
Abstract
Abstract
Background:
Lymphedema of hand after breast cancer treatment causes significant loss of hand function. Although there are several ways of assessing limb volume, measuring hand volume has been problematic due to technical difficulties associated with assessment of finger volumes. The aim of this study was to investigate the criterion validity and reliability of Perometer™ for measuring hand volume in woman with and without lymphedema.
Methods and Results:
Hand volume of forty women with (n = 20) and without lymphedema (n = 20) was assessed twice by one rater and once by another rater using the Perometer, and once by one rater using the water volumetry method. Intra- and inter-rater reliability was determined from the intraclass correlation coefficients and Percent Close Agreement. Agreement between the Perometer and water volumetry was determined using a limit of agreement and Lin's concordance correlation. The Perometer had high intra [ICC2,1 = 0.989 (95% CI: 0.98–0.99)] and inter-rater reliability [ICC2,1 = 0.993 (95% CI: 0.99–1.0)]. Percent close agreement revealed that 80% of the measures were within 9 ml for inter-rater reliability and within 15 ml for intra-rater reliability. In addition, there was high concordance between hand volumes obtained with the Perometer and water volumetry method (Rc = 0.88). However, the Perometer overestimated the volume of hand compared to water volumetry method (bias: 7.5%).
Conclusions:
The Perometer can be used with high reliability to measure hand volume but caution should be exercised when data are compared with measures derived from the water volumetry method.
Introduction
The main clinical methods for measuring hand volume are water displacement (volumetric) measurements and figure-of-eight circumferential measurements. 3 Water displacement measurement is currently considered to be the “gold standard” for the direct measurement of hand and wrist lymphedema. 4 Previous studies have established that water displacement volumetrics have an ‘error of method’ of less than 1% for measurements of hand volumes.4,5 Although the water displacement method is the criterion reference for measuring volume, it can be a time consuming process that can be technically demanding. To ensure reliability, the volumeter must be placed on an even surface, the water temperature standardized between occasions (i.e., 32°C), 4 and adequate time allowed for water to finish dripping from the volumeter after limb immersion. 6 Alternative indirect methods of volume estimation, such as standardized arm circumferences taken at regular intervals along the limb using a tape measure, may be difficult for hand lymphedema because reference bony landmarks may be unidentifiable in edematous hands and wrists. In addition, this method of hand volume cannot include finger volume.
Recently, measurement of volume using the Perometer has been proposed as a simple and quick alternative method for measuring limb volume. The Perometer is an optoelectrical imaging device that has been designed specifically for measuring limb volume, circumference, contour, and cross sectional area. 7 The Perometer consists of a moveable frame that can scan a limb segment within a matter of seconds and can be safely used for people with open wounds or skin infections. The Perometer has been found to be an accurate, convenient, and highly reliable for the measurement of arm volume;8,9 however, the suitability of the Perometer for measurements of hand volume has not been established.
The aim of this study was to investigate the criterion validity and reliability of the Perometer for measuring hand volume using samples of asymptomatic and symptomatic participants.
Materials and Methods
Design
This within-session study consisted of a test-retest protocol to determine the inter- and intrareliability for measurement of the hand volume using the Perometer. In addition, it assessed the validity of perometry hand volume measurements by comparing them to those from water displacement. The water displacement method was used as the criterion reference since high reliability, accuracy, and responsiveness to volume change for the method had been established. 4 The Human Ethics Committee of the University of Sydney approved the study, and informed consent was obtained from each participant prior to testing.
Participants
Women with (n = 20) and without hand lymphedema (n = 20) were recruited for the study through advertisements around the University campus and participants from other studies. Women with unilateral lymphedema after breast cancer treatment had been diagnosed as having lymphedema by a health care practitioner. Exclusion criteria were the presence of any of the following: skin conditions or open wounds below the elbow, or absence of any part of a digit from previous amputation.
The average age of women was 56 ± 12 years (Table 1). Thirty-six women were right-handed and 12 women had right-side lymphedema. The average length of time since diagnosis of lymphedema was 6.5 ± 7.0 years.
