
Abstract
Background:
The transoral endoscopic thyroidectomy by vestibular approach (TOETVA) has been developed for papillary thyroid carcinoma (PTC) treatment with satisfactory results. However, there were few malignant thyroid nodules ≥2 cm in previous studies of TOETVA. Therefore, we conducted this study to evaluate the results of treatment by TOETVA for PTC with tumor size ≥2 cm.
Materials and Methods:
The clinical characteristics and surgical outcomes of 10 PTC patients with tumor size ≥2 cm who underwent TOETVA in our center from June 2018 to August 2021 were, respectively, reviewed.
Results:
All 10 included PTC patients successfully underwent TOETVA and the mean tumor size was 2.5 ± 0.5 cm. The mean number lymph nodes dissected was 9.6 ± 2.9, and 3.1 ± 3.3 positive lymph nodes were discovered. Postoperatively, transient hypoparathyroidism was recorded in 2 patients (20%), transient recurrent laryngeal nerve injury was noted in 1 patient (10%), transient superior laryngeal nerve injury was noted in 1 patient (10%), and numb chin was identified in 1 patient (10%). The postoperative complications aforementioned recovered within 6 months. During a median follow-up of 23.8 ± 13.1 months, no other complications or tumor recurrence were found.
Conclusions:
TOETVA is feasible for PTC patients with tumor size ≥2 cm and satisfactory short-term surgical outcomes have achieved in this study. We suggested that experienced surgeons can gradually expand the indications for TOETVA.
Introduction
Thyroid carcinoma ranks fifth in malignancies among women and mostly occurs in the young. Therefore, aesthetic satisfaction has gradually become an important treatment require. To avoid a conspicuous neck scar caused by open surgery, endoscopic thyroidectomy was developed and gradually popularized. Many different approaches have been described to perform thyroidectomy, and the transoral endoscopic thyroidectomy vestibular approach (TOETVA) is the only procedure absolutely free of cutaneous scar. Nowadays, TOETVA has been widely used in the treatment of papillary thyroid carcinoma (PTC), and satisfactory surgical outcomes have been confirmed in many centers.1–3 Previous studies suggested that the safety and feasibility of TOETVA for the treatment of PTC are comparable with open surgery.4,5
However, due to the narrow operation space and technical difficulty, TOETVA was only used in the treatment of thyroid microcarcinoma in some centers,6,7 and some researchers set malignant nodules <2 cm as the inclusion criteria for TOETVA. Therefore, TOETVA for malignant nodules ≥2 cm is rarely reported, and the therapeutic effect of TOETVA on PTC patients with tumor size ≥2 cm remains unclear.
In this study, we retrospectively analyzed the clinical characteristics and surgical outcomes of 10 PTC patients with tumor size ≥2 cm. The main purpose was to evaluate the feasibility of expanding the application of TOETVA.
Materials and Methods
Patients and inclusion criteria
Clinical data of PTC patients with tumor size ≥2 cm who underwent TOETVA at the Guangdong Provincial Hospital of Traditional Chinese Medicine between June 2018 and August 2021 were retrospectively analyzed. The study protocol was approved by the Institutional Review Board for ethics at the Guangdong Provincial Hospital of Traditional Chinese Medicine. The inclusion criteria were (1) confirmed cases of PTC with tumor size ≥2 cm based on final histopathology and (2) patients who underwent TOETVA. Besides, TOETVA is not recommended for patients with any of the following conditions: (1) evidence of distant metastasis or level I–V metastatic lymph nodes; (2) patients with T4; (3) patients with a prior history of surgery or radiotherapy on the neck; and (4) patient could not tolerate anesthesia or surgery. All 10 patients were qualified for the study selection criteria.
Perioperative preparation
Preoperative neck ultrasound was recommended routinely for evaluation of tumor and lymph node status. Lobectomy and isthmectomy is the recommended initial surgical approach for cT2 PTC patients. Total thyroidectomy may be preferred in cT3 patients or in patients with bilateral malignant nodules. Intravenous antibiotic was administered 30 minutes before surgery.
