
Abstract
Background:
Achieving critical view of safety is a key for a successful laparoscopic cholecystectomy (LC) procedure. Near-infrared fluorescence cholangiography using indocyanine green (NIF-ICG) in LC has been extensively used and accepted as beneficial auxiliary tool to visualize extrahepatic biliary structures intraoperatively. This study aimed to analyze its safety and efficacy.
Materials and Methods:
Searching for potential articles up to March 25, 2022 were conducted on PubMed, Europe PMC, and ClinicalTrials.gov databases. Articles on the near infrared fluorescence during laparoscopy cholecystectomy were collected. Review Manager 5.4 software was utilized to perform the statistical analysis.
Results:
Twenty-two studies with a total of 3457 patients undergo LC for the analysis. Our meta-analysis revealed that NIF-ICG technique during LC was associated with shorter operative time (Std. Mean Difference −0.86 [95% confidence interval (CI) −1.49 to −0.23], P = .007, I2 = 97%), lower conversion rate (risk ratio [RR] 0.28 [95% CI 0.16–0.50], P < .0001, I2 = 0%), higher success in identification of cystic duct (CD) (RR 1.24 [95% CI 1.07–1.43], P = .003, I2 = 94%), higher success in identification of common bile duct (CBD) (RR 1.31 [95% CI 1.07–1.60], P = .009, I2 = 90%), and shorter time to identify biliary structures (Std. Mean Difference −0.52 [95% CI −0.78 to −0.26], P < .0001, I2 = 0%) compared with not using NIF-ICG.
Conclusions:
NIF-ICG technique beneficial for early real-time visualization of biliary structure, shorter operative time, and lower risk of conversion during LC. Larger randomized clinical trials are still needed to confirm the results of our study.
Introduction
Achieving critical view of safety is a key for successful laparoscopic cholecystectomy (LC) procedure. 1 LC seems associated with a higher incidence of bile duct injury (BDI) than open cholecystectomy resulting from poor visualization of anatomic structures. 2 BDI remain being most serious complications during LC with the incidence ranging from 0.3% to 1.5%. 3 Among many causes of intraoperative BDI, unclear identification of the bile duct account for 71%–97% of cases.4,5 Patient who sustain BDI may have significantly reduced quality of life for years afterward.6,7 These data showed that poor visualization of anatomical structures during LC still becomes a serious problem for a digestive surgeon. 8
Several interventions have been tried to prevent poor visualization of anatomical structure during LC such as conventional X-ray-based intraoperative cholangiography (IOC), but it is not adopted worldwide in standard cholecystectomy because of radiation side effect and manpower requirements.9–11
Another visual tool modalities currently studied for LC is near-infrared fluorescence cholangiography using indocyanine green (NIF-ICG). NIF-ICG during an LC has been extensively used as a beneficial auxiliary tool to visualize extrahepatic biliary structures intraoperatively. 12 Current up-to-date overview suggested that NIF-ICG could be a gold standard for all LC procedures in elective and emergency settings due to safety and low costs. 13 However, another review article also showed that the biliary tract visualization using NIF-ICG was equal when compared with IOC, negating the significant benefit of NIF-ICG in LC. 14 These conflicting evidences need to be resolved through a comprehensive meta-analysis study. This systematic review and meta-analysis study aim to summarize the latest evidence regarding the benefit of NIF-ICG during LC procedure compared with not using NIF-ICG.
Materials and Methods
Eligibility criteria
The inclusion criteria were formulated based on PICOS formulation as follows: (1) P—Population: patients who undergo LC procedure for any indications; (2) I—Intervention: using indocyanine green fluorescence technology to aid the visualization of biliary structures during LC; (3) C—Control: did not use indocyanine green fluorescence or only use any conventional methods; (4) O—Outcome: have data on one of the following outcomes: time of operation, duration of hospital stay, intraoperative complications, conversion rate, BDI, blood loss volume, success rate for cystic duct (CD) identification, success rate for common bile duct (CBD) identification, and time to identification of biliary structures; (5) S—Study design: clinical trials (either randomized or nonrandomized), cohort studies (either prospective or retrospective), case–control, cross-sectional studies, and case-series; (6) available as full-length articles (may include preprints).
