
Abstract
Background:
Pancreatoduodenectomy is a standard surgical procedure for periampullary tumors. With recent improvements in perioperative management, postoperative mortality has decreased significantly in recent years; however, postoperative pancreatic fistula (POPF) is still one of the most prevalent and dangerous complications. The purpose of this study was to analyze the prevalence of malnutrition and the value of predicting POPF in patients with laparoscopic pancreatoduodenectomy (LPD).
Methods:
We retrospectively analyzed the perioperative data of 747 patients undergoing LPD in the Department of Hepatobiliary and Pancreatic Surgery, The First Hospital of Jilin University, China. Simultaneously, we analyzed the prevalence rate of malnutrition with three different nutritional assessment scores and explored the independent risk variables for POPF to identify potential predictive value.
Results:
Malnutrition was observed in 20.1% of patients with the prognostic nutritional index (PNI), 85.0% of patients with the controlling nutritional status (CONUT) score, and 73.1% of patients with the NRI score. Univariate and multivariate analyses all showed that the risk factors for POPF were pancreatic texture, pancreatic duct diameter, abdominal infection, body mass index (BMI), nomogram-revised risk index (NRI), and PNI. The receiver operating characteristic curve indicated that the BMI/PNI ratio was capable of predicting the occurrence of clinical POPF following LPD, with an area under the curve of 0.708.
Conclusions:
Compared with no malnourished patients, malnutrition is associated with a higher risk of POPF among patients with LPD. In addition, the BMI/PNI ratio has some predictive value in the development of POPF following LPD.
Introduction
The mortality rates of pancreatoduodenectomy (PD) have decreased significantly in recent years with the development of laparoscopic instruments and surgical experience. Nevertheless, complications, such as postoperative pancreatic fistula (POPF) and hemorrhage, remained prevalent. Meanwhile, POPF, referred to as “the Achilles heel,” can result in abdominal bleeding, infection, and even death. It can also prolong hospitalizations and increase the cost of hospitalization. 1 Consequently, it is crucial to identify patients with a high risk of POPF to reduce its incidence. Some evidence has proven that malnutrition is a key prognostic factor for benign and malignant diseases,2–4 affecting recovery time, prolonged length of hospital stay, and decreased quality of life, as well as speeding up tumor progression, resulting in a bad prognosis.5–8 However, the prevalence of malnutrition and its impact on POPF are rarely described in patients with periampullary tumors who underwent laparoscopic pancreatoduodenectomy (LPD). Thus, in this study, we analyze the prevalence of malnutrition and discuss the impact on POPF.
Materials and Methods
General information
Between April 2015 and June 2021, the perioperative data of those patients with periampullary tumors were retrospectively analyzed at the Department of Hepatobiliary and Pancreatic Surgery, The First Hospital of Jilin University, China. POPF, postpancreatectomy hemorrhage (PPH), delayed gastric emptying (DGE), and bile leakage were defined and classified according to the corresponding international guidelines.9–12 Postoperative complications were categorized according to the Clavien–Dindo classification. 13 These patients were all performed by the same surgical team.
Clinical data were collected from medical electronic records. Preoperative data included: age, gender, body mass index (BMI), American Society of Anesthesiology Score (ASA), history of upper abdominal surgery, complication, preoperative biliary drainage, and laboratory data such as preoperative albumin (ALB) levels, serum lipid levels, and total lymphocyte count (TLC), which were selected based on recent preoperative data. Intraoperative data included: time of operation, estimated blood loss, pancreas texture, and pancreatic duct diameter. Postoperative parameters such as pancreatic postoperative pancreatic fistula (POPF), PPH, intra-abdominal infection, DGE, and bile leakage were all collected from database.
Inclusion and exclusion criteria
Inclusion criteria were as follows: (1) Patients who were diagnosed with cancers around ampulla; (2) patients who did not receive neoadjuvant therapy; and (3) there was no distant metastasis. Exclusion criteria were as follows: (1) Patients without these nutritional indicators, such as height, weight, ALB level, lymphocyte count, and total cholesterol level before surgery; (2) death within 30 days; (3) immune-boosting agents, hormones, or blood transfusion were administered before surgery; and (4) patients who received palliative surgical interventions.