Surgical technique
Patients were placed in supine position with their neck extended. Electromyography tube was used for endotracheal intubation. After disinfecting the oral cavity, a 10-mm incision port was made in the middle of the vestibule and above the inferior labial frenulum. An adrenaline–saline solution (1:500,000) was injected from the vestibule to the anterior of the neck at the subplatysmal layer. Then, two 5-mm bilateral incisions were made on the mucosa at the level of the first premolars. A 10-mm and two 5-mm trocars were inserted through the middle and lateral incisions, respectively. Owing to the limited working space, a hybrid method combining carbon dioxide (CO2) insufflation with surgical sutures was applied (Fig. 1). The CO2 was insufflated at a pressure of 6 mm Hg with high flow. A 30° angled camera was then advanced through the middle trocar.

A hybrid method combining CO2 insufflation with surgical sutures. CO2, carbon dioxide.
Then a working space was created by electric hook and ultrasonic scalpel to the larynx superiorly, to the sternal notch inferiorly and to both middle edges of the sternocleidomastoid laterally. After the establishment of the initial working space, the linea alba cervicalis was divided and the strap muscles were retracted by a U-shaped retractor (Fig. 2), and the thyroid was revealed. Then the isthmus was separated from the surface of the trachea and transected, and the thyroid was retracted medially and the carotid artery was exposed on the outside. To better expose the superior pole of the gland and protect the external branch of the superior laryngeal nerve (SLN), part of the sternothyroid was routinely transected (Fig. 3). The upper pole of the gland was lifted up and superior thyroidal vessels was ligated. Then adjacent soft tissues were dissected to preserve the superior parathyroid gland, and the recurrent laryngeal nerve (RLN) was confirmed near the larynx entry point.
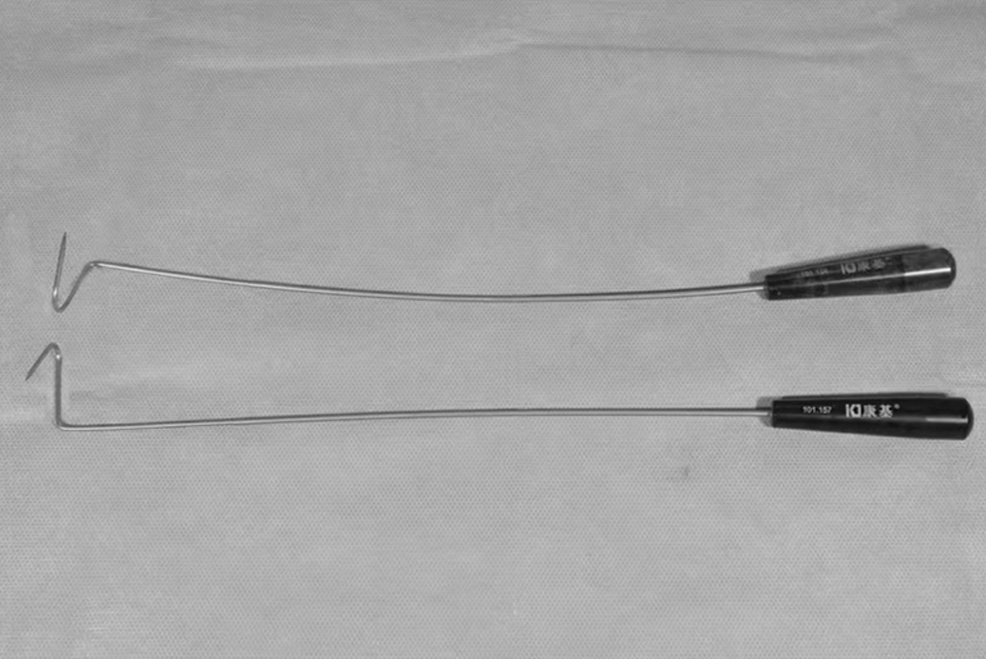
U-shaped retractors used during operation.