Systematic review and meta-analysis study was performed from the clinical trials and observational studies based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 15 and Meta-analysis of Observational Studies in Epidemiology (MOOSE) 16 guidelines.
Meanwhile, the exclusion criteria for this study were as follows: (1) non-English language articles; (2) studies on robotic cholecystectomy; (3) studies which did not include any comparison group; (4) unpublished study or abstract; and (5) nonprimary research.
Search strategy and study selection
We searched the following databases for English-language articles up to March 25, 2022: ClinicalTrials.gov, PubMed, and Europe PMC. The following search strategy was used: “(indocyanine green OR ICG) AND (fluorescence OR fluorescent OR near-infrared OR cholangiography OR cholangiogram) AND (laparoscopic OR minimally invasive) AND (cholecystectomy OR gallbladder removal).” Two-stage screening process was done by 2 reviewers to identify publications that would be eligible for inclusion: screening for title and abstract, followed by full-text review. Any original articles referenced by systematic reviews but not identified by the initial search were also included if they were eligible. Any duplicates were subsequently removed. Any disagreement during screening process was resolved through discussion employed for our study.
Data extraction and quality assessment
Data from eligible articles were extracted independently by 2 reviewers, which include the following: authors' names, year of study, sample size, study design, indications for LC, ICG dose and timing, age, gender, body mass index (BMI), number of patients with ICG intervention, the comparison group in included studies, as well as the outcome of interest.
Two independent reviewers assessed the methodological quality of the included studies. In the present study, we used Modified Jadad Scale for clinical trials evaluation, which has four points of assessment: the randomization process, allocation concealment, blinding method, and withdrawals and dropouts of each study. 17 The studies were scored from zero to seven and a study ranked as a high-quality study if the score was >4. 17 Meanwhile, we used Newcastle–Ottawa Scale (NOS) to evaluate the quality of observational studies (cohort and case–control). 18 The NOS tool's point of assessment consisted of comparability, selection, and outcome of each study where each research was assigned a total score beginning with zero until nine. 18 Research is graded good if it scores ≥7. 18
Statistical analysis
For the dichotomous variable outcomes, Mantel–Haenszel formula was utilized to obtain the risk ratio (RR) and its 95% confidence interval (95% CI). For continuous variable outcomes, we used Inverse-Variance formula to obtain standardized mean difference (SMD) and its standard deviations (SD). Random-effects model was employed in this study, regardless of the heterogeneity. We calculated the I2 statistic as a measure of the overall variation in the proportion that was attributable to between-study heterogeneity, where a value of <25%, 26–50%, and >50% were considered as low, moderate, and high heterogeneity, respectively. Data reported as medians and interquartile ranges or as medians and minimum-to-maximum ranges were converted based on the formula by Wan et al 19 to obtain the mean and SD for meta-analysis pooling. The bias of publication in this study was assessed qualitatively by using funnel plot analysis. All of the statistical analysis was done by using Review Manager 5.4 software from Cochrane Collaboration.
Results
Study selection and characteristics
Database searches identified 674 studies. After reviewing the secondary reference lists from included articles, removing all duplicates, and screening the studies from titles/abstracts, a total of 108 studies were eligible for review in full text. Among these eligible articles, 86 articles were further excluded after full-text screening: 60 articles did not have comparison/control groups, 10 articles were robotic cholecystectomy, 7 articles were not primary research, 5 articles were not in English language, and 4 articles did not have data about the specified outcome of interest thus resulting in the final number of 22 studies,20–41 which included a total of 3457 patients undergoing LC for the analysis (Fig. 1). Out of 22 studies, 3 were single-blind randomized clinical trials (RCTs),25,30,37 1 was open-label RCT, 36 10 were prospective cohort,20,21,28,31–35,39,40 7 were retrospective cohort,22–24,26,27,29,41 and the remaining 1 article was case–control studies. 38 Sample sizes ranged from 20 to 1389. The three uttermost indications for LC in the included studies were cholelithiasis, choledocholithiasis, and acute cholecystitis.
