
Abstract
Purpose:
Our aim was to expand existing evidence on structural determinants of cardiovascular health disparities among lesbian, gay, and bisexual (LGB) adults by examining sexual orientation differences in the impact of sexual orientation-related nondiscrimination laws on 30-year cardiovascular disease (CVD) risk.
Methods:
We analyzed data from Waves III (2001–2002), IV (2008–2009), and V (2016–2018) of the National Longitudinal Study of Adolescent to Adult Health. Sexual orientation was categorized as exclusively heterosexual, mostly heterosexual, bisexual, or gay/lesbian. We categorized changes in sexual orientation-related nondiscrimination laws between Waves III-IV as no change (reference group), increased, or decreased. We assessed 30-year CVD risk at Wave V using the Framingham Risk Score. We ran sex-stratified regression models to examine whether the association between changes in sexual orientation-related nondiscrimination laws and 30-year CVD risk was moderated by sexual orientation.
Results:
The sample included 3768 participants (mean age [standard deviation] = 28.7 [±1.72] years) of whom approximately 77% were White, 11% Hispanic, and 51% female. Compared with exclusively heterosexual participants, an increase in nondiscrimination laws was associated with lower CVD risk among mostly heterosexual women (B = −5.05, 95% confidence interval [CI] = −8.50 to −1.59) and gay men (B = −10.22, 95% CI = −19.05 to −1.39). There were no significant differences for other LGB subgroups when compared with exclusively heterosexual adults.
Conclusions:
Increasing laws that prohibit sexual orientation-related discrimination may play an important role in reducing CVD risk among some LGB subgroups. These findings can inform structural-level interventions to reduce CVD risk among LGB adults.
Keywords
Introduction
Cardiovascular disease (CVD) is the leading cause of death among adults in the United States. 1 More than 70% of CVD risk is attributed to modifiable risk factors. 2 Despite significant racial, ethnic, and income disparities in cardiovascular health in the United States,3–5 prior work has largely excluded examination of disparities related to sexual orientation. 6 There is growing evidence that lesbian, gay, and bisexual (LGB) adults have a higher prevalence of CVD risk factors compared to their heterosexual counterparts. 6 LGB adults are more likely to be current smokers than heterosexual adults.7–9 Gay and bisexual men as well as bisexual women are at higher risk of hypertension than their heterosexual counterparts.10–15 Similarly, bisexual men are twice as likely to have elevated blood pressure compared with heterosexual men. 16 In addition, lesbian and bisexual women are more likely than heterosexual women to have a body mass index (BMI) greater than 30 kg/m2.6,17 Lesbian and bisexual women as well as bisexual men may be at higher risk of diabetes than heterosexual adults.10,18,19 In contrast, gay men are at a lower risk of diabetes and elevated BMI than heterosexual men.8,20
Most research on cardiovascular health disparities among LGB adults has focused on individual risk factors for CVD. Comprehensive measures of CVD risk, such as the Framingham Risk Score (FRS), provide more accurate assessments of future CVD risk than individual risk factors. The FRS is a sex-specific, multivariable risk factor algorithm that can be used to predict a composite 30-year risk of ‘hard’ CVD that includes hard coronary heart disease (i.e., heart attack) and stroke (i.e., fatal and non-fatal). 21
Few studies have examined differences in cumulative CVD risk between LGB and heterosexual adults.22–26 A study using Wave IV data from the National Longitudinal Study of Adolescent to Adult Health (Add Health) reported that mostly heterosexual women had higher 30-year CVD risk using the FRS than exclusively heterosexual women, but no sexual orientation differences were found among men. 24 Using data from the National Health and Nutrition Examination Survey (2001–2010) investigators found that lesbian and bisexual women and bisexual men had higher 10-year CVD risk versus their heterosexual counterparts.25,26 In contrast, gay men had a lower 10-year CVD risk than heterosexual men. 26 Although the aforementioned studies have provided valuable data on CVD risk among LGB adults, there is a need to examine social and structural determinants of these disparities.
The minority stress model proposes that LGB individuals are exposed to significant minority stressors, defined as chronic psychosocial stressors experienced due to heterosexism.27,28 A recent adaptation extended the minority stress model to cardiovascular health. 6 This adaptation posits that, as a marginalized population, LGB individuals are exposed to minority stressors at the individual, interpersonal, and structural levels that may contribute to greater risk of CVD through mediated psychological (e.g., depression), behavioral (e.g., tobacco use), and physiological (e.g., increased inflammation) pathways. 6 Research on the link between minority stressors and CVD risk among LGB adults is sparse22,29–31 as most studies have focused on individual-level differences with limited attention to social and structural determinants. 6 A recent systematic review of 18 studies found that although there is growing research on social determinants of cardiovascular health among LGB adults, there is a significant gap regarding structural determinants. 32
Structural stigma is defined as “societal-level conditions, cultural norms, and institutional policies that constrain the opportunities, resources, and wellbeing of stigmatized populations.”33,34 Structural stigma (in the form of homophobia) is associated with adverse substance use, sexual and reproductive, and mental health outcomes, as well as higher all-cause mortality among LGB individuals.35–41 In a review of 98 studies that examined the influence of structural stigma on health outcomes among lesbian, gay, bisexual, transgender, queer, and questioning (LGBTQ+) people, 58 studies operationalized structural stigma as the presence of discriminatory policies. 33 The aforementioned review included several studies that examined CVD risk factors, including tobacco use (n = 14) and BMI (n = 1). Further, two studies have examined the impact of structural stigma on hypertension risk among LGB adults.42,43 A study using Add Health data found that LGB women living in states with more sexual orientation-related nondiscrimination laws had a 27% lower risk of reporting maternal hypertension. 42 Another study found a decrease in the total number of medical visits for hypertension among gay and bisexual men after the legalization of same-sex marriage in Massachusetts. 43
To date, there has been no comprehensive examination of the influence of sexual orientation-related nondiscrimination laws on cumulative CVD risk among LGB adults. Understanding changes in sexual orientation-related nondiscrimination laws over time provides an opportunity to examine how fluctuations in the sociopolitical environment, which often reflect shifts in societal attitudes, influence health outcomes. 33 Therefore, we analyzed data from Add Health to examine the impact of sexual orientation-related nondiscrimination laws on CVD risk among LGB and heterosexual adults. We leveraged Add Health’s longitudinal design to, for the first time, examine whether changes in sexual orientation-related nondiscrimination laws between Waves III and IV were associated with CVD risk among LGB and heterosexual adults at Wave V. Only one prior study has analyzed the impact of changes in state-level policies on health outcomes among LGB adults; however, that study focused on HIV-related outcomes among men who have sex with men. 40
We hypothesized that changes in state-level sexual orientation-related nondiscrimination laws between Wave III and IV would be: (1) associated with 30-year CVD risk at Wave V in the full sample of LGB and heterosexual adults (including both men and women) and (2) more strongly associated with 30-year CVD risk at Wave V among LGB adults relative to exclusively heterosexual adults.
