
Abstract
Background:
The aim of this study is to assess the extent of the increased intracranial pressure resulting from lateral decubitus and 45° downward positioning using sonographic optic nerve sheath diameter (ONSD) in patients undergoing laparoscopic transperitoneal nephrectomy. In addition, we evaluated the effect of the carbon dioxide pneumoperitoneum (CO2PP) on ONSD.
Materials and Methods:
Twenty-four adults were enrolled in this prospective observational study. Longitudinal and transverse ONSDs were measured for each eye by ocular ultrasonography. The values were noted in supine position (T0), 20 minutes after induction of anesthesia (T1), after insufflation of the abdomen in lateral 45° head-down position (T2), at 30-minute intervals during surgery (T3-T4-T5), during lateral 45° head-down position after CO2 exsufflation (T6), before awakening while supine (T7), and at postoperative 24th hour (T8). Hemodynamic and respiratory parameters were investigated at the measurement time points.
Results:
Average ONSD values for the lower eye was T0 = 4.27 ± 0.4 mm, T1 = 4.56 ± 0.6 mm, T2 = 4.84 ± 0.6 mm, T3 = 4.91 ± 0.4 mm, T4 = 4.99 ± 0.5 mm, T5 = 4.97 ± 0.5 mm T6 = 4.96 ± 0.5 mm, T7 = 4.76 ± 0.4 mm, T8 = 4.36 ± 0.5 mm and for the upper eye was T0 = 4.24 ± 0.4 mm, T1 = 4.39 ± 0.5 mm, T2 = 4.54 ± 0.5 mm, T3 = 4.60 ± 0.4 mm, T4 = 4.66 ± 0.4 mm, T5 = 4.72 ± 0.7 mm, T6 = 4.68 ± 0.4 mm, T7 = 4.52 ± 0.4 mm, T8 = 4.30 ± 0.4 mm (P < .001).
Conclusion:
In our study, we observed a significant increase in ONSD within minutes after the patient was placed in a head-down position. We also observed that the difference increased more with CO2PP and was proportional to the length of the surgery. We found that it regressed to initial levels at the postoperative 24th hour.
Clinicaltrials.gov:
NCT05185908.
Introduction
Laparoscopic surgery is the primary surgical approach for the treatment of many surgical disorders, including urological operations. Laparoscopic transperitoneal nephrectomy (LTPN) has emerged as a standard of care for renal cell tumors that are confined to the kidney. 1 In the contemporary world, the laparoscopic technique is performed by placing three to five ports through the peritoneum and carbon dioxide (CO2) is the most commonly used gas for insufflation because it is colorless, inexpensive, nonflammable, and has higher blood solubility than air, which reduces the risk of gas embolism due to its high diffusion rate. 2 The combined effect of a prolonged 45° head-down position and carbon dioxide pneumoperitoneum (CO2PP) has been reported to increase the risk of significant negative physiological effects.
Increased intracranial pressure (ICP) and decreased cerebral perfusion pressure (CPP) represent well-known fearful complications in many types of acute brain injuries. 3 Clinically it can lead to brain injury, seizure, coma, stroke, or death. The application of monitoring methods for the early detection of treatable ischemic complications and the introduction of protocols to prevent secondary insults to the brain have been reported to improve the outcome in these patients. 4 Even though invasive ICP monitoring provides the most accurate information on ICP, it costs a craniotomy. 5 In practice, a noninvasive diagnosis of raised ICP is preferably performed by ophthalmoscopy or transcranial Doppler sonography.6,7
Recent studies have shown that measuring optic nerve sheath diameter (ONSD) is gaining popularity as a noninvasive and effective method that can detect increases in ICP. Whenever ICP raises, subarachnoid compartment of the nerve is also affected, the optic nerve sheath is stretched resulting in an enlargement of the ONSD. Scientific literature describes a linear relationship between ONSD and ICP.5,8–14 There are many studies in recent years that investigated the relationship between ONSD and postoperative morbidity in several surgical procedures, including laparoscopy.15,16
This study aimed to investigate the influence of CO2PP and lateral 45° head-down positioning on ONSD in patients undergoing LTPN. In addition, hemodynamic and respiratory parameters were screened in the first 24 hours. Perioperative and postoperative complications were also recorded.