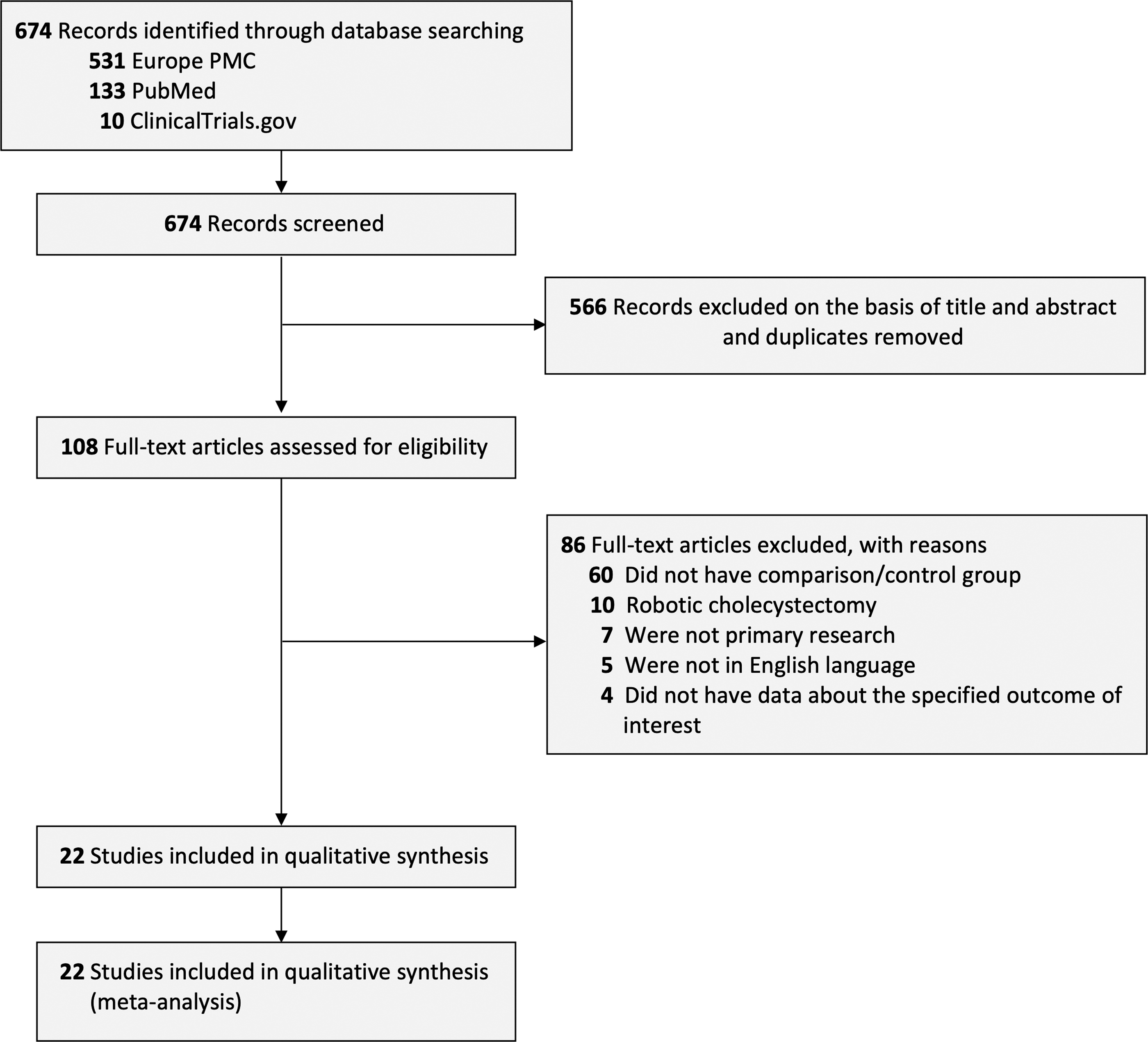
PRISMA diagram of the detailed process of selection of studies for inclusion in the systematic review and meta-analysis.
