches of the right and left gastroepiploic vessels and of the short gastric vessels.
The gastric section was performed with a 60 mm endoscopic stapler at 3 cm from the pylorus and maintained the esophageal-gastric transition. Specific stapling loads were used for each portion of the stomach. Signa Medtronic Endostapler loads were used, from the pylorus to the gastric fundus, two black loads (2.3 mm) and four purple loads (2.0 mm), or Echelon Powered using in sequence one black load (2.3 mm), one green load (2.0 mm), one gold (1.8 mm), and three blue (1.5 mm), all 60-mm long.
The protocol (Fig. 1) starts with a complete revision of the stapling line, looking for major signs of bleeding, namely, jet bleeding, diffuse and continuous bleeding, or continuous bleeding requiring aspiration. If any, the SLO was promptly performed with a 3–0 polydioxanone suture.
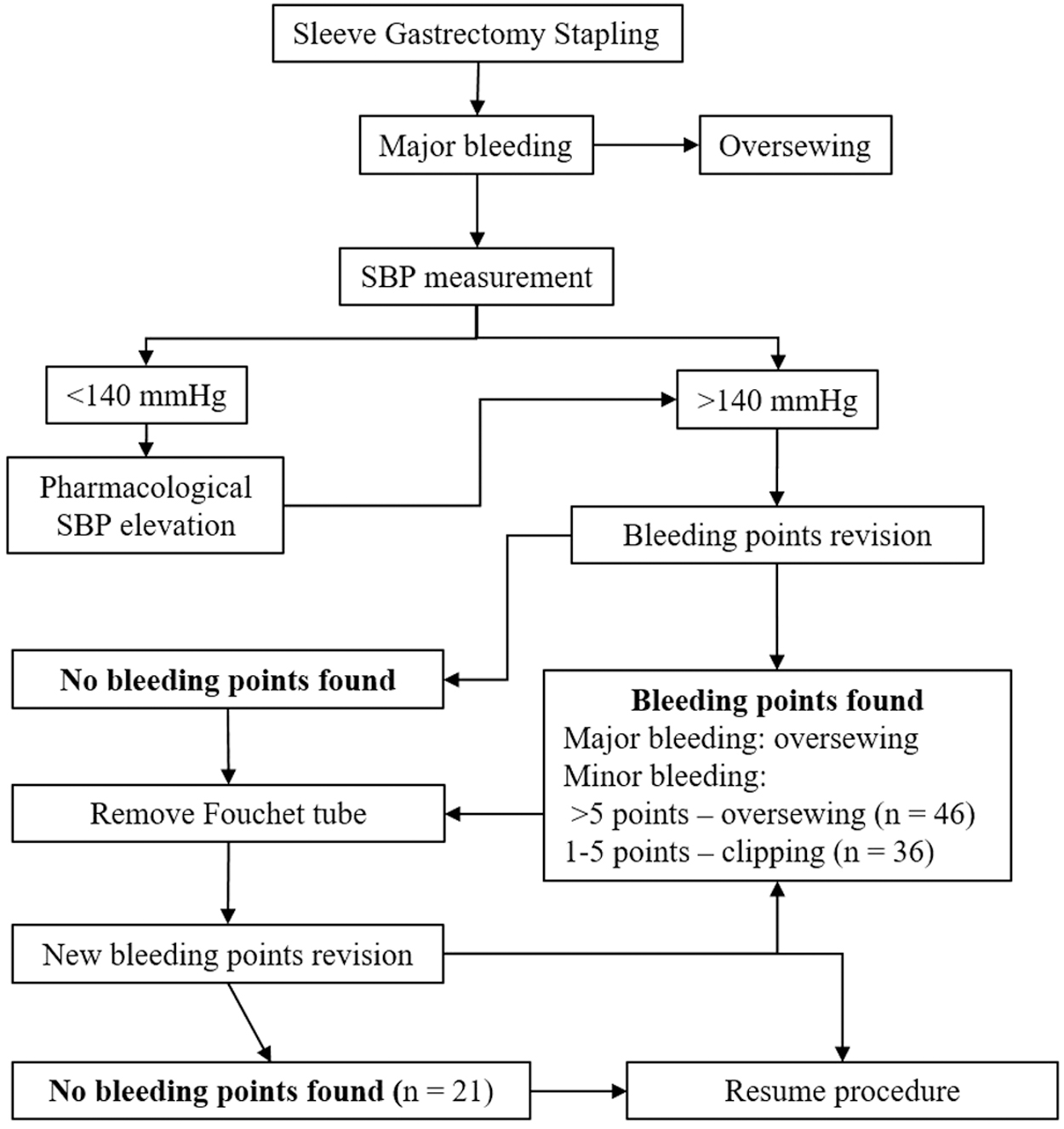
Bleeding protocol to define the procedures used in sleeve gastrectomy. SBP, systolic blood pressure.