Methods
Sample
We analyzed data from Add Health, a nationally representative longitudinal study that began in 1994. Approximately 90,000 students (Wave I, aged 12–18) were recruited from 80 high schools and 52 middle schools throughout the United States. A subsample of 20,747 participants were invited to complete additional in-home interviews and follow-up assessments in 2001–2002 (Wave III; aged 18–26), 2008–2009 (Wave IV; aged 24–32), and 2016–2018 (Wave V; aged 34–43). Wave IV (n = 15,701) was the first to include cardiovascular measures. This present study was deemed exempt by the Institutional Review Board of Columbia University Irving Medical Center as data were deidentified.
The Wave V Biomarker subsample included 5377 participants. We included all participants with complete data for indicators of state-level sexual orientation-related nondiscrimination laws (at Waves III and IV) as well as sexual orientation and cardiovascular data (at Wave V). We excluded participants who indicated they were not sexually attracted to either males or females (n = 8), those with a history of heart attack (n = 40) or stroke (n = 27), and those who were pregnant at Wave V (n = 54) to avoid bias due to gestational diabetes and hypertension that are common during pregnancy.44–46 Data on sexual orientation-related nondiscrimination laws were not available for Wave V. Our sample included 3768 participants (see Fig. 1).
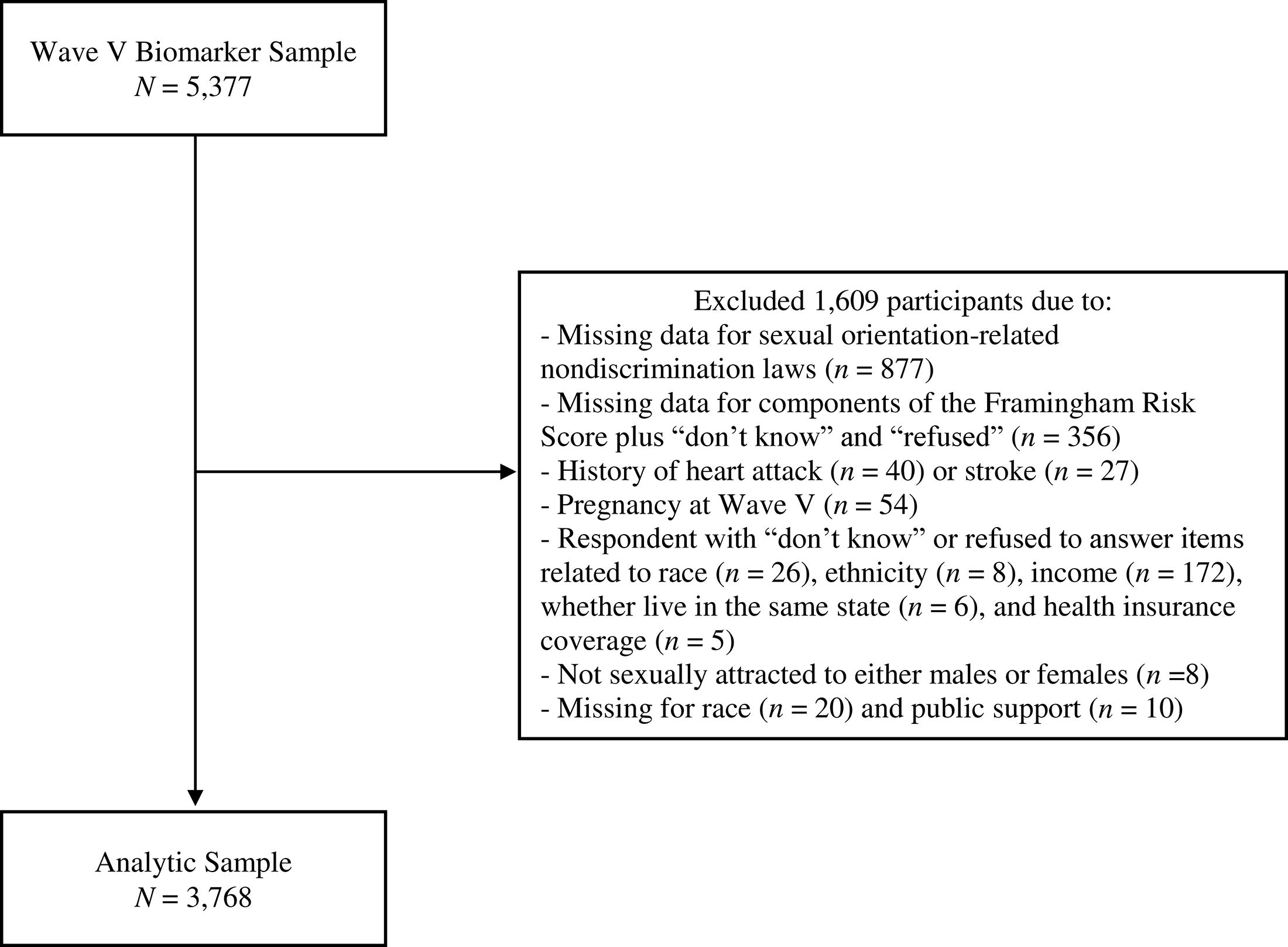
Flowchart of inclusion and exclusion criteria.
Measures
At Wave IV, participants were asked to choose which of the following best fit with their sexual orientation: “100% heterosexual (straight),” “mostly heterosexual (straight), but somewhat attracted to people of your own sex,” “bisexual, that is, attracted to men and women equally,” “mostly homosexual (gay), but somewhat attracted to people of the opposite sex,” “100% homosexual (gay),” and “not sexually attracted to either males or females.” Those who reported they were “not sexually attracted to either males or females” were excluded. As has been done in prior Add Health studies focused on LGB health, we combined mostly gay and 100% gay participants into the categories of “gay/lesbian” for women and “gay” for men.41,42 Sexual orientation was recategorized as “exclusively heterosexual,” “mostly heterosexual,” “bisexual,” and “gay/lesbian.”
Four sexual orientation-related nondiscrimination laws were assessed using geocoded data collected at Waves III and IV and captured respondents who lived in states that: (1) prohibited employment discrimination based on sexual orientation, (2) had hate crime statutory provisions based on sexual orientation, (3) allowed same-sex marriage/domestic partnership/civil union/reciprocal beneficiary relationships, and (4) allowed same-sex joint adoption and/or second-partner adoption. Consistent with prior work, two count variables accounting for sexual orientation-related nondiscrimination laws were created (range 0–4) for Wave III and Wave IV separately.37,41
We created a three-level categorical variable accounting for the change in sexual orientation-related nondiscrimination laws from Wave III to Wave IV by calculating the difference in nondiscrimination laws between both waves (no change [reference group], increased, and decreased). This variable captures both changes in the legal environment in a given state as well as whether participants moved to a state that had similar, increased, or decreased nondiscrimination laws.
The FRS comprehensively measures CVD risk and is a strong predictor of future CVD events and cardiovascular mortality.47–50 The 30-year FRS CVD risk score (vs. the 10-year FRS) is recommended in individuals under the age of 59 because CVD prevalence is generally low in this population. 51 Components of the 30-year FRS include sex, age, systolic blood pressure, anti-hypertensive medication use, current smoking, BMI (kg/m2), and diagnosis of diabetes.