The dose for ICG used in the included studies varied from 0.05 mg/kg to 2.5 mg, which most of them were administered before the surgery. More details regarding each included research can be seen in Table 1.
Characteristics of Included Studies
Outcomes: 1, operation time; 2, length of hospital stay; 3, intraoperative complications; 4, conversion rate; 5, bile duct injury; 6, blood loss volume; 7, successful identification of cystic duct; 8, successful identification of common bile duct; 9, time to identification of biliary structures.
BMI, body mass index; ICG, indocyanine green; RCT, randomized clinical trials.
Quality of study assessment
The quality assessment using NOS scale revealed good quality for all included cohort and case–control studies (Table 2). The evaluation of included clinical trials using Jadad scale assessments also suggested that one clinical trial study was graded high quality, while another study was graded moderate quality (Table 3).
Newcastle–Ottawa Quality Assessment of Observational Studies
(1) representativeness of the exposed cohort; (2) selection of the nonexposed cohort; (3) ascertainment of exposure; (4) demonstration that outcome of interest was not present at start of study.
(1) comparability of cohorts on the basis of design or analysis, (maximum two stars).
(1) assessment of outcome; (2) was follow-up long enough for outcomes to occur; (3) adequacy of follow-up of cohorts.
Quality Appraisal of Studies Included in the Meta-Analysis Using Jadad Scale Assessment
We used Jadad scale to assess the included studies. Points were determined as follows,
I. Random allocation: computer-generated random numbers, 2 points; not described, 1 point; inappropriate method, 0 point.
II. Allocation concealment: central randomization, sealed envelopes or similar, 2 points; not described, 1 point; inappropriate or unused, 0 point.
III. Blindness: identical placebo tablets or similar, 2 point; inadequate or not described, 1 point; inappropriate or no double blinding, 0 point.
IV. Withdrawals and dropouts: numbers and reasons are described, 1 point; not described, 0 point.
ICG versus control
Operative time
Thirteen studies (n = 2349) reported on the operative time outcome. Our pooled analysis showed that using ICG technique for LC was associated with shorter operative time when compared with control (Std. Mean Difference −0.86 [95% CI −1.49 to −0.23], P = .007, I2 = 97%, random-effects modeling; Fig. 2A).
Forest plot that demonstrates the comparison between using ICG technique and not using ICG technique for laparoscopic cholecystectomy in terms of operative time
Length of hospital stay
Nine studies (n = 2127) reported on the length of hospital stay outcome. Our pooled analysis showed that using the ICG technique for LC did not differ with not using ICG technique in terms of length of hospital stay (Std. Mean Difference −0.64 [95% CI −1.29 to 0.01], P = .05, I2 = 96%, random-effects modeling; Fig. 2B).
Intraoperative complications
Sixteen studies (n = 3129) reported on the intraoperative complication outcome. Our pooled analysis showed that using the ICG technique for LC did not differ with not using ICG technique in terms of intraoperative complication rate (RR 0.73 [95% CI 0.43–1.23], P = .24, I2 = 0%, random-effects modeling; Fig. 2C).