Materials and Methods
Study design and study subjects
In this prospective observational study, 24 patients undergoing LTPN were enrolled between December 2016 and February 2017. This study is performed according to the principles of good clinical practice and the International Declaration of Helsinki. The study was approved by the local ethics committee (dossier no. 2016/1283). The study is registered on Clinicaltrials.gov and reported according to the CONSORT statement.
Before enrolment, written informed consent was obtained from all participants. Twenty-four adult patients who were American Society of Anesthesiologists (ASA) class I to III, aged between 18 and 75 years, and scheduled for an elective LTPN were enrolled in this study. The main exclusion criteria were patients with pre-existing ophthalmic or neurological disease (diabetic retinopathy, glaucoma, and retinal detachment), history of eye surgery, history of neurosurgery, age >75 years, body mass index (BMI) >40, and ASA physical status >III.
Anesthesia protocol
Patients were monitored with pulse oximetry, noninvasive blood pressure, end-tidal carbon dioxide (ETCO2), temperature, electrocardiogram, and bispectral index (BIS). General anesthesia was induced using a bolus intravenous injection of 2 mg/kg propofol and 2 μg/kg fentanyl followed by 0.6 mg/kg rocuronium. After tracheal intubation, patients were mechanically ventilated with a tidal volume of 6–8 mL/kg of ideal body weight at a respiratory rate of 10–16 breaths/min to maintain ETCO2 partial pressure between 35 and 40 mm Hg. Positive end-expiratory pressure of 4 cm water was applied to prevent decreases in functional residual capacity in those with normal lungs and the inspiratory-to-expiratory time ratio was set at 1:2. Anesthesia was maintained with 2% sevoflurane plus a continuous infusion of 0.02 μg/kg remifentanil with 40% oxygen using medical air. Radial artery cannulation was performed for continuous monitoring of arterial blood pressure and analysis of arterial blood gas.
Surgical technique
A transperitoneal approach was performed in all patients. Patients were placed in a 45° head-down (flank) position. A Veress needle was used to enable pneumoperitoneum. A 10-mm trocar was placed lateral to the umbilicus, and a camera was introduced into the abdominal cavity. In right-sided cases, a 12-mm second port was placed at the midclavicular line 2 cm below the costal margin, whereas the 5-mm third port was inserted between the anterosuperior iliac spine and the umbilicus. In left-sided cases, a 12-mm port was placed between the anterosuperior iliac spine and the umbilicus, whereas a 5-mm port was placed at the midclavicular line 2 cm below the costal margin.
Dissection started with the incision of the Toldt line and followed by the reflection of the ascending or descending colon medially, according to operation side. After retroperitoneal space was entered, the ureter was identified and dissected, and the hilar vessels were observed. After the application of Hem-o-lok® clips on each artery and vein, the vessels were transected and ligated. The specimen was released from the surrounding adhesions and was removed. All operations were performed or supervised by a single attending surgeon (S.E.). Insufflation pressure was limited to 12–15 mm Hg during the surgery.
Sonography technique
The measurements were performed by 2 experienced anesthesiologists (A.G.A. and M.S.K.) with an ultrasound machine with a 7–10 MHz high-frequency linear probe (GE Healthcare, Wauwatosa, WI). The probe was oriented perpendicularly in the vertical plane and at around 30° in the horizontal plane on the closed eyelids of both eyes of individuals in supine position. Ultrasound gel was applied on the surface of each eyelid and the measurements were made in the transverse and sagittal planes of the widest diameter visible 3 mm behind the retina in both eyes.
The final ONSD value was calculated by averaging three measured values. ONSD measurements were noted at each time point; T0: supine position, T1: 20 minutes after induction of anesthesia, T2: after insufflation of the abdomen in lateral 45° head-down position, T3-T4-T5: at 30-minute intervals during surgery, T6: during lateral 45° head-down position after CO2 exsufflation, T7: before awakening while supine, T8: at postoperative 24th hour. Hemodynamic and respiratory parameters were also recorded at the measurement time points.