In-home interview, medication inventory, and biomarker data were used to assess each component of the 30-year FRS at Wave V. 52 Age and current smoking were self-reported. At Wave V, a subsample of participants completed in-home cardiovascular assessments. The Wave V cardiovascular protocol has been previously described. 52 Three blood pressure assessments were collected, separated by at least 30 seconds. A variable accounting for average systolic blood pressure was constructed as the mean of the second and third blood pressure readings. 52
To assess the use of anti-hypertensive medication at Wave V, participants were asked to provide the names of all prescription medications they had used within the past four weeks. Those who reported using one or more anti-hypertensive medications were categorized as “yes.” Detailed information about the medication inventory at Add Health Wave V is provided elsewhere. 53
BMI (kg/m2) was assessed using height and weight measured to the nearest 0.5 cm and 0.1 kg, respectively.
Diagnosis of diabetes was determined by asking: “Has a doctor, nurse, or other health care provider ever told you that you have or had high blood sugar or diabetes?” Responses were yes versus no.
We assessed individual- and state-level factors that were modeled as covariates. Individual-level factors included race, ethnicity, education, household income, health insurance coverage, and geographic region at Wave III. We also assessed whether participants moved states between Waves III and IV (yes vs. no). Further, we included state-level indicators of social disadvantage. The change in state-level median income and the change in state-level proportion of the population under the poverty level (continuous) from Wave III to Wave IV were assessed by calculating the difference between the two waves for each variable (continuous). In addition, we assessed state-level public support for sexual orientation-related nondiscrimination laws using data released by Add Health in 2024. These data were pooled from 41 random national polls in the Roper Center’s iPoll archive conducted with approximately 80,000 respondents between 1999 and 2008. We averaged public support for the four sexual orientation-related nondiscrimination laws that are the focus of this analysis.
Statistical analyses
All analyses were conducted in Stata Version 18 following analytic guidelines for recommended survey weights and complex sampling for Add Health. 54 The percentage of missing data was less than 1% for covariates. Missing data were observed only for race (n = 20) and state-level public support for sexual orientation-related nondiscrimination laws (n = 10). Therefore, we handled missing data using listwise deletion.
All analyses were sex-stratified with exclusively heterosexual participants as the reference group. We calculated means, standard deviations, ranges, and proportions for each variable. We used design-adjusted Rao-Scott Chi-square and Student t-tests to examine sexual orientation differences across study variables. Statistical significance was set at p < 0.05.
Figure 2 presents the hypothesized associations between study variables. We ran linear regression models to examine the association of change in sexual orientation-related nondiscrimination laws from Wave III to Wave IV with 30-year CVD risk at Wave V. Model 1 was unadjusted. Model 2 was adjusted for race, ethnicity, household income, education, health insurance coverage, geographic region, sexual orientation-related nondiscrimination laws at Wave III (baseline), whether participants moved states between Wave III and Wave IV, change in state-level median income, change in state-level proportion of the population under the poverty level, and average state-level public support of sexual orientation-related nondiscrimination laws. To examine whether the association of change in sexual orientation-related nondiscrimination laws with 30-year CVD risk was moderated by sexual orientation, we added an interaction term between sexual orientation and change in sexual orientation-related nondiscrimination laws to Model 2.
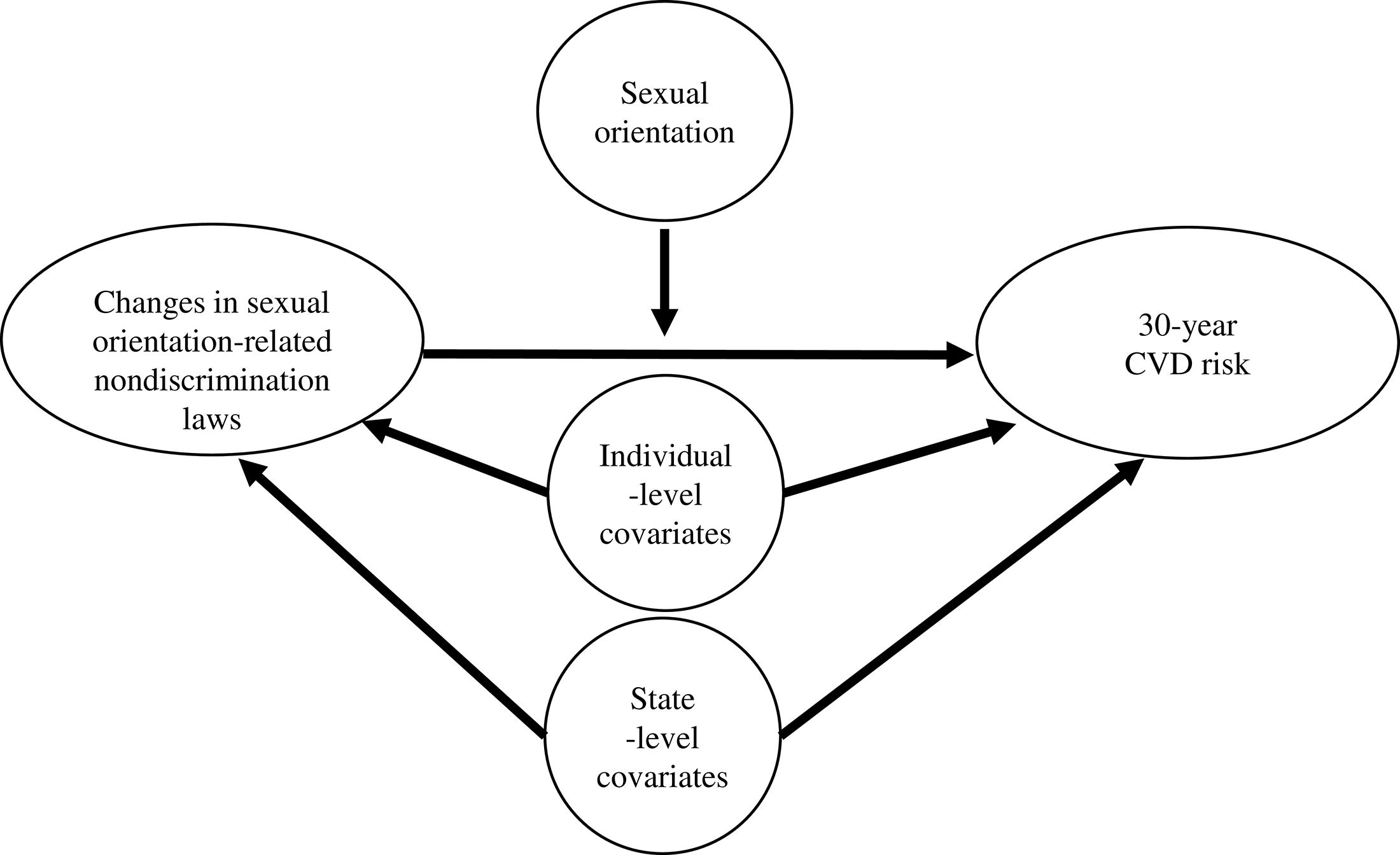
Model of hypothesized associations between study variables. The figure represents the hypothesized associations between changes in sexual orientation-related nondiscrimination laws and 30-year cardiovascular disease risk. Sexual orientation was modeled as a moderator of the association between changes in sexual orientation-related nondiscrimination laws and 30-year cardiovascular disease risk. Individual- and state-level covariates were included to account for potential confounding.