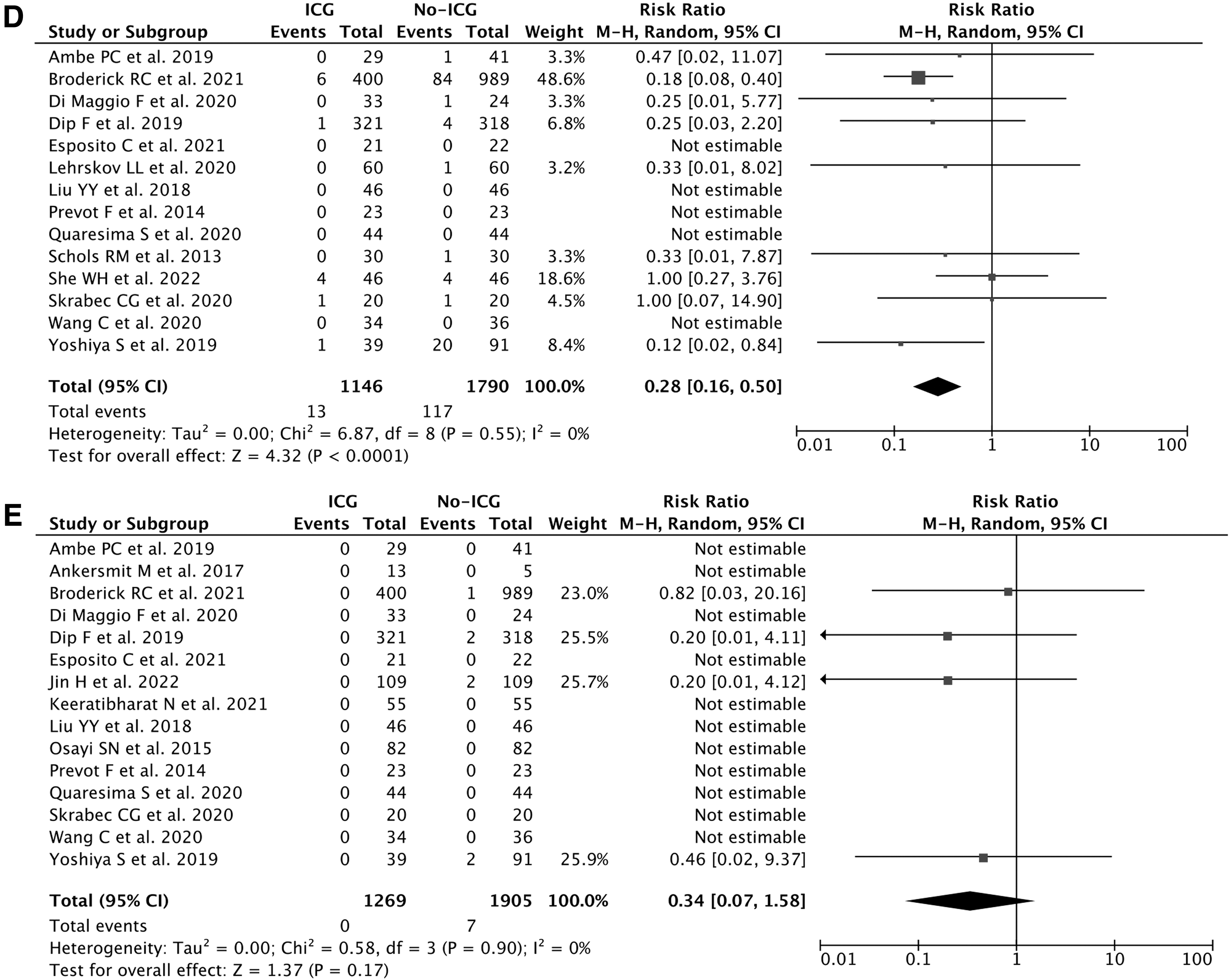
Conversion rate
Fourteen studies (n = 2936) reported on the conversion rate outcome. Our pooled analysis showed that using ICG technique for LC was associated with lower conversion rate when compared with not using the ICG technique (RR 0.28 [95% CI 0.16–0.50], P < .0001, I2 = 0%, random-effects modeling; Fig. 2D).
Bile duct injury
Fifteen studies (n = 3174) reported on the BDI outcome. Our pooled analysis showed that the risk for BDI did not differ between using the ICG technique and not using ICG technique for LC (RR 0.34 [95% CI 0.07–1.58], P = .17, I2 = 0%, random-effects modeling; Fig. 2E).