Primary outcome
The primary outcome of this observational study was to investigate the influence of CO2PP in combination with lateral 45° head-down positioning on ONSD in patients undergoing LTPN.
Secondary outcomes
The secondary outcomes included mean arterial pressure (MAP), heart rate, ETCO2, BIS, length of hospital stay, and the incidence of side effects, including nausea, vomiting, hypotension, and complications (e.g., neurological disorders and vascular injury). Postoperative early-stage agitation was screened by the Richmond Agitation Sedation Scale (RASS). The RASS is a commonly used sedation scale by the use of a 10-point, with scores ranging from +4 (a violent dangerous patient) to −5 (an unarousable patient). A sedation score of 0 is most often therapeutically targeted, as it correlates with an alert and calm patient. In addition, all patients were screened for signs of delirium with the 3-minute Diagnostic Confusion Assessment Method (3D-CAM). The 3D-CAM is a validated appropriate method for assessment of delirium in the postanesthesia care unit or intensive care unit.17,18
Statistical analysis
Sample size calculation was performed based on a previous study 19 comparing the differences in ONSD. A minimum of 19 patients were required for a standard deviation of 0.5 mm between T0 and the T4 time points (90% power and P < .05). Taking into account a possible loss of patients of 30% during the follow-up period, the final sample size is adjusted to 24 patients. Data analysis was performed using SPSS 22 software (IBM Corp., Armonk, NY). The mean and standard deviation values of the categorical data were calculated. The percentage of nominal values is extracted. Parametric data were assessed by repeated measure ANOVA. Baseline characteristics are presented as mean ± standard deviation or median (minimum–maximum) for quantitative variables, and as number (percentage) for qualitative variables. A P value of .05 was considered significant in outcome analysis.
Results
Study flow, baseline characteristics, and procedural characteristics
Twenty-three patients were able to complete the study between December 2016 and February 2017. One patient was excluded due to unplanned conversion of open surgery. There were 11 men and 12 women, with a mean age of 39.8 ± 13 years and a BMI of 27 ± 3.3. Demographic and intraoperative records are listed in Table 1.
Patient Demographics and Intraoperative Data
Values are presented as mean ± standard deviation.
BMI, body mass index.
The primary outcome measure is shown in Figure 1. Average ONSD values for the lower eye was T0 = 4.27 ± 0.4 mm, T1 = 4.56 ± 0.6 mm, T2 = 4.84 ± 0.6 mm, T3 = 4.91 ± 0.4 mm, T4 = 4.99 ± 0.5 mm, T5 = 4.97 ± 0.5 mm T6 = 4.96 ± 0.5 mm, T7 = 4.76 ± 0.4 mm, T8 = 4.36 ± 0.5 mm and for the upper eye was T0 = 4.24 ± 0.4 mm, T1 = 4.39 ± 0.5 mm, T2 = 4.54 ± 0.5 mm, T3 = 4.60 ± 0.4 mm, T4 = 4.66 ± 0.4 mm, T5 = 4.72 ± 0.7 mm, T6 = 4.68 ± 0.4 mm, T7 = 4.52 ± 0.4 mm, T8 = 4.30 ± 0.4 mm (P < .001). ONSD values in both eyes were found significantly higher than the initial values, except for T8 (P < .001).