The presence of minor bleeding is determined by the absence of the above criteria, which can be controlled with compression and the use of gauze and no need for continuous aspiration interruption. The SBP goal of 140 mmHg is then reached with slow and gradual administration of metaraminol 1 mg and/or ephedrine 10 mg. The SBP increase is done concurrently with the hemostasis checking. Under the SBP criteria, the staple line will be rechecked for bleeding point counting. In the case of more than five identified bleeding points, it is considered diffuse bleeding and the surgeon proceeds to oversew the staple line considering that clipping may not be sufficient to effectively control it diffusely.
In case of five or fewer bleeding points, they will be managed using number 400 titanium clips. If no bleeding points are found, the procedure can be completed (Fig. 2). The test was run before and after the removal of the Fouchet probe, due to the compressive effect that can be exerted on the bleeding points. A similar methodology, including the applied SBP goal, to evidence silent or hidden bleeding, was described by Sroka et al. 15 The aforementioned bleeding scores have been developed in 2014 by Siegel et al., 16 and have been used to coordinate the decision of intraoperative management.17,18 During this study, we did not consider spot cautery as a possible bleeding control measure, given the lack of evidence regarding its safety.
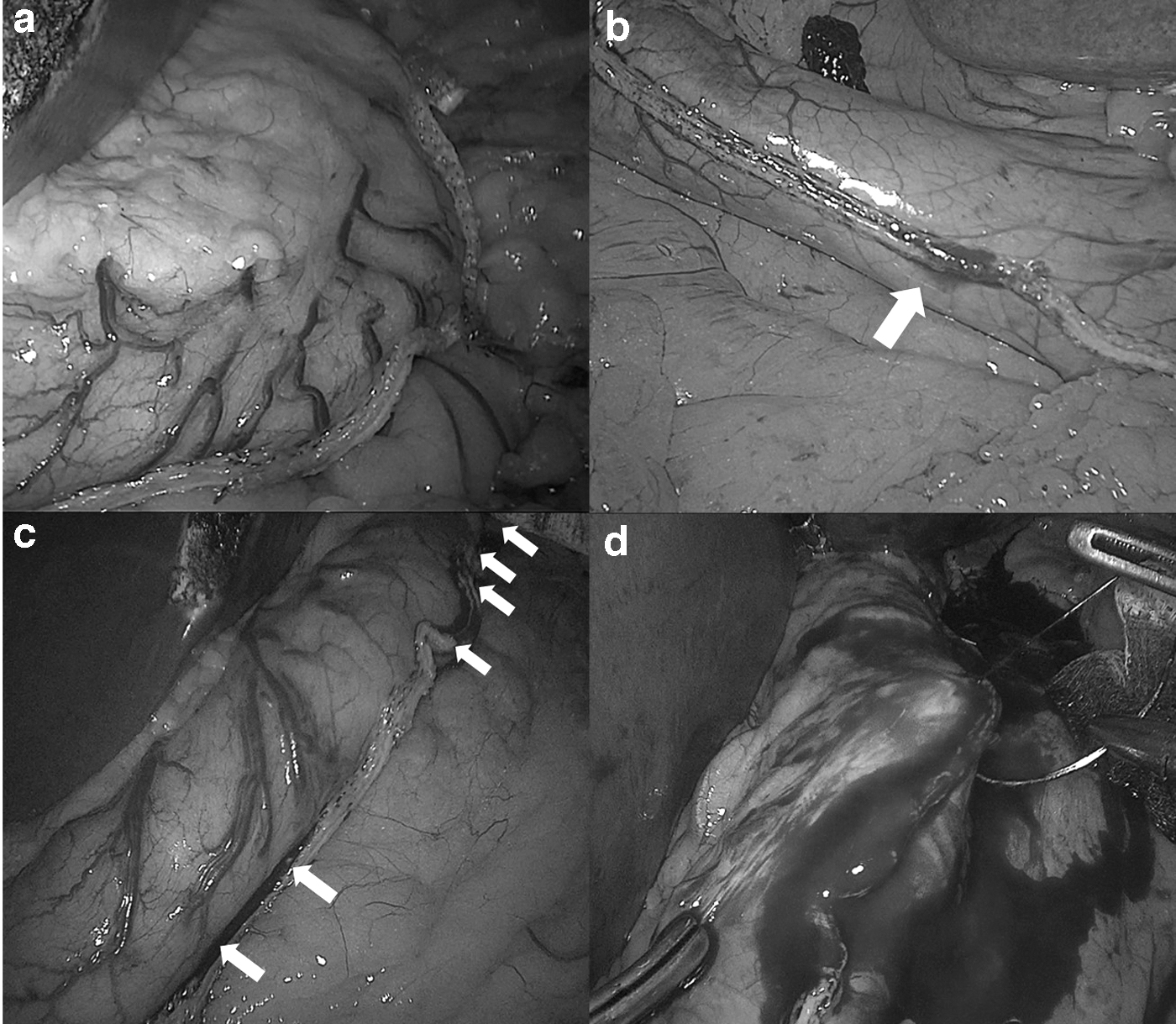
Bleeding test results in 140 mmHg SBP:
The patients were followed up for 15 days after the procedure to assess the length of hospitalization and the presence of signs indicative of hemorrhagic complications, such as melena, blood transfusion, and need for surgical reintervention. Considering that not all postoperative bleeding is due to staple line bleeding, and could eventually be due to omentum or short gastric vessels if there were any registry of bleeding complications, it would be investigated to find its origin. All surgeries selected in the study were performed by the same surgeon to avoid potential learning curve bias.