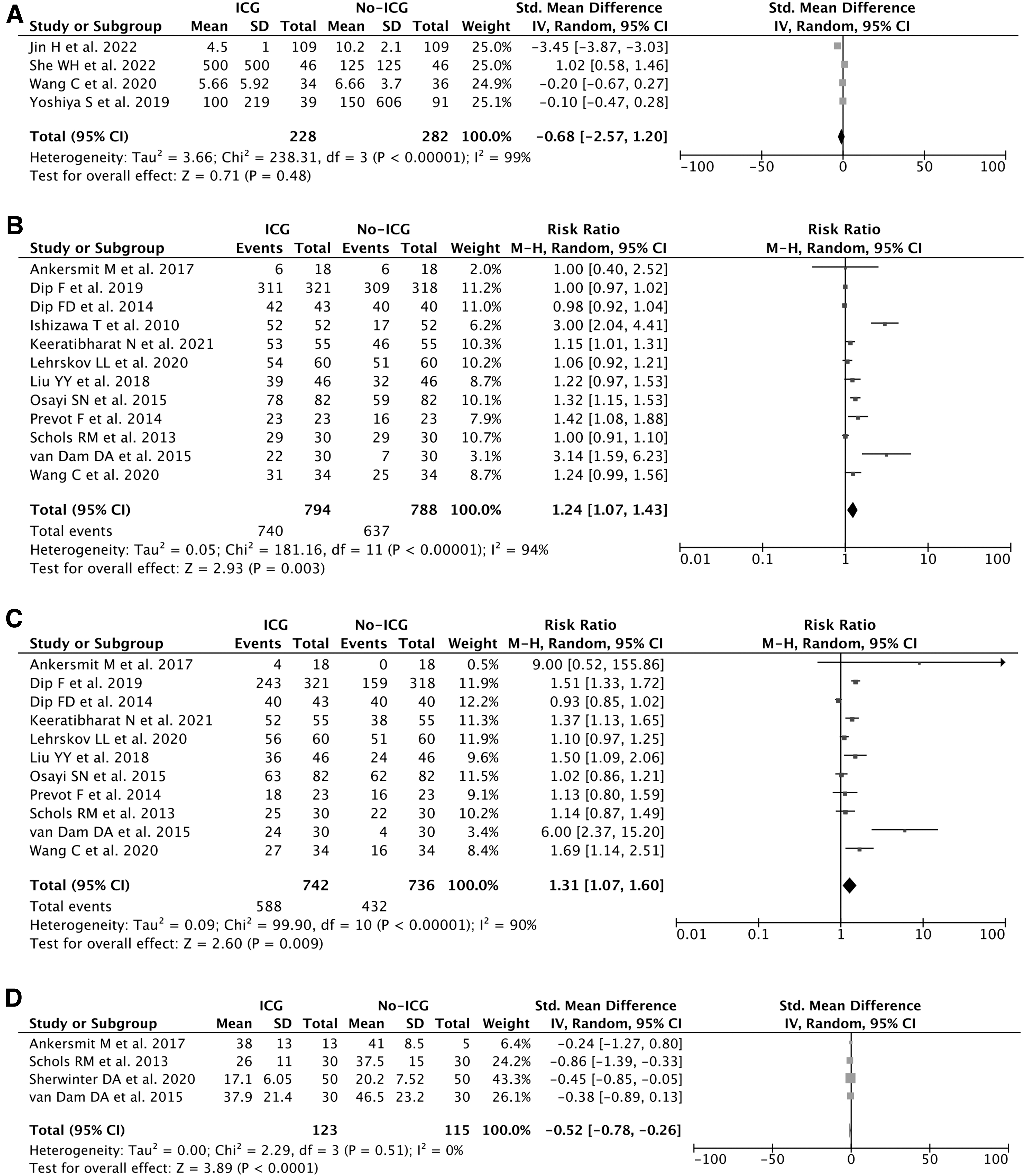
Blood loss volume
Four studies (n = 510) reported on the blood loss volume outcome. Our pooled analysis showed that using the ICG technique for LC did not differ with not using ICG technique in terms of blood loss volume (Std. Mean Difference—0.68 [95% CI −2.57 to 1.20], P = .48, I2 = 99%, random-effects modeling; Fig. 3A).
Forest plot that demonstrates the comparison between using ICG technique and not using ICG technique for laparoscopic cholecystectomy in terms of blood loss volume
Success rate for identification of CD
Twelve studies (n = 1582) reported on the success rate for identification of CD outcome. Our pooled analysis showed that using ICG technique for LC was associated with higher success rate for identification of CD when compared with the not-using ICG technique (RR 1.24 [95% CI 1.07–1.43], P = .003, I2 = 94%, random-effects modeling; Fig. 3B).