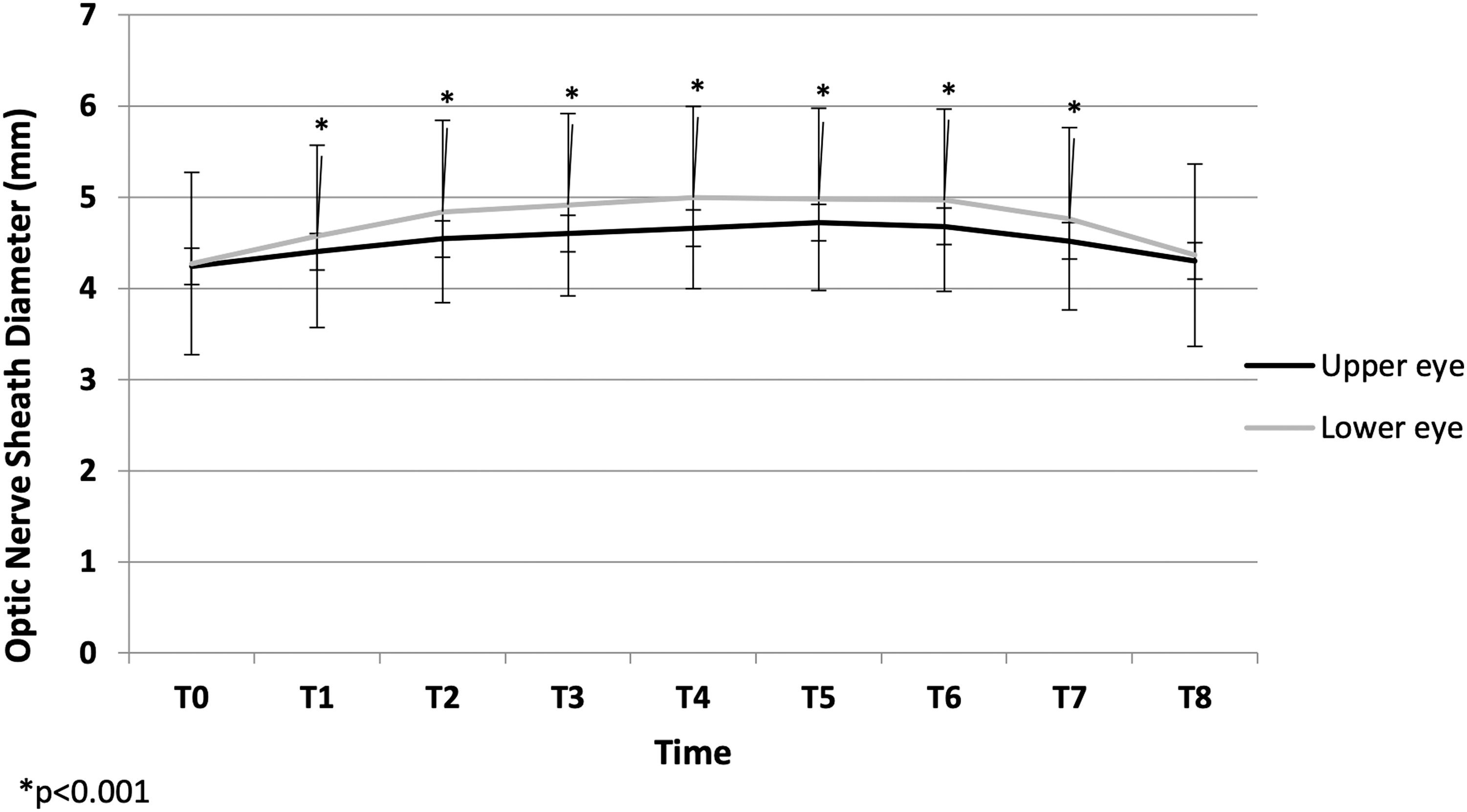
Optic nerve sheath diameter.
The secondary outcome measures are shown in Figure 2. Hemodynamic and respiratory data were not significantly different compared with the initial values (P > .05). RASS scores were observed <1 in the study population. Delirium was not diagnosed in any patient.

Hemodynamic parameters: Mean arterial pressure
Discussion
In this study, we observed a significant increase in ONSD, measured by optic sonography, in both eyes after the patient was placed in the lateral 45° head-down position. We also found that the difference in ONSD increased extra with the effect of CO2PP and was proportional to the duration of the surgery. The values were regressed to initial levels at the postoperative 24th hour.