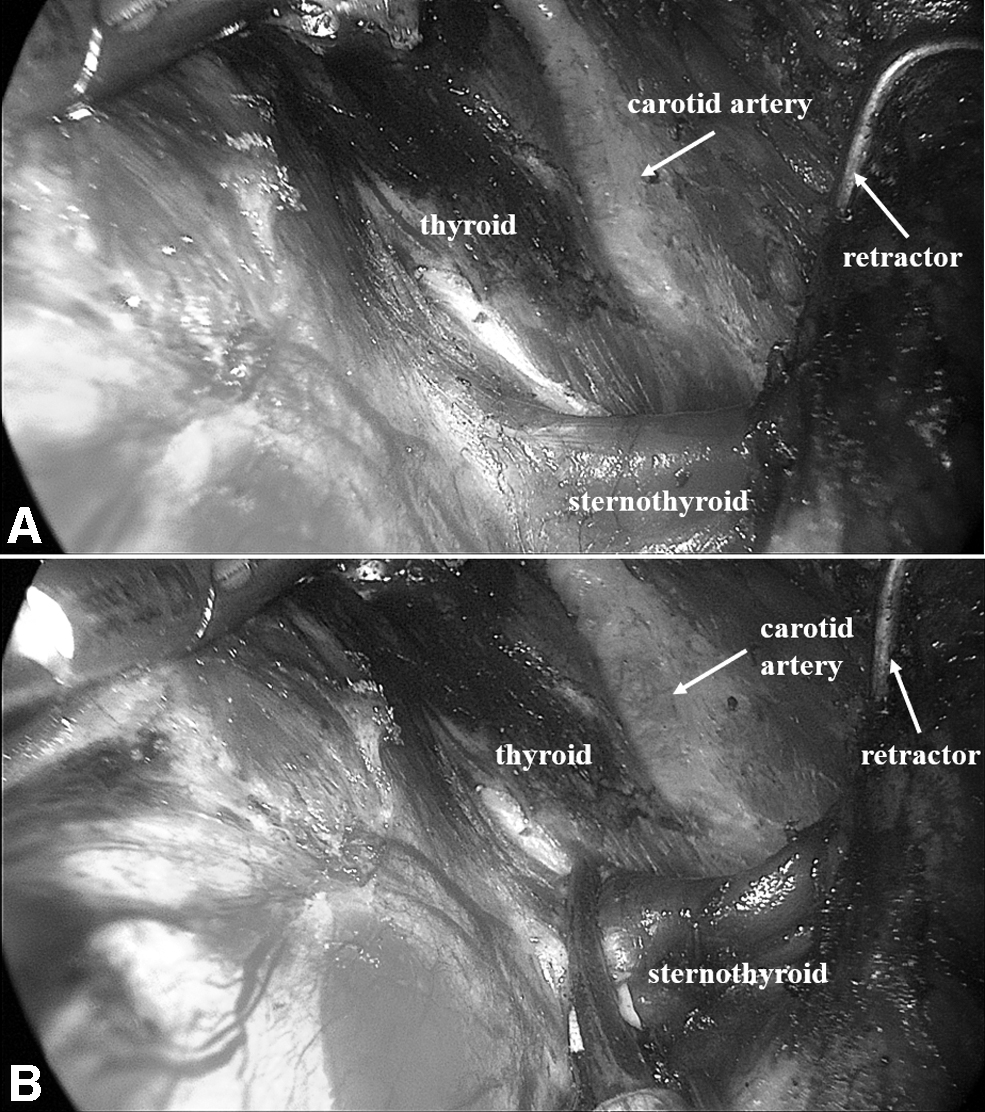
Exposure of the superior pole of the thyroid;
The use of a nerve monitoring system was highly recommended and used in all included cases. Subsequently, the thyroid was cut close to the thyroid capsule to protect the RLN and inferior parathyroid gland. Then the rest of Berry's ligament was dissected, the inferior thyroid vessel was ligated and the thyroid lobe was removed completely. If necessary, the contralateral thyroid lobe was removed in the same way as earlier. The ipsilateral central neck dissection (CND) was performed routinely. Central compartment was identified by brachiocephalic trunk artery inferiorly, carotid artery laterally, and deep layer of deep cervical fascia posteriorly. Pay attention to dissect and protect the RLN until it descends into the chest. Afterward, both the thyroid and central lymph nodes were taken out from the observation hole in a specimen bag. Then the operative field was rinsed with distilled water and a drainage tube was placed beside the trachea. At last, both the linea alba cervicalis and incisions of mouth were closed using absorbable sutures.