Protocol
Women attended the laboratory on a single session. The lymphedematous arm was measured in the women with lymphedema whereas the dominant limb was measured in the women without lymphedema. Each woman's affected/dominant arm was measured with the Perometer twice by one rater and once by a second rater. The affected/dominant arm was also measured once with the water volumeter. The order of these four measurements was randomized prior to the commencement of data collection by another researcher. Women who wore compression garments were asked to remove them 2 hours prior to attending the laboratory to allow their lymphedema to stabilize.
To standardize the distance over which volume was calculated for both methods, the distance between the tip of the middle finger to the distal palmar crease was determined.
Measurements
Perometry
Hand volume was measured using an optoelectrical perometer (Perometer 350S, Juzo, Wuppertal, Germany). The participants were positioned sitting with their arm in 90° abduction, palm down, and their middle finger touching the tip of metal plate on the hand rest (Fig. 1). Participants held their digits extended while keeping the thumb adjacent to the index finger. During the measurement, the Perometer frame, which was initially positioned behind the hand rest, moved slowly toward the shoulder before returning to the starting position.
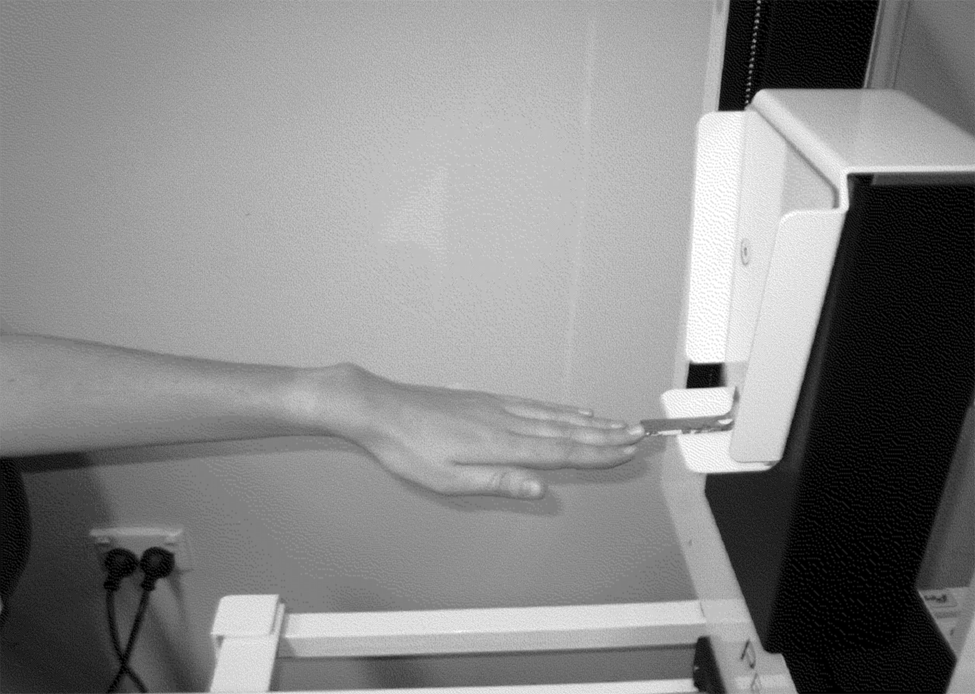
Perometry. Position of the hand during a Perometer measurement.