Results
The sample included 3768 participants with a mean age of 28.7 (±1.72) years of whom approximately 77% identified as White, 11% as Hispanic, and 51% as female.
As shown in Table 1, among women, 76.6% were exclusively heterosexual, 18.9% were mostly heterosexual, 2.4% were bisexual, and 2.1% were gay/lesbian. Compared to exclusively heterosexual women, mostly heterosexual women were younger, more likely to identify as White, more likely to have moved states between Wave III and Wave IV, and more likely to experience a decrease in sexual orientation-related nondiscrimination laws. Bisexual women were less likely to identify as White and to have graduated college than exclusively heterosexual women. Compared to exclusively heterosexual women, gay/lesbian women were less likely to have health insurance coverage.
Sexual Orientation Differences across Sample Characteristics Among Women (N = 2273)
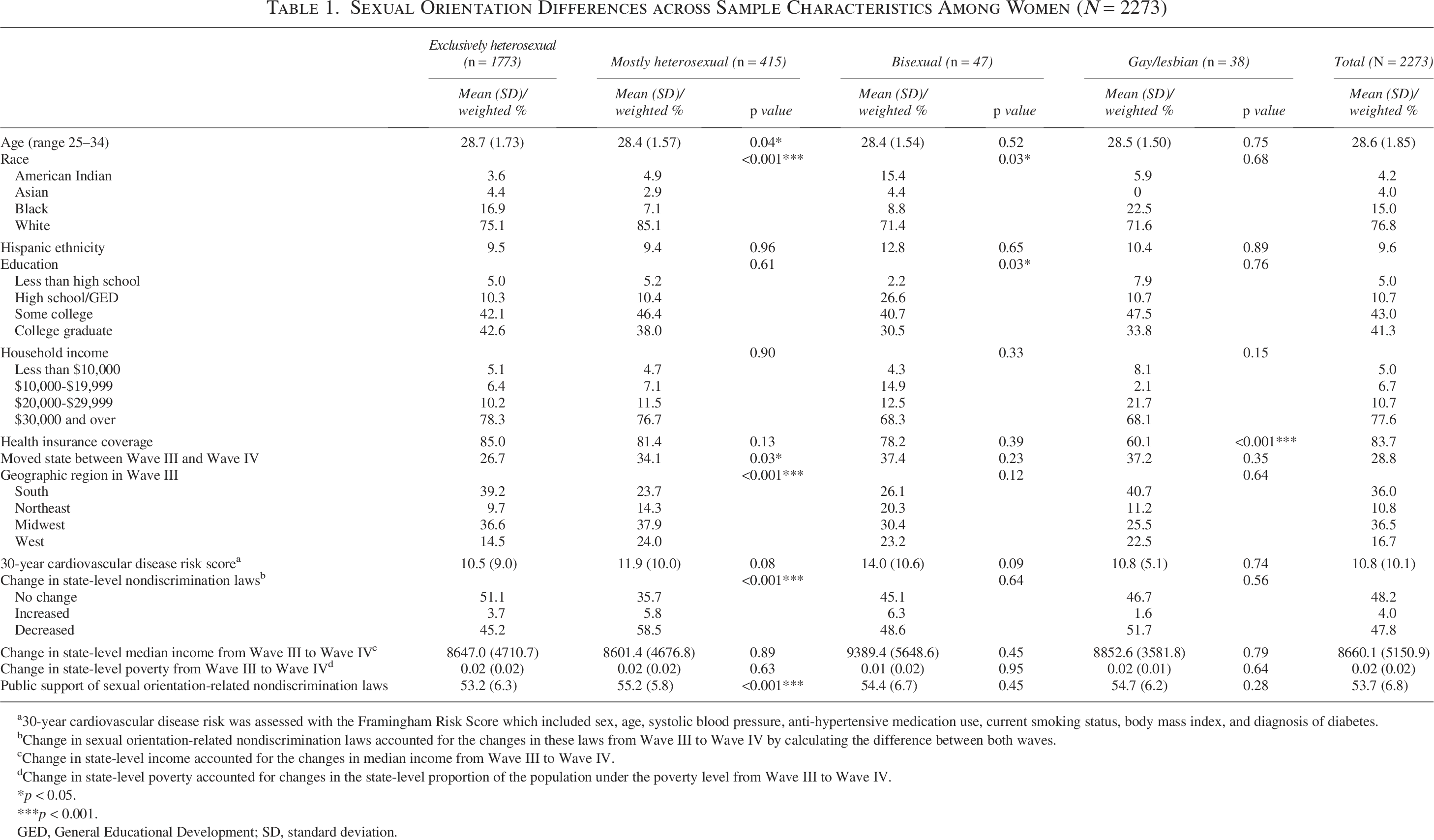
30-year cardiovascular disease risk was assessed with the Framingham Risk Score which included sex, age, systolic blood pressure, anti-hypertensive medication use, current smoking status, body mass index, and diagnosis of diabetes.
Change in sexual orientation-related nondiscrimination laws accounted for the changes in these laws from Wave III to Wave IV by calculating the difference between both waves.
Change in state-level income accounted for the changes in median income from Wave III to Wave IV.
Change in state-level poverty accounted for changes in the state-level proportion of the population under the poverty level from Wave III to Wave IV.
p < 0.05.
p < 0.001.
GED, General Educational Development; SD, standard deviation.
As shown in Table 2, among men, 91.4% were exclusively heterosexual, 4.3% were mostly heterosexual, 1.0% were bisexual, and 3.3% were gay. Compared to exclusively heterosexual men, mostly heterosexual men were more likely to have graduated college and to have experienced a decrease in sexual orientation-related nondiscrimination laws. Mostly heterosexual and bisexual men were less likely than exclusively heterosexual men to report household incomes of $30,000 or more. Bisexual men also had higher 30-year CVD risk compared with exclusively heterosexual men. Gay men were more likely than exclusively heterosexual men to identify as Hispanic.