Postoperative management
Patients received a normal diet 6 hours after surgery. Prophylactic antibiotics were used once within 24 hours postoperatively. The gauze was pressed by elastic bandage and placed around the chin for 48 hours. If the 24-hour drainage volume was <30 mL, the drainage tube was removed. Postoperative follow-up visits were scheduled at 1, 3, 6 months, and then annually thereafter. Hoarseness, cough, vocal cord function, parathyroid hormone level, numb chin, other complications, and tumor recurrence were monitored during follow-up.
Results
Patients' characteristics
All 10 patients underwent TOETVA successfully and no cases required conversion to open surgery. Of the 10 patients, 9 were female and 1 was male. The mean patient age was 34.2 ± 11.0 years, and the mean body mass index was 21.7 ± 3.9 kg/m2. Total thyroidectomy was performed in 2 patients and lobectomy was performed in the other 8 patients. The mean operative times for lobectomy and total thyroidectomy were 142.4 ± 53.4 and 160.0 ± 14.1 minutes, respectively. The size of the tumor was 2.5 ± 0.5 cm with 9.6 ± 2.9 retrieved lymph nodes and 3.1 ± 3.3 positive lymph nodes. The mean length of postoperative hospital stay was 3.4 ± 1.3 days with a range of 2–6 days (Table 1).
Clinical Characteristics and Surgical Outcomes of the Papillary Thyroid Carcinoma Patients with Tumor Size ≥2 cm Who Underwent Transoral Endoscopic Thyroidectomy by Vestibular Approach
BMI, body mass index; CND, central neck dissection.
Complications of TOETVA
The postoperative complications of TOETVA are presented in Table 2. Transient RLN and SLN were found in 1 patient each, whereas transient hypoparathyroidism in 2 patients. The aforementioned complications spontaneously resolved within 6 months and no case developed permanent RLN injury, permanent SLN injury, or permanent hypoparathyroidism. Besides, numb chin occurred in 1 patient and recovered in 3 months. None of the patients had surgical infection, tracheal injury, chyle fistula, vagus nerve injury, or Horner syndrome. The mean follow-up period for the patients was 23.8 ± 13.1 months. During the follow-up period, no other complications and tumor recurrence were found.
Postoperative Complications of the Papillary Thyroid Carcinoma Patients with Tumor Size ≥2 cm Who Underwent Transoral Endoscopic Thyroidectomy by Vestibular Approach
Including tracheal injury, chyle fistula, vagus nerve injury, and Horner syndrome.
RLN, recurrent laryngeal nerve; SLN, superior laryngeal nerve.
Discussion
TOETVA was first used in clinical practice in 2009. 8 Compared with other remote approaches for endoscopic thyroidectomy, TOETVA has less trauma and better cosmetic results.7,9 Therefore, TOETVA has been widely concerned and developed rapidly. TOETVA was primarily done for benign thyroid disease in the first few years and only 26 patients diagnosed with malignant lesions in the largest cohort included 422 patients by Anuwong. 10 With the progress of surgical techniques, TOETVA has been routinely used in the treatment of PTC. However, the maximum tumor size for TOETVA remains debatable. In some studies, only papillary thyroid microcarcinoma was selected for TOETVA.6,11,12
Some other surgeons consider a tumor size <2 cm as an indication for TOETVA,3,13,14 and in the consensus of Chinese experts in 2018, TOETVA was recommended for PTC patients with tumor size <2 cm. However, the Chinese consensus also suggested that experienced surgeons can appropriately expand the application of TOETVA. Several reports on TOETVA include a few PTC patients with tumor size ≥2 cm, but do not separately record the complications for these patients.15–18 Therefore, the feasibility of TOETVA for the treatment of PTC patients with tumor size ≥2 cm needs to be confirmed. To our knowledge, this is the first cohort of study of TOETVA specifically aimed at the treatment of PTC patients with tumor size ≥2 cm.