Malnutrition screening tools
BMI of all the patients were collected; meanwhile, patients were divided into underweight (<18.5 kg/m2), normal weight (18.5 to 25.0 kg/m2), overweight (25.0 to 28.0 kg/m2), and obesity (≥28 kg/m2) based on BMI. In addition, we screened for malnutrition with three different ways (controlling nutritional status [CONUT]/prognostic nutritional index [PNI]/nomogram-revised risk index [NRI]) (Supplementary Table S1). The CONUT score is composed of the serum values of ALB, TLC, and total cholesterol. 14 The PNI score consists of 10 × serum ALB (g/dL) +0.005 × TLC (mm3). 15 The NRI was made up of 1.489 × serum ALB +41.7 × current body weight (kg)/usual body weight. 16 Malnutrition is classified according to the CONUT score (scores of 2–4, 5–8, and 9–12 reflected mild, moderate, and severe malnutrition, respectively). Malnutrition is also graded as mild, moderate, or severe based on the NRI score (scores of 97.5 ≤ NRI <100, 83.5 ≤ NRI <97.5, or NRI <83.5, respectively). However, the malnutrition can also be divided into two categories based on the PNI score (scores of 35–38 and <35 reflect moderate and severe malnutrition, respectively).
Statistical analysis
Data were analyzed using SPSS 21.0 statistical software and were divided into categorical and continuous variables. If continuous variables were a normal distribution, they were expressed as (X ± s). And, independent samples t-tests were used to compare the two groups. If not, median (interquartile range) was used.
Comparison between groups was performed by the Mann–Whitney U test. Categorical variables were expressed as numbers and percentages; meanwhile, we compared the two groups using the χ 2 test or Fisher's exact test. P < .05 was considered statistically significant.
Results
Patient characteristics
A total of 747 patients underwent LPD with periampullary carcinomas in our center. The baseline characteristics of these patients are shown in Table 1. The average age and BMI were 62.21 ± 6.34 years and 22.87 ± 2.90 kg/m2, respectively. Three hundred twenty-nine (44.0%) patients were female, while 418 (56.0%) patients were male. The average intraoperative blood loss and the duration of surgery were 168.84 (50–200) mL and 254.83 ± 42.61 minutes, respectively. In addition, 574 (76.8%) patients were categorized as ASA grades 1–2. There were 135 individuals who had previously undergone upper abdominal surgery.
Baseline Characteristics of the Patients
ASA, American Society of Anesthesiology Score; BMI, body mass index; CONUT, controlling nutritional status; ENBD, endoscopic nasobiliary drainage; IPMN, Intraductal papillary mucinous neoplasm; NRI, nomogram-revised risk index; PNI, prognostic nutritional index; PTCD, percutaneous transhepatic cholangial drainage; PTGB, percutaneous transhepatic gallbladder bile drainage.
Indications for LPD included distal cholangiocarcinoma in 225 (30.1%) patients; the remaining instances involved pancreatic cancer in 190 (25.4%) patients, ampullary tumor in 140 (18.7%) patients, and duodenal cancer in 40 (5.4%) patients. Before surgery, 291 patients had severe jaundice. Among them, 217 (74.6%), 68 (22.9%), and 6 (2.1%) had percutaneous transhepatic gallbladder bile drainage, percutaneous transhepatic cholangial drainage, and endoscopic nasobiliary drainage, respectively. The severe complications (≥Clavien-Dindo [CD] III) occurred in 156 patients (20.9%); POPF, PPH, DGE, bile leakage, and intra-abdominal sepsis were observed in 103 (13.7%), 53 (7.1%), 25 (3.3%), 23 (3.1%), and 78 (10.4%), respectively. Meanwhile, the average length of hospital stay was 14.27 ± 3.26 days.
Prevalence and clinical associations of malnutrition
Malnutrition was found in 20.1% of patients with the PNI score, 85.01% of patients with the CONUT score, and 73.09% of patients with the NRI score. According to CONUT, NRI, and PNI, 282 (37.8%), 429 (57.4%), and 151 (20.2%) patients, respectively, had moderate-to-severe malnutrition. Despite the fact that all malnutrition indices were correlated, only 148 (19.8%) patients were classified as malnourished (any degree of malnutrition) by three scores, and only 39 (5.2%) patients were classified as not malnourished by any ways. And, according to BMI classification, patients with a BMI <25 kg/m2 had the highest prevalence of malnutrition. The three different ways of CONUT (55.2%), NRI (55.3%), and PNI (19.9%) identified a significant proportion of patients with a BMI of >25 kg/m2 who were malnourished (Fig. 1).