Sample calculation aiming to evaluate surgical time difference lead to 105 patients, estimating a confidence interval of 95% and a significance level of 5%, in a continuous outcome study of the mean surgical time of 74 minutes for the intervention group and 54 minutes for the group without prophylactic intervention, under the hypothesis of a standard deviation of 21 minutes. Considering this study as a hybrid model between the two approaches, the average between the two average surgical times is assumed as 64 minutes.15,16,19 Statistical analyses of results were used with Dunn's test for multiple comparisons, chi-square test for qualitative data, and t-test for quantitative data.
The study description was made from the STROBE Statement™ for observational studies, available at https://www.strobe-statement.org/. The study was approved by the institution's ethics and research committee under protocol number CAAE 44301021.0.0000.5335. The authors have no financial, academic, or personal conflicts of interest related to the study outcomes.
Results
One hundred five (105) patients subject to SG and meeting the study inclusion criteria were included. Two patients were excluded for using anticoagulation therapy with the impossibility to discontinue the treatment. There were no further sample losses in the analysis process, closing the screening with 103 participants concluding the follow-up process.
From the sample profile analysis, none significantly influenced the bleeding test result, except for gender, with women more likely to have a positive result (P < .05) (Table 1).
Factors Associated with the Bleeding Test Result in Patients Undergoing Sleeve Gastrectomy
The bold value signifies P = 0.47.
Application of the chi-square test for qualitative variables.
Application of the t-test for quantitative variables.
BMI, body mass index; DM2: type 2 diabetes mellitus; F, female; M, male; SAH, systolic arterial hypertension; SBP-BT, systolic blood pressure reached during the bleeding test.
The bleeding test was positive in 82 (79.6%) of the cases, with SLO being necessary for 56% thereof, 44.7% of the total (Table 2). The bleeding test result was significant (P < .001) for increased surgical time (Table 2). The mean surgical time in procedures with a positive test was 63.5 minutes, 19.8% longer than those with a negative test.
Impact of the Bleeding Test Result and the Prophylaxis Approach on the Surgical Time of Patients Undergoing Sleeve Gastrectomy
Application of Dunn's Test for multiple comparisons.
Medians followed by equal letters do not differ from each other.
SLO, staple line oversewing.
There was a significant difference in surgical time between SLO and clipping; however, no significant difference was identified between clipping and continuing the procedure without further measures of bleeding prophylaxis (Table 2).
Regardless of the intraoperative bleeding test result, there were no postoperative complications related to staple line bleeding. There were no reports of melena, blood transfusion, or surgical new intervention in the patient sample.
Furthermore, there were no significant differences between the length of hospitalization and the bleeding test result or the reinforcement procedure used (Table 1).