A steep head-down position may have significant negative physiological effects when maintained for long period. Main ocular adverse events are represented by corneal abrasions, increased IOP, and perioperative visual loss (POVL), including anterior and posterior ischemic optic neuropathy. Hypertension produced by prolonged head-down position has been attributed to serious ocular consequences, such as retinal detachment. 20 Further cases have been reported up to an irreversible bilateral visual loss, by ischemic optic neuropathy caused by reduced ocular blood flow, central retinal artery occlusion, and cortical infarction.21–24
Many studies investigated the relationship between positioning and ocular complications. In the United States, POVL incidence is estimated to 8.46/10,000 after cardiac surgery, 3.09/10,000 after spinal fusion, and 1.24/10,000 after colorectal resection. 25 When we narrow our research on laparoscopic surgeries, we found that the frequency of ocular complications increases in the literature. 15 Further cases have been reported after laparoscopic procedures of prostatectomy, nephrectomy, herniotomy, and colorectal resection.21,23,24,26–28 Several studies have investigated the measurements of optic nerve diameter in robot-assisted prostatic surgery; however, no other study investigated ONSD in laparoscopic nephrectomies in the literature. Surprisingly, one study investigated the extent of the raised ICP in pediatrics by ultrasonographical measuring ONSD undergoing laparoscopic surgery. 29
The respiratory changes of this positioning mainly include cephalic displacement of the diaphragm, decreased lung volume, lung compliance, functional residual capacity, and increased peak airway pressure, leading to postoperative pulmonary complications. It allows for a gravity-induced reduction in shunt flow to the lungs and may have higher rates of intraoperative desaturations.30,31 The prevalence of pulmonary complications in steep Trendelenburg position and abdominal insufflation of CO2 has been shown ∼30% and is associated with increased mortality and morbidity rates. 32 Falabella et al showed that the steep Trendelenburg position and pneumoperitoneum significantly increased MAP and systemic vascular resistance and decreased aortic diameter. 33 Accordingly, in our study, we did not encounter any pulmonary and/or cardiac complications.
Cerebral autoregulation plays a significant role in maintaining constant blood flow and avoiding changes in CPP. 34 Trendelenburg position and CO2PP increase venous congestion and cause significant changes in cerebral hemodynamic physiology and increase ICP. Cerebral autoregulation impairment may result in undesirable postoperative neurological events. Hence, ONSD measurement can be a reliable landmark to monitor possible ICP increases in a head-down position. An observational study by Chen et al investigated internal jugular vein incompetency (IJVVI) in elderly patients that shows IJVVI after adequate positioning may develop elevated ICP as well as mildly compromised postoperative cognitive function in the short term. 35 Our patients were middle-aged adults, and we did not encounter any neurological dysfunction during early recovery.
Possible measures that can be applied to prevent ocular complications are reducing operating times as much as possible. Second, in the Trendelenburg position, pursue the minimal tilt to provide an adequate operating field. Steep tilt should be avoided as much as possible. Third, a vigilant anesthesiologist should be aware of specific patient conditions that may preclude certain positions, anticipate any physiological insult that may result, and ensure adequate access to treat these damages.
Our study had some limitations. First of all, despite the observational nature of our study, there might be unrecognized bias concerning the new developments in the area, for example, the values of cerebral tissue oxygen saturation (rSO2) were not monitored through cerebral oximeter, which would be recommended to investigate the possible relation between rSO2 and 45° downward position and CO2PP. Second, we assess the early postoperative period through RASS and 3D-CAM scores. Thus, additional studies should examine longer-term basis for delirium screening. Finally, our data must be validated with future multicenter research.
Conclusion
In conclusion, steep head-down positioning in laparoscopic surgery remains a clinical challenge. This observational study demonstrated a significant increase in ONSD within minutes after the patient was placed in a lateral decubitus position. We also observed that the difference increased more with CO2PP and was proportional to the length of the surgery. Clinical outcomes reported here provide consistent data to support the evidence of ONSD regression to initial levels at the postoperative 24th hour. Further quantitative studies evaluating these variables for laparoscopic procedures are needed.
Footnotes
Authors' Contributions
Conceptualization and writing—reviewing and editing by A.G.A; data curation and investigation by E.A.S.; software and methodology by H.Ş.Ç.; writing—original draft preparation by E.S.B.; visualization and investigation by N.S.; visualization and software by S.E.; investigation and supervision by M.S.K.
Acknowledgments
The authors thank postoperative care unit and colleagues, for their help in recording data and following patients.
Disclosure Statement
The authors have no conflicts of interest in this study.
Funding Information
No funding has been received for this study.