Sexual Orientation Differences across Sample Characteristics Among Men (N = 1495)
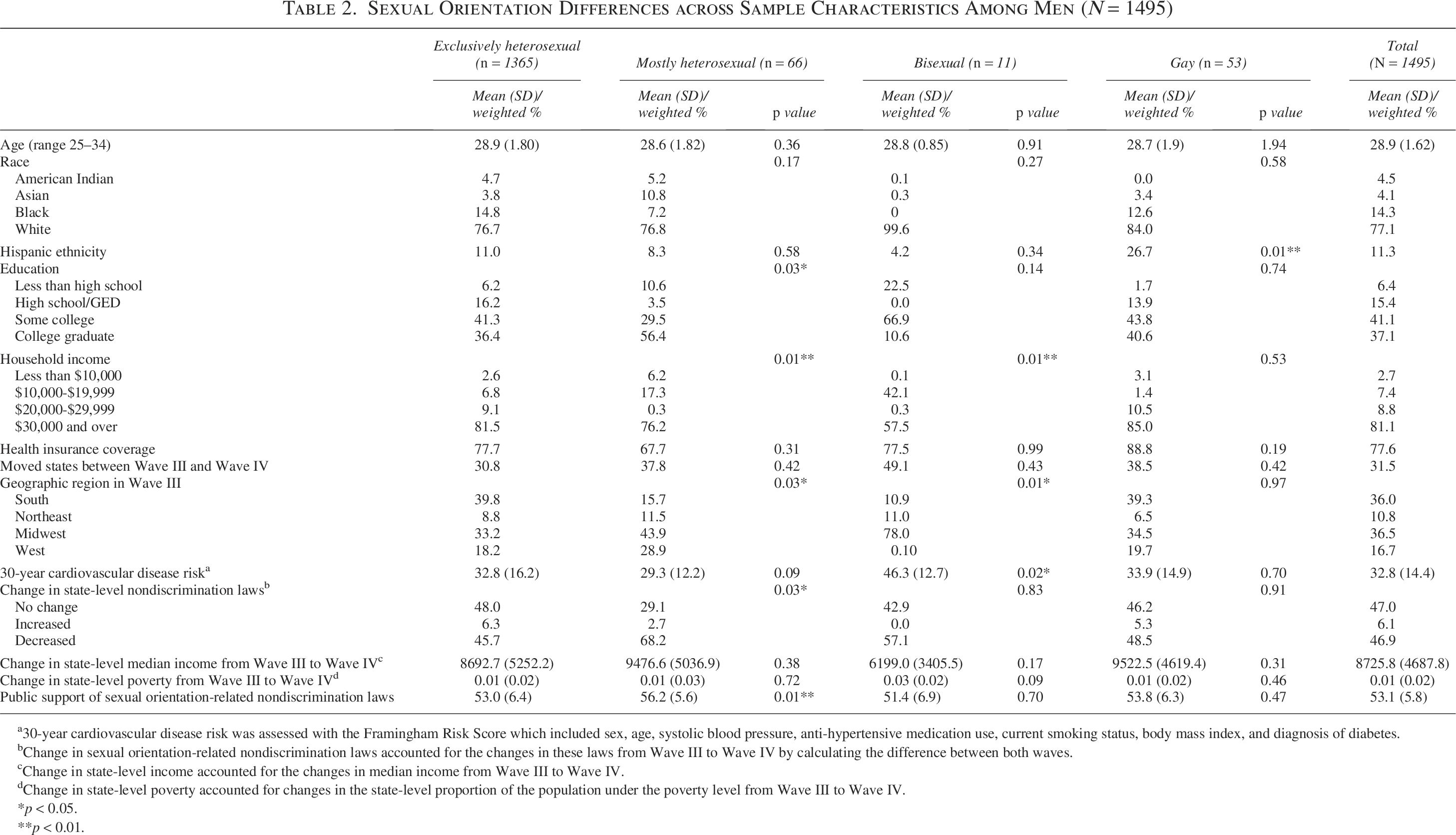
30-year cardiovascular disease risk was assessed with the Framingham Risk Score which included sex, age, systolic blood pressure, anti-hypertensive medication use, current smoking status, body mass index, and diagnosis of diabetes.
Change in sexual orientation-related nondiscrimination laws accounted for the changes in these laws from Wave III to Wave IV by calculating the difference between both waves.
Change in state-level income accounted for the changes in median income from Wave III to Wave IV.
Change in state-level poverty accounted for changes in the state-level proportion of the population under the poverty level from Wave III to Wave IV.
p < 0.05.
p < 0.01.
Table 3 presents the results of multiple linear regression models examining the association of change in sexual orientation-related nondiscrimination laws with 30-year CVD risk in the full sample. In unadjusted models, women (B = −2.31, 95% confidence interval [CI] = −4.52 to −0.11) and men (B = −4.02, 95% CI = −6.71 to −1.34) who experienced an increase in sexual orientation-related nondiscrimination laws had lower 30-year CVD risk. However, these estimates were attenuated after covariate adjustment.
Results of Multiple Linear Regression Models Examining the Association of Change in Sexual Orientation-Related Nondiscrimination Laws with 30-Year Cardiovascular Disease Risk (N = 3768)
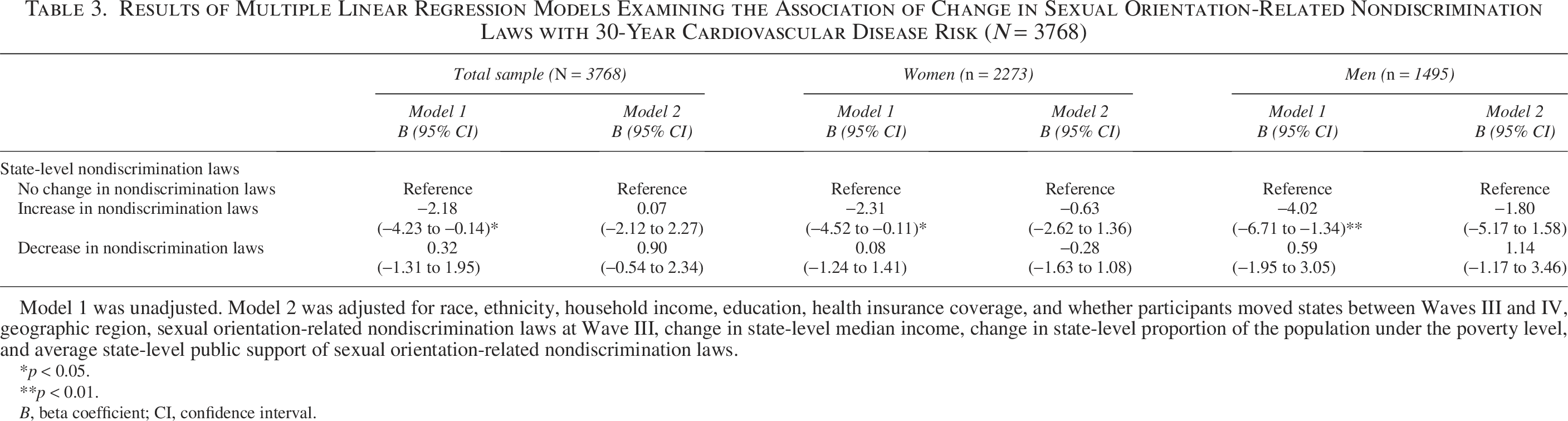
Model 1 was unadjusted. Model 2 was adjusted for race, ethnicity, household income, education, health insurance coverage, and whether participants moved states between Waves III and IV, geographic region, sexual orientation-related nondiscrimination laws at Wave III, change in state-level median income, change in state-level proportion of the population under the poverty level, and average state-level public support of sexual orientation-related nondiscrimination laws.
p < 0.05.
p < 0.01.