Success rate for identification of CBD
Eleven studies (n = 1478) reported on the success rate for identification of CBD outcome. Our pooled analysis showed that using ICG technique for LC was associated with higher success rate for identification of CBD when compared with the not-using ICG technique (RR 1.31 [95% CI 1.07–1.60], P = .009, I2 = 90%, random-effects modeling; Fig. 3C).
Time to identification of biliary structures
Four studies (n = 238) reported on the time to identification of biliary structure outcome. Our pooled analysis showed that time needed for identification of biliary structures was shorter while using ICG technique for LC compared with not using ICG technique (Std. Mean Difference −0.52 [95% CI −0.78 to −0.26], P < .0001, I2 = 0%, random-effects modeling; Fig. 3D).
Publication bias
Publication bias assessment from Funnel plot analysis showed a relatively symmetrical inverted-plot for all outcomes of interest in this study, indicating no publication bias (Fig. 4A–I).
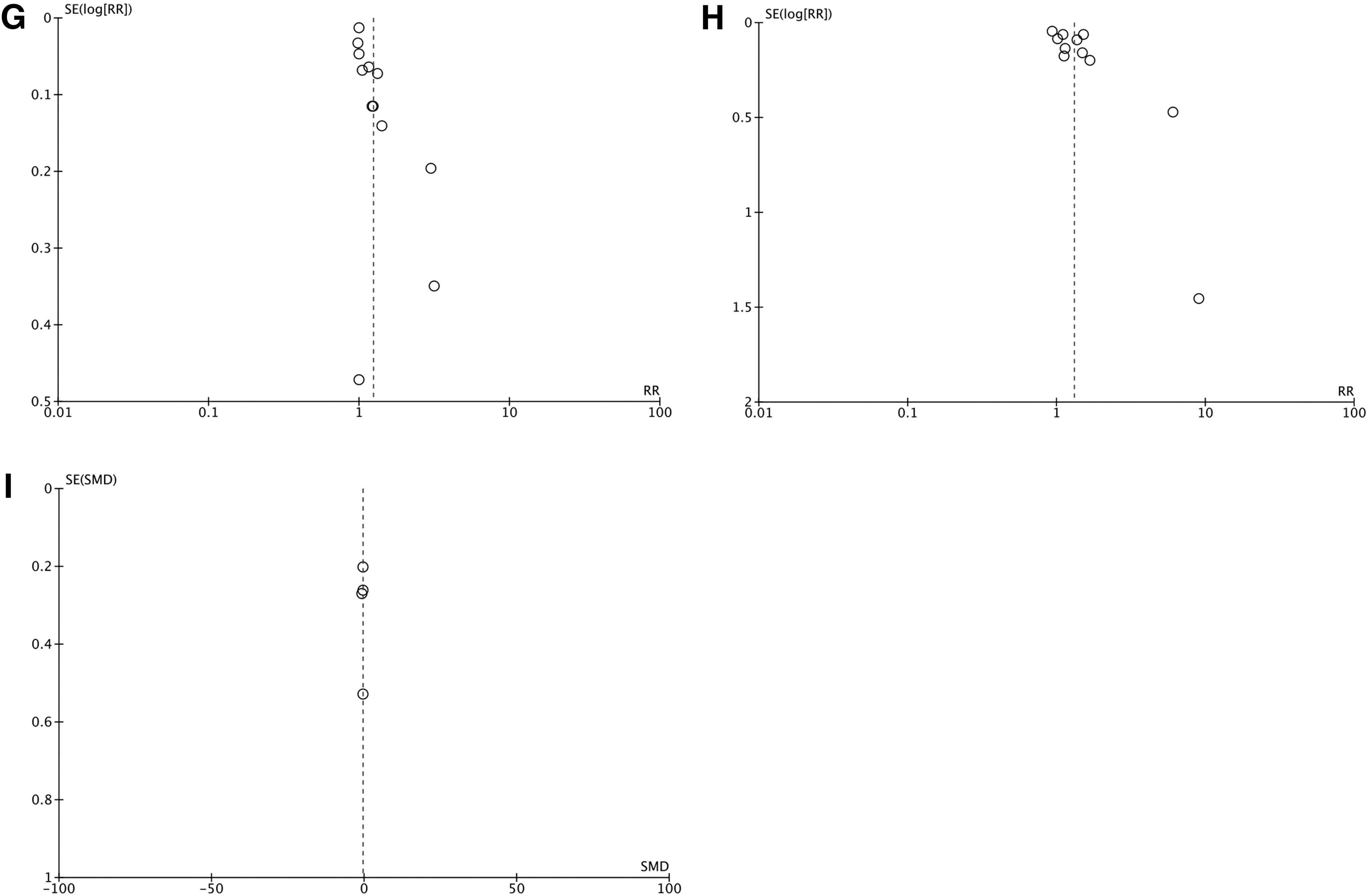
Funnel plot analysis for each outcomes of interest in this study: operative time
Discussion
According to our pooled analysis, it was discovered that NIF-ICG technique during LC was associated with shorter operative time, lower conversion rate, higher success rate for identification of CD, higher success rate for identification of CBD, and shorter time to identify biliary structures when compared with not using NIF-ICG technique. However, the length of hospital stay, intraoperative complication rate, risk of BDI, and blood loss volume did not differ significantly between using NIF-ICG technique and not using NIF-ICG technique during LC.
There are some explanations of how NIF-ICG could reduce operative time and conversion rate. ICG is a nontoxic, fluorescent, iodide dye, and when injected intravenously, it binds to plasma proteins, undergoes hepatic clearance, and excreted in the biliary system. 42 Using ICG technique may help in visualizing biliary structures earlier and easier by giving the surgeon a real time and image-guided tactile perception. Early identification of CD, CBD, and other biliary structures make the procedure going smooth and straight forward to evacuate bile and cystic duct by separating biliary structures with other tissues such as adhesion band and blood vessels. 43 If the biliary structures can be identified earlier and easier, the needs for conversion into open cholecystectomy can therefore be reduced and the operative time may also be shortened.