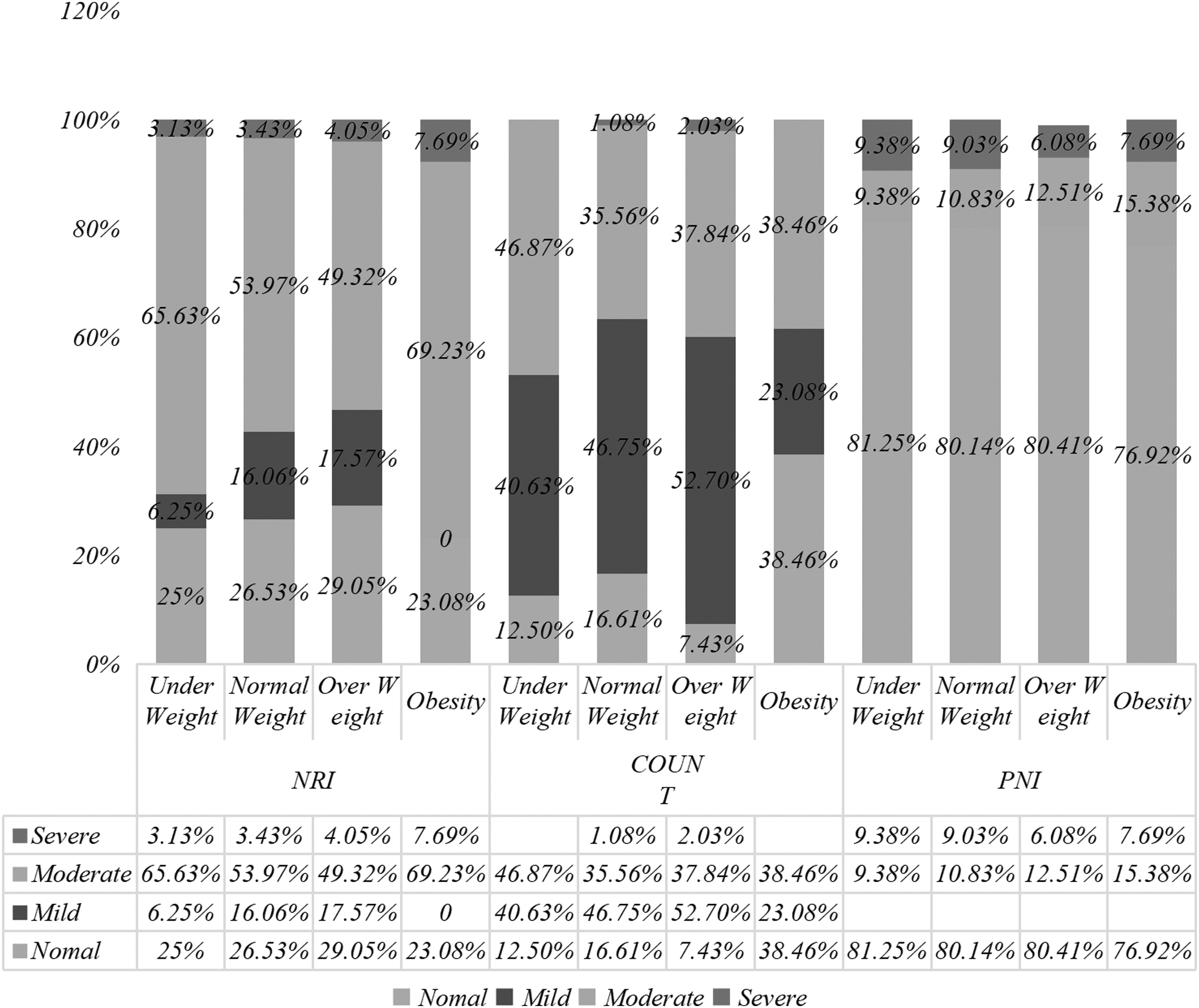
The prevalence of malnutrition according to body mass index. CONUT, controlling nutritional status; NRI, nomogram-revised risk index; PNI, prognostic nutritional index.