B, beta coefficient; CI, confidence interval.
Table 4 presents the results of models examining sexual orientation as a moderator of the association of change in sexual orientation-related nondiscrimination laws with 30-year CVD risk among women. Compared to exclusively heterosexual women, mostly heterosexual women who experienced an increase in sexual orientation-related nondiscrimination laws had lower 30-year CVD risk (B = −5.05, 95% CI = −8.50 to −1.59; p = 0.007).
Results of Multiple Linear Regression Models Examining Sexual Orientation as a Moderator of the Association of Change in Sexual Orientation-Related Nondiscrimination Laws with 30-Year Cardiovascular Disease Risk Among Women (N = 2273)
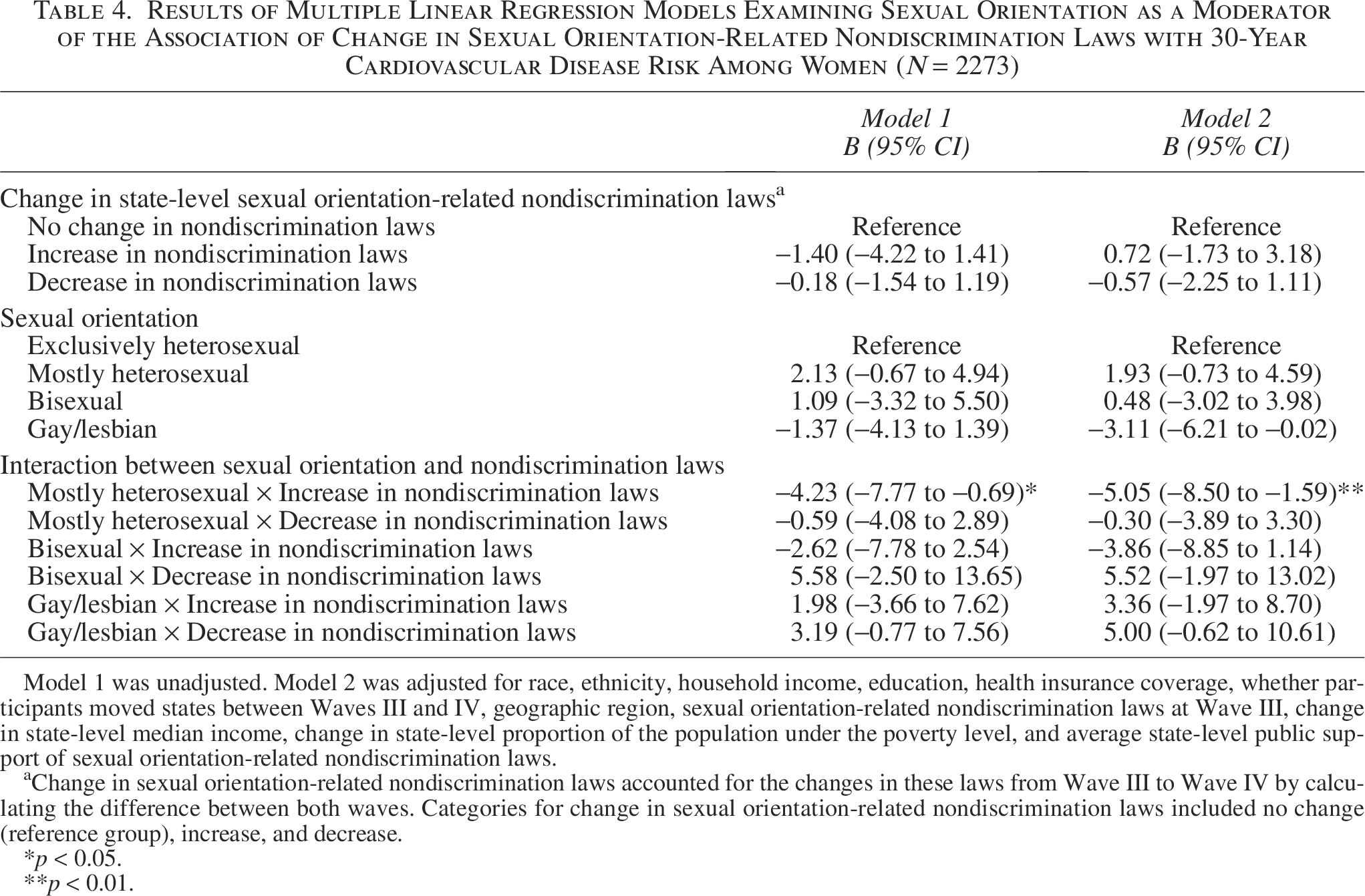
Model 1 was unadjusted. Model 2 was adjusted for race, ethnicity, household income, education, health insurance coverage, whether participants moved states between Waves III and IV, geographic region, sexual orientation-related nondiscrimination laws at Wave III, change in state-level median income, change in state-level proportion of the population under the poverty level, and average state-level public support of sexual orientation-related nondiscrimination laws.
Change in sexual orientation-related nondiscrimination laws accounted for the changes in these laws from Wave III to Wave IV by calculating the difference between both waves. Categories for change in sexual orientation-related nondiscrimination laws included no change (reference group), increase, and decrease.
p < 0.05.
p < 0.01.
Table 5 presents the results of models examining sexual orientation as a moderator of the association of change in sexual orientation-related nondiscrimination laws with 30-year CVD risk among men. Compared to exclusively heterosexual men, gay men who experienced an increase in sexual orientation-related nondiscrimination laws had lower 30-year CVD risk (B = −10.22, 95% CI = −19.05 to −1.39, p = 0.03).