Discussion
This study showed that procedures to reinforce the staple line significantly impacted the surgical time, with the SLO being responsible for a longer surgical time. There were no significant differences in surgical time between clipping and no management at the stapling line. There were no complications of hemorrhagic origin, inferred by the absence of data related to melena, blood transfusion, and surgical new intervention, in the follow-up of patients receiving staple line reinforcement procedures based on the intraoperative bleeding test. Patients' characteristics such as age, SAH, diabetes, and previous cardiac pathology were considered risk factors to bleeding complications in SG. This study did not identify a correlation between the sample characteristics and the bleeding test result, except for the female with a greater tendency to a positive result in the bleeding test. We hypothesize that the difference is justified by the thinner gastric tissue in female patients. 20
The need to perform some intervention on the staple line seems to be increasingly evident in scientific studies. Postoperative bleeding is associated with increased morbidity and higher new intervention rates. 21 There is also an association between the incidence of fistulas and the need for blood transfusion after SG. 22
The clinical trial by Taha et al. 12 identified that SLO is a cost-effective method capable of significantly reducing the incidence and severity of postoperative bleeding. However, this method requires a significant increase in surgical time. According to the results of this study, it would be necessary to use SLO in 66.7 cases to prevent 1 case of severe bleeding.
Shah et al. showed that the use of a membrane coating made of biological tissue was able to guarantee a lower incidence of intraoperative bleeding and reduce surgical time regarding its control. The longest surgical time in the control group was attributed to the need for SLO or clipping in 67.3% versus 19.6% in the experimental group. In this analysis, 79.6% of patients needed intervention on the uncoated stapling line. This higher rate can be attributed to screening for occult bleeding performed with the protocol of the transoperative induced SBP increase.
The bleeding test used was based on the study by Sroka et al. 15 These authors performed a comparison between different approaches to prevent bleeding in the stapling line. De Angelis et al. 23 also associated the test with an improvement in bleeding outcomes after SG. This test has an interesting clinical translation because they tested the hypothesis that bleeding occurs in the postoperative period due to increased blood pressure, secondary to complete anesthetic recovery and pain.
In this study, we analyzed an intervention proposal after using the bleeding test stratified according to the magnitude of the identified bleeding. This scale was built based on previous studies by Siegel et al. and Redmann et al.16,17 Both authors developed bleeding scores with a progressive classification of severity. Redmann et al. compared different technologies to build the stapling line in SG.
In a previous study by Jossart, age, SAH, diabetes, and previous cardiac pathology were considered significant for the increase in bleeding complications in SG. 24 This study did not identify a correlation between the sample characteristics and the bleeding test result, except for the female with a greater tendency to a positive result in the bleeding test. It is hypothesized that the difference is justified by the thinner gastric tissue in female patients. 25
An analysis limitation refers to the absence of a control group in the study design, in which no bleeding prophylaxis would be taken. However, not performing any kind of intervention without an SBP goal may put the patient at a high risk of complications in the postoperative period. We encourage new studies to compare the individual management and stratified treatment of staple line proposed in this study, with compulsory SLO. We highlight that the study aims primarily to report the operation room time difference between bleeding prophylaxis and claims the necessity of further studies to properly evaluate the rare risk of bleeding.
Suspects of occult bleeding were not measured in this study. Although secondary outcomes of need for transfusion or symptoms of gastrointestinal bleeding were not reported in our sample in the first 15 days after surgery, analyses of hemoglobin levels and nonuse of a drain did not allow the quantification of a low amount of bleeding. Our study did not consider the applicability of endoscopy as a form of intraluminal bleeding measure and as a part of the intervention decision process due to the increase in cost and surgical time of the process. Although our study aims to build a rationale for postoperative staple line bleeding prophylaxis based on extraluminal bleeding quantification, we encourage new studies approaching intraluminal bleeding using intraoperative endoscopy as a more accurate risk stratification of postoperative complications.
It is noteworthy that the results presented were related to surgeries performed during the COVID-19 pandemic. In this period, the importance of result optimization protocols became even more evident. Our study questions the compulsory staple line reinforcement since it may not be worth the considerable increased operative time spent on a procedure with controversial results. A faster surgery without losing the opportunity to deliver the available resources to prevent complications can have repercussions in a postoperative period of early recovery and with less demand for the use of emergency resources.
Conclusion
In a scenario with limitations for the use of high-cost homeostatic agents, it can be concluded that a stratified protocol to prevent bleeding in SG stapling line was able to significantly reduce surgical time in 55.3% of patients operated with a scientifically proven screening intervention.
Footnotes
Authors' Contributions
A.V.B.: conceptualization (lead), investigation, methodology, project administration, and writing original draft and review; J.I.: data curation, formal analysis (lead), methodology, visualization, and writing original draft and review; J.N.C.d.L.: data curation (lead) and formal analysis; M.C.M.: data curation and writing review; E.R.B.: data curation and formal analysis; J.V.M.G.: supervision, validation, visualization, and writing review; M.K.F.: data curation and writing review; I.V.d.S.: supervision and writing review.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.