The relevant of malnutrition scores and pancreatic fistula
According to the three different nutritional scores and BMI classification, the incidence of POPF (Grade B/C) was related to nutritional status. When compared with mild and severe malnutrition, the incidence of POPF was lowest under normal nutritional status. According to the CONUT score, the incidence of POPF in those patients who were not malnourished was 10.71%. However, POPF were significantly higher in patients with mild, moderate, and severe malnutrition, and these distinctions were statistically significant (P < .05; Supplementary Table S2). Surprisingly, when we used NRI, PNI, and BMI to assess the relationship between nutritional condition and POPF, we discovered that there were also statistical significance across different categories (P < .05; Supplementary Tables S3–S5).
Comparison of factors between patients with clinical POPF and those without clinical POPF
To find significant risk factors for clinical POPF, we compared the variables between the patients with clinical POPF (n = 103) and those without clinical POPF (n = 644) (Table 2). Among the variables, BMI, NRI, PNI, pancreatic duct diameter, pancreas texture, and intra-abdominal infection tended to be relevant with clinical POPF. Patients with clinical POPF had a considerably higher BMI than those without clinical POPF (24.04 ± 3.06 kg/m2 vs. 22.68 ± 2.84 kg/m2, P < .001). The level of preoperative ALB in the POPF group was significantly lower than that in the no-POPF group (34.38 ± 4.69 g/L vs. 36.91 ± 4.28 g/L, P < .001). Patients with clinical POPF also exhibited more inferior nutritional status based on NRI, CONUT, and PNI scores than those without clinical POPF (all P < .05).
Univariate Analysis of Risk Factors of Clinical Postoperative Pancreatic Fistula After Laparoscopic Pancreatoduodenectomy
BMI, body mass index; CONUT, controlling nutritional status; NRI, nomogram-revised risk index; PNI, prognostic nutritional index; POPF, postoperative pancreatic fistula.
Meanwhile, we found that a higher prevalence of soft pancreas in the POPF group compared with without POPF group (58.25 vs. 45.63, P = .011). Pancreatic duct diameters were significantly smaller in the clinical POPF group than in the no-POPF group (3.31 ± 0.79 mm vs. 3.58 ± 1.19 mm, P = .028). There is no statistical significance in intraoperative blood loss and operative time. In regard to postoperative variables, the incidence of abdominal infection in the POPF group was significantly higher than that in the no-POPF group; meanwhile, the difference between the two groups was statistically significant (30.1% vs. 7.3%, P < .001). In addition, we conducted multivariate analysis for factors predicting POPF using a logistic regression analysis. Higher BMI, poor nutritional status (according to NRI and PNI), intra-abdominal infection, and postoperative hemorrhage were found to be independent risk variables associated with clinical POPF in multivariate analysis (Table 3).
Multivariate Analysis of Risk Factors of Clinical Postoperative Pancreatic Fistula After Laparoscopic Pancreatoduodenectomy
BMI, body mass index; CI, confidence interval; CONUT, controlling nutritional status; NRI, nomogram-revised risk index; PNI, prognostic nutritional index.
Analysis of the BMI/PNI ratio as a predictor for clinical POPF
In order to better predict POPF, we combine any two independent risk factors, such as BMI, PNI, NRI. As a consequence, we compared the BMI/PNI and BMI/NRI ratios between the two groups and discovered that the BMI/PNI (0.538 ± 0.102 vs. 0.622 ± 0.115) and BMI/NRI (0.235 ± 0.361 vs. 0.261 ± 0.364) ratios in the no-POPF group were significantly higher than those in the POPF group (all P < .05). The receiver operating characteristic curve indicated that the BMI/PNI ratio was capable of predicting the occurrence of clinical POPF following LPD, with an area under the curve (AUC) of 0.708. The AUC of the BMI/PNI ratio was greater than that of BMI (0.630), PNI (0.635), and NRI (0.619) alone (Fig. 2). When the cutoff of the BMI/PNI ratio was set to 0.573, the sensitivity and specificity for POPF prediction were 65% and 66%, respectively.