Results of Multiple Linear Regression Models Examining Sexual Orientation as a Moderator of the Association of Change in Sexual Orientation-Related Nondiscrimination Laws with 30-Year Cardiovascular Disease Risk Among Men (N = 1495)
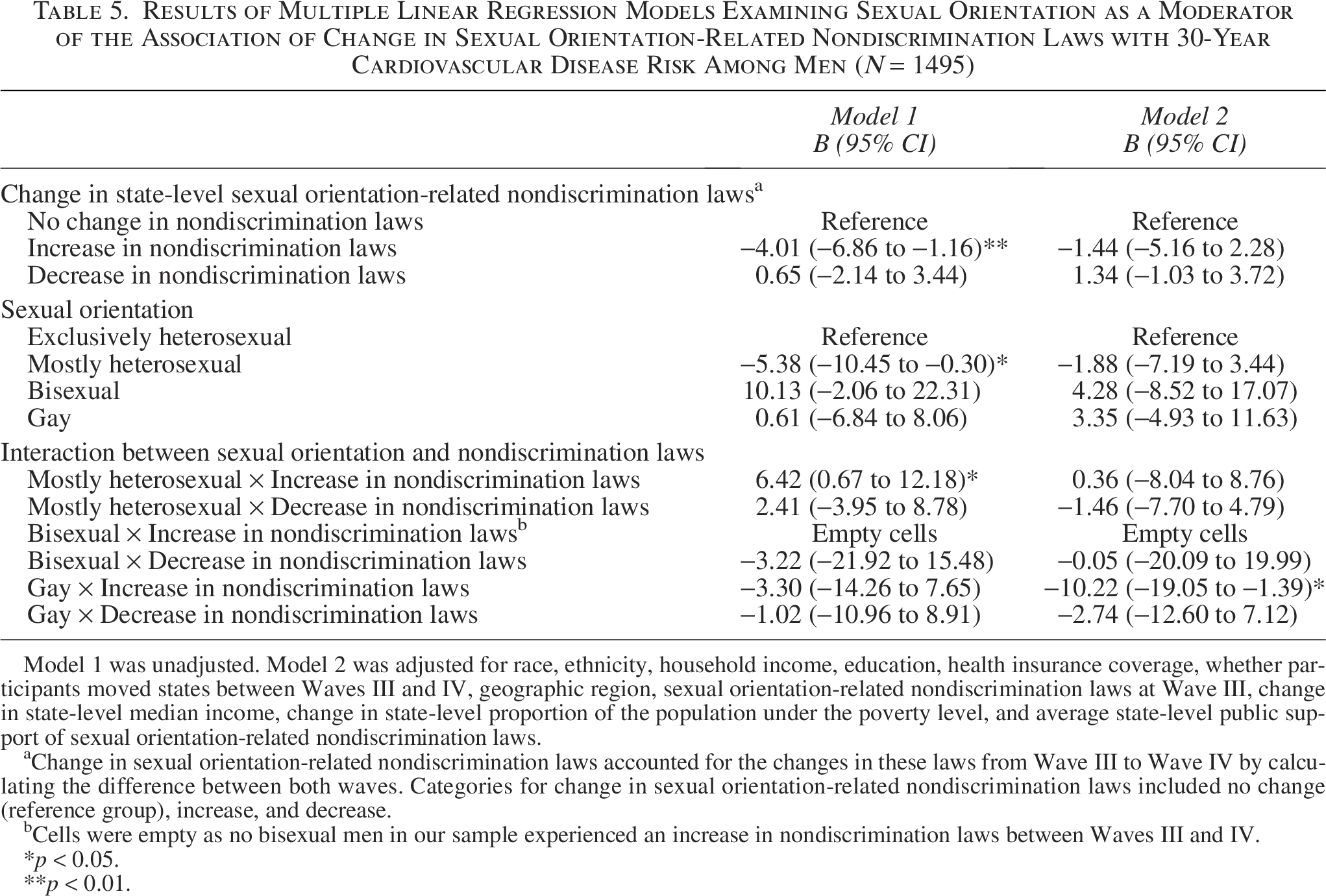
Model 1 was unadjusted. Model 2 was adjusted for race, ethnicity, household income, education, health insurance coverage, whether participants moved states between Waves III and IV, geographic region, sexual orientation-related nondiscrimination laws at Wave III, change in state-level median income, change in state-level proportion of the population under the poverty level, and average state-level public support of sexual orientation-related nondiscrimination laws.
Change in sexual orientation-related nondiscrimination laws accounted for the changes in these laws from Wave III to Wave IV by calculating the difference between both waves. Categories for change in sexual orientation-related nondiscrimination laws included no change (reference group), increase, and decrease.
Cells were empty as no bisexual men in our sample experienced an increase in nondiscrimination laws between Waves III and IV.
p < 0.05.
p < 0.01.
Figure 3 presents margins plots illustrating the influence of the interaction between sexual orientation and changes in sexual orientation-related nondiscrimination laws on 30-year CVD risk. Consistent with Tables 4 and 5, Figure 3 shows that mostly heterosexual and bisexual women who experienced an increase in sexual orientation-related nondiscrimination laws had lower 30-year CVD risk. However, this was only significant for mostly heterosexual women, as the confidence intervals for increased, decreased, and no change in sexual orientation-related nondiscrimination laws overlapped for bisexual women. Among men, gay men who experienced an increase in sexual orientation-related nondiscrimination laws had lower 30-year CVD risk. No bisexual men in our sample experienced an increase in sexual orientation-related nondiscrimination laws. There were no other sexual orientation differences.
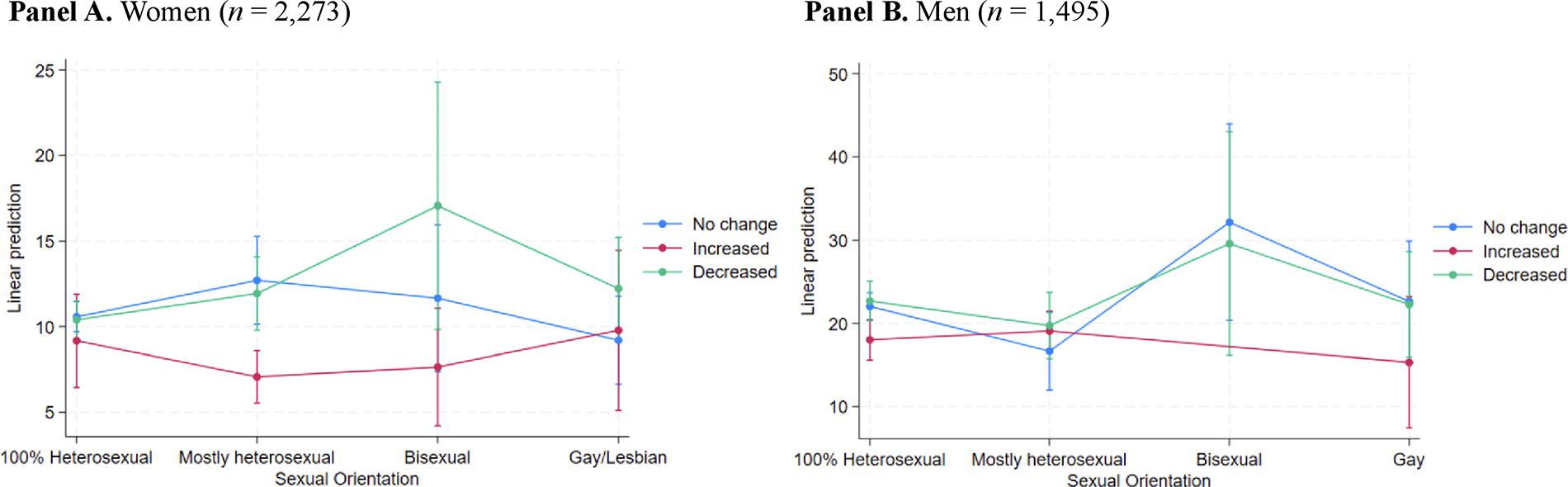
Margins plots of the influence of the interaction between sexual orientation and change in sexual orientation-related nondiscrimination laws on 30-year cardiovascular disease risk. Panel
As our independent variable (i.e., change in sexual orientation-related nondiscrimination laws) captures both changes in a state’s legal environment as well as whether participants moved to a state that had similar, increased, or decreased nondiscrimination laws, we conducted sensitivity analyses to assess whether moving states between Waves III and IV affected our results. As shown in Supplementary Tables S1 and S2, there were no sexual orientation differences in the associations of changes in sexual orientation-based nondiscrimination laws with 30-year CVD risk based on whether or not participants moved states between Waves III and IV.