Regarding the incidence of BDI, blood loss volume, and intraoperative complications during LC, which did not differ between using NIF-ICG and not using NIF-ICG may be explained by several factors. First, the populations used in the included studies were heterogenous. Some studies included only uncomplicated gallbladder disease,20,39 while others have included both complicated and uncomplicated gallbladder disease.22,40 Moreover, some studies also included older (age >60 years) and obese patients (BMI >30 kg/m2) as the sample for their studies. In complicated gallbladder disease, especially in those who were old and obese, there may be a thickening of the tissue covered on the extrahepatic biliary tract structures, which make the dye penetration limited, thus making visualization of deeper structure or detection of lesion's location become difficult, even with NIF-ICG technique. 44 Second, most of the included studies were observational (cohort or case–control) by design. Different from randomized clinical trial studies, observational studies may be confounded by many biases, one of them is selection bias.
Patients included in the NIF-ICG and patients in the control group may not have comparable baseline characteristics, such as age, gender distribution, BMI, ASA score, preoperative diagnosis, and comorbidities. For example, in a study by Esposito et al, 26 the median BMI was higher in the NIF-ICG group than in the control group. NIF-ICG group in a study by Broderick et al 22 also have older age and higher Charlson Comorbidity Index (CCI) when compared with the control group. All of these factors may increase the complexity and influence the operative outcomes during LC.45,46
Our study is not free from limitations. Our analyses were based mostly on the observational studies, which have many biases, such as selection bias, information bias, and confounding. These biases may influence the results from the study. Majority of the outcomes of interest in this study also have notable heterogeneities. This might be due to differences in the sample characteristics, ICG dosage, and time to administration of ICG in each of the included studies. More randomized clinical trial studies with larger sample sizes and proper methodology are still needed to confirm the results from our study.
Conclusion
Our systematic review and meta-analysis concluded that NIF-ICG technique is beneficial for early real-time visualization of biliary structures, shorten operative time, and lower risk of conversion into open cholecystectomy.
Footnotes
Authors' Contributions
Data Availability Statement
The authors confirm that the data supporting the findings of this study are available within the article [and/or] its supplementary materials.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.