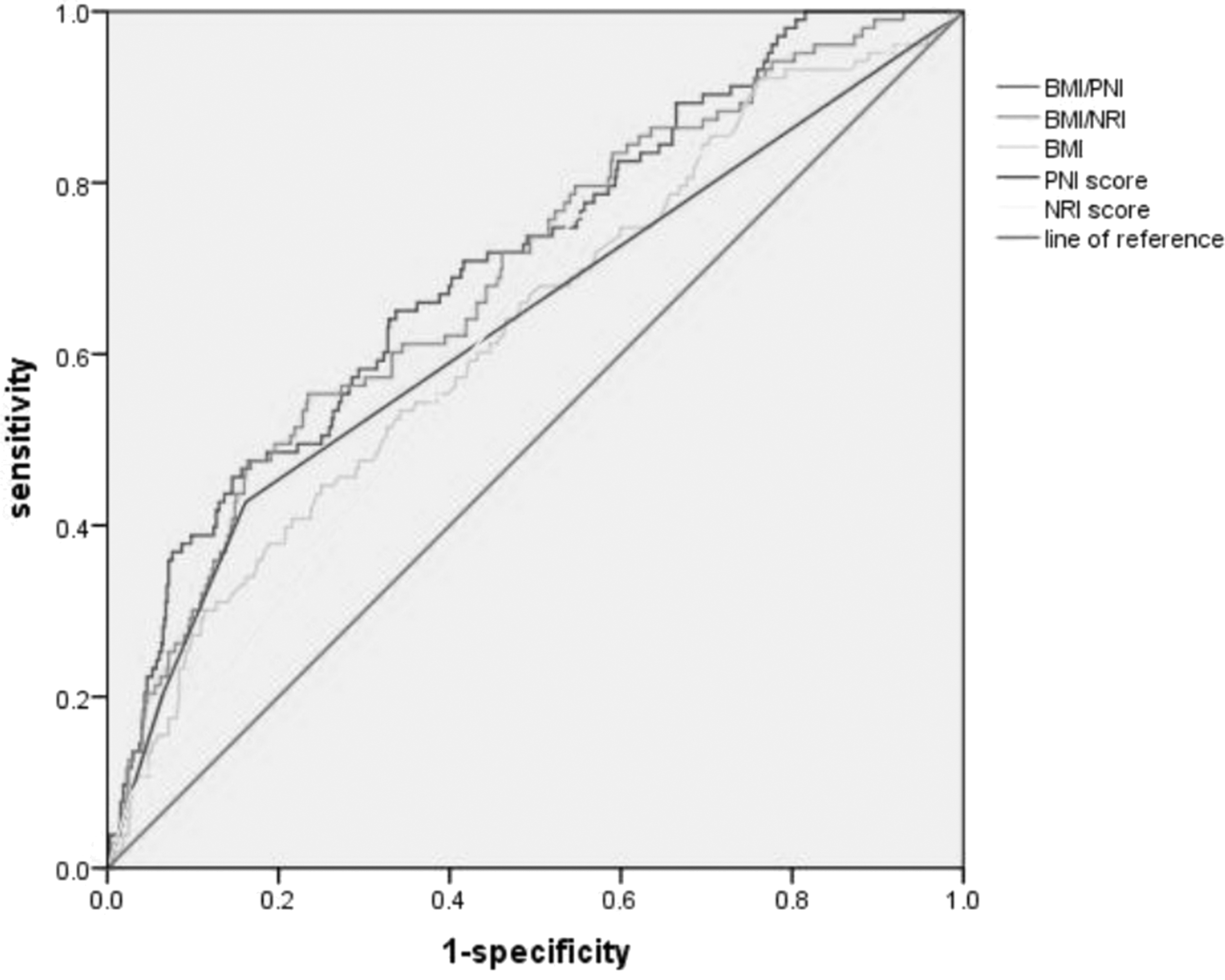
The receiver operating characteristic curve analysis proved that the BMI/PNI ratio could predict the occurrence of postoperative pancreatic fistula (AUC = 0.708). AUC, area under the curve; BMI, body mass index; NRI, nomogram-revised risk index; PNI, prognostic nutritional index.
Discussion
PD, as one of the biggest abdominal surgeries, can cause significant alterations in metabolism and nutritional status through activation of an inflammatory cascade and the release of stress hormones and cytokines. 17 During the past decade, LPD has become increasingly popular at home and abroad because perioperative management has improved. There is less invasiveness in LPD compared with open pancreaticoduodenectomy, but it needs to be further researched on oncological results. Surgical trauma can also weaken the immune system; 18 meanwhile, this response appears to be related to the level of surgical trauma.