Discussion
We used nationally representative data from Add Health to examine the association of change in sexual orientation-related nondiscrimination laws with 30-year CVD risk among LGB and heterosexual adults. Our hypotheses were partially supported. Increases in sexual orientation-related nondiscrimination laws were associated with lower 30-year CVD risk among mostly heterosexual women and gay men, but not for other LGB subgroups.
Our findings are generally consistent with prior work on structural stigma and health outcomes in this population.33,42 Using Add Health data, investigators found that a higher number of sexual orientation-related nondiscrimination laws was associated with a lower risk of maternal hypertension among LGB women. 42 Our results are also consistent with the 35 U.S.-based studies included in the aforementioned review that found state-level discriminatory policies were associated with adverse health outcomes among LGB individuals, including CVD-related outcomes (e.g., tobacco use). 33
Increases in sexual orientation-related nondiscrimination laws appear to have a protective effect on CVD risk among mostly heterosexual women and gay men. This underscores the importance of enhancing and enforcing sexual orientation-related nondiscrimination laws. However, simply enacting nondiscrimination laws does not guarantee their implementation. Thus, policy changes must be accompanied by individual- and interpersonal-level interventions to address CVD risk among LGB individuals. There is a need to establish processes to enforce these legal protections. Efforts such as public education campaigns can also increase awareness of the protective effects of nondiscrimination laws. Our findings highlight the need for comprehensive upstream changes combined with downstream efforts across multiple levels to ensure that nondiscrimination laws have a beneficial impact on the cardiovascular health of LGB individuals.
These findings have important practice, research, and policy implications. Given the impact of structural stigma on CVD risk among LGB individuals, clinicians need to be educated about these disparities and trained to provide culturally competent care. Clinicians should also advocate for nondiscrimination policies, not just at the state level but also within their healthcare organizations. Although Add Health is one of the few nationally representative datasets that includes sexual orientation, cardiovascular health, and sexual orientation-related nondiscrimination law data, it is limited by the number and types of state-level nondiscrimination laws assessed. Although our study focused on state-level laws, future research should examine other indicators of structural stigma at the local and federal levels (e.g., religious exemption laws) to provide a comprehensive understanding of how structural stigma affects the cardiovascular health of LGB individuals. The findings also underscore the need for structural-level interventions to promote the cardiovascular health of LGB adults. Structural-level determinants must be considered when developing strategies for CVD risk reduction among LGB adults.
Changes in sexual orientation-related nondiscrimination laws were not associated with 30-year CVD risk among other LGB subgroups. It is likely that mostly heterosexual men benefit from support systems similar to those of exclusively heterosexual men, including greater access to healthcare and employment opportunities. Although evidence on CVD risk among mostly heterosexual individuals is limited, mostly heterosexual individuals—particularly mostly heterosexual men—view themselves as closer to the exclusively heterosexual community than to the LGB community and predominantly socialize with exclusively heterosexual individuals.55,56 It is possible that mostly heterosexual men, who face less gender- and sexual orientation-related discrimination, are less susceptible to the deleterious effects of less protective sexual orientation-related nondiscrimination laws.
In contrast, mostly heterosexual women may be more vulnerable to structural stigma due to exposure to gender-based stressors. Investigators have found that discrimination is widely experienced by women, particularly LGB women.57,58 The intersection of these minoritized identities may compound the impact of structural stigma among mostly heterosexual women. Cisgender men may also be less likely to identify with gay or bisexual labels despite engaging in same-sex behavior or experiencing same-sex attraction, potentially due to prevailing norms around masculinity.59,60 This distancing from LGB identities may reduce both visibility and exposure to sexual orientation-related discrimination. Together, these gender differences may help explain why mostly heterosexual women—but not men—had lower CVD risk due to experiencing increases in nondiscrimination laws. However, more research is needed to better understand the complex factors that may contribute to differences in CVD risk between mostly heterosexual men and women. 6
It is unclear why findings were null for gay/lesbian women, bisexual women, and bisexual men; however, it is likely attributed to small sample sizes. Future research should replicate our analyses in larger samples of LGB adults to determine if these associations are consistent across different LGB subgroups. Although our sample had similar racial, ethnic, and gender distribution to other population-based studies on CVD risk among LGB individuals,11,15,61,62 there is growing evidence that Black and Hispanic LGB adults have higher CVD risk than their heterosexual and White LGB counterparts.15,63–65 Replication of our analyses with larger, more diverse samples of LGB adults will permit comprehensive examination of LGB subgroups who remain underrepresented within CVD research, such as LGB people of color and older adults.
Strengths
First, the longitudinal design of Add Health allowed us to examine the impact of changes in sexual orientation-related nondiscrimination laws on CVD risk among LGB and heterosexual adults. Second, the use of objective measures to assess the CVD risk using the FRS strengthens the study’s findings, particularly because most research on CVD risk among LGB adults has relied on self-reported data, 6 which is prone to recall and social desirability bias. Third, Add Health’s nationally representative sample enhances generalizability of our findings.
Limitations
First, we were unable to examine laws related to gender identity that specifically impact transgender and gender diverse individuals because these data were not available in Add Health. This is an important area for future research. Second, the available measure of gender/sex in Add Health Wave III was binary and likely conflated sex assigned at birth with gender identity. Lastly, there are additional confounders that were not accounted for, such as additional minority stressors (e.g., internalized homonegativity, family rejection), which are not included in Add Health but that may influence CVD risk among LGB adults.
Conclusion
In this population-based study, we found that changes in sexual orientation-related nondiscrimination laws were associated with 30-year CVD risk among certain groups of LGB adults. These findings suggest that state laws that protect LGB people from sexual orientation-based discrimination might play an important role in promoting their cardiovascular health. The results highlight the need for structural-level interventions to reduce CVD risk among LGB adults.
Authors’ Contributions
M.P., B.E., and B.A.C.: Conceptualization, funding acquisition, writing—original draft and reviewing. Y.S., A.B., L.P., and B.A.C.: Formal analysis. Y.S., M.P., B.E., C.D., D.D., L.P., and L.B.B.: Writing—review and editing.
Footnotes
Author Disclosure Statement
Dr. Caceres is a member of the Editorial Board of LGBT Health. No competing financial or other interests exist for any of the other authors.
Funding Information
This work was supported by grants from the National Heart, Lung, and Blood Institute (K01HL146965; R56HL168489; R01HL168489) to B.A.C. Y.S. was supported by a predoctoral research fellowship from the American Heart Association (899585). This research uses data from Add Health, funded by grant P01HD31921 from the Eunice Kennedy Shriver National Institute of Child Health and Human Development, with cooperative funding from 23 other federal agencies and foundations. Add Health is currently funded by the National Institute on Aging cooperative agreements U01AG071448 (Hummer) and U01AG071450 (Aiello and Hummer) at the University of North Carolina at Chapel Hill.
Disclaimer
The funders had no role in the study analysis, decision to publish the study, or the preparation of the article.