The number of dissected/positive lymph nodes and operative time were used to evaluate the feasibility in this study. CND in TOETVA can be performed without the obstacle of the sternum and clavicle. Therefore, TOETVA is superior to chest approach in the process of CND. Previous studies reported that the number of dissected lymph nodes in CND by TOETVA was comparable with that of open surgery.4,5,19,20 The mean number of dissected lymph nodes in this study was 9.6 ± 2.9, which was higher than that in Ahn's study (3.67 ± 3.05), 4 Wang's study (8.24 ± 4.88), 5 Liu's study (9), 19 and Sun's study (7.00 ± 4.08). 20 The rate of lymph-node metastasis was 60.0% and the mean number of positive lymph nodes was 3.1 ± 3.3 (0–8). Different from previous studies, the pathological stages of the patients we included were pT2–3.
We suggested that the high rate of lymph node metastasis was mainly due to the staging of patients. In addition, the mean operative time for lobectomy and total thyroidectomy in this study were 142.4 ± 53.4 min and 160.0 ± 14.1 min, respectively, longer than that in Ahn's study (lobectomy 95.25 ± 32.02 minutes; total thyroidectomy 104.13 ± 34.54 minutes), shorter than that in Liu's study (194 minutes) and Wang's study (193 ± 47 minutes). However, compared with open surgery in previous studies, the operative time of TOETVA in this study is significantly longer.
As for the incidence of postoperative complications, the protection of RLN is of great importance in thyroidectomy. The incidence of permanent RLN injury and transient RLN injury in TOETVA was reported 0%–1.9% and 1%–20%, respectively.4,7,12,14,19 In this study, 1 patient had transient RLN injuries and recovered within 6 months. The rate of temporary hypoparathyroidism in this study was 20%, slightly higher than that in Anuwong's study on TOETVA (17.5%), and lower than that in Stoll's study on open thyroid surgery. (21.1%).7,21 Besides, tracheal injury, Horner syndrome, and other complications reported in previous studies did not occur in the included patients. In the follow-up after surgery, we suggest that neck ultrasound should be performed at 6 months, 1 year, and annually thereafter, and no other complications or tumor recurrence were found.
We proposed some suggestions for the TOETVA in the treatment of PTC with tumor size ≥2 cm. First, due to the limited working space, a hybrid method combining CO2 insufflation with surgical sutures was applied (Fig. 1), and the surgical assistant uses an endoscopic retractor to help broaden the working space (Fig. 2). In most cases, it also needs to partially disconnect the sternothyroid to exposing the superior pole of the thyroid (Fig. 3). Second, it is suggested to use nerve monitoring system during surgery to reduce the incidence of nerve injury. Third, due to technical difficulty, only experienced surgeons are recommended to expand the application of TOETVA to tumor size ≥2 cm.
This study has the following limitations: First, this is a retrospective study with a limited number of cases. The prospectively designed and controlled trial studies with large cohort are urgently needed. Besides, the mean follow-up time of patients included in this study is 23.8 ± 13.1 months, which is too short for patients with PTC. Long-term surgical outcomes of TOETVA for PTC with tumor size ≥2 cm require investigation by further research.
In summary, based on the satisfactory short-term outcomes recorded in this study, it is feasible to perform TOETVA for PTC patients with tumor size ≥2 cm. We suggested that experienced surgeons may expand the indications of TOETVA for patients with cosmetic needs.
Footnotes
Authors' Contributions
Writing—review and editing (equal) and writing—original draft (equal) by Z.-X.C. Conceptualization (lead) and writing—original draft (equal) by F.-S.P. Software (lead) and writing—original draft (equal) by J.-B.C. Methodology (lead) by J.-M.D. Formal analysis (lead) by Y.C. Conceptualization (supporting) and software (supporting) by X.-B.Z. and Z.-H.L. Methodology (supporting) and formal analysis (supporting) by B.-Y.C. and L.-M.Y. Writing—review and editing (equal) by Y.Q.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.