Simultaneously, an increasing number of reports have indicated that the inflammatory response and immune system played a significant role in tumor invasion, metastasis, and progression.19,20 There was a high rate of malnutrition and cancer cachexia in cancer that affected the upper gastrointestinal (GI) system and the pancreas, with almost 80% experiencing it. Meanwhile, cancer cachexia is also one of the most common signs of pancreatic cancer, with weight loss occurring in 85% of patients even before diagnosis; simultaneously, cachexia is related to a lower quality of life, so it has an negatively impact on overall survival.21,22 Meanwhile, about 20% of all cancer-related deaths can be attributed to cachexia.
POPF is one of the most prevalent and dangerous postoperative complications, which could lead to bleeding, abdominal infection, and even death. 1 A great number of studies have been reported that preoperative nutritional state would not only raise the risk of POPF but also have an effect on long-term survival.23–25 Around 20%–50% of patients are diagnosed with moderate–severe malnutrition according to the CONUT, NRI, and PNI score in our department. The PNI was determined based on lymphocytes and the ALB. Typically, hypoalbuminemia typically leads to a decrease in collagen production, impaired wound healing, and compromised immune function. 26 It is for this reason that hypoproteinemia is often associated with surgical site infections. In the same way, the amount of lymphocytes in the body also reflects the body's nutritional status and immune function.
As a result of systemic inflammation, lymphopenia occurs, which suppresses cellular immunity in a striking manner. It has been shown that patients with low PNI scores (malnutrition) are more likely to develop postoperative complications. CONUT is similar to PNI except that it includes cholesterol. Therefore, CONUT reflects protein, lipid metabolism, and immune status. There is evidence that postoperative complications are associated with low serum cholesterol following GI surgery. 27 Cholesterol reductions indicate a lack of calories as well as essential nutrients for maintaining the integrity of cell membranes and metabolic function of the cells. 14 It is possible to illustrate the relationship between cholesterol level and POPF by examining tissue fragility.
Based on our data, we found that preoperative malnutrition was an independent risk factor for POPF. In addition, the diameter of pancreatic duct, abdominal infection, pancreatic texture, postoperative hemorrhage, BMI, CONUT, PNI, and NRI were also independently associated with POPF. Although there are some POPF prediction systems at present, these systems often require the combination of preoperative, intraoperative, and postoperative, which are complicated and difficult to be implemented in daily practice.28,29 As a result, we combined preoperative nutritional indicators that are independently associated with POPF by multivariate analysis to predict POPF and discovered that the BMI/PNI ratio has some predictive value for POPF (AUC = 0.708), which is a simple and useful preoperative indicator of POPF.
According to a number of studies, BMI is an independent risk factor for POPF;30,31 however, among some people, fat distribution is not equal. Therefore, the BMI/PNI ratio can be used to predict the probability of POPF, which is more accurate than BMI. The BMI/PNI ratio can quickly identify those patients who benefit from preoperative nutritional support, thereby reducing the incidence of POPF. 32 But, there are different contributions of lean body mass and fat mass to BMI. For example, for similar BMI values, Asian people usually have a higher percentage of body fat than Western people. Therefore, Asian people have a higher ratio of visceral fat to subcutaneous fat than Western people. 33 So, this result may not be generalizable to Western populations that have much higher BMIs. Meanwhile, with the rapid development of science and technology, robotic PD has been gradually performed in large pancreatic surgery centers all over the world. However, whether this result is suitable for robotic PD needs to be further verified.
In conclusion, malnutrition is a highly widespread problem among those patients with periampullary carcinomas. And, patients with malnutrition had a higher incidence of POPF compared with those without malnutrition, along with bad results. The BMI/PNI ratio has a certain prognostic significance for POPF after LPD, which is a simple preoperative indicator. However, as a retrospective study, prospective studies with a great number of people are needed to verify this finding.
Data Availability Statement
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Footnotes
Acknowledgment
The authors thank Y.D. who came up with the idea.
Authors' Contributions
S.W. and L.L. created the study design. Y.D. and Y.L. performed the data collection. S.W. was involved in data analysis and interpretation. All authors wrote the article and substantially revised the article.
Disclosure Statement
The authors declare that no competing interests exist.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.