Water volumetry
A purpose-built hand volumeter was used to assess hand volume (Fig. 2a, Vinidex Tubemakers Pty Ltd, Melbourne, Victoria). A spout on one side of the volumeter channeled overflow water into a purpose-built measuring cylinder. Depth regulators were placed in the bottom of the volumeter during measurements to standardize the segment of hand measured for each participant (Fig. 2b). The distance between the discs could be adjusted and set for each participant, so that the segment of hand that was immersed was always standardized to be only to the level of the distal palmar crease. The accuracy, reliability, and responsiveness of the purpose-built measuring cylinder (Fig. 2a) has been previously established. 4
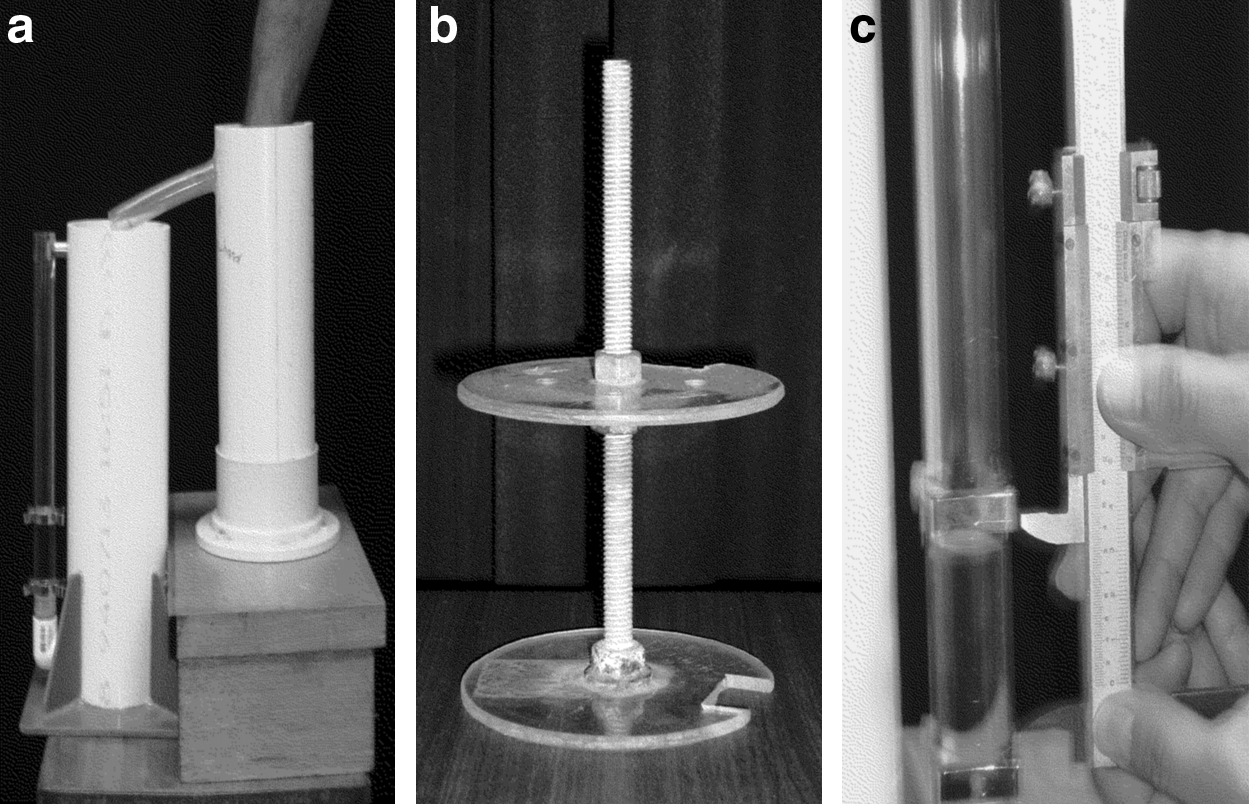
Water volumetry.
The regulator was placed in the bottom of the volumeter and the measuring cylinder was placed underneath the overflow spout. The volumeter was then filled with water that had been warmed to 32°Celsius (±1°). A small volume of water was then poured into the measuring cylinder until the meniscus rose to a visible level at the bottom of the manometer tube. The lower clamp was then set to level 1 to zero the instrument. The participant then lowered the experimental hand into the volumeter until the tip of the middle finger touched the top of the threaded rod. The participant then continued to immerse the hand while maintaining contact against the threaded rod with the palmar aspect of the middle finger. When the fingertip touched the upper disc of the regulator, the participant was instructed to remain still until water had ceased dripping from the volumeter. The arm was withdrawn, the observer aligned the clamp on the measuring cylinder to level 2, and then measured and recorded the distance between levels 1 and 2 with the vernier calipers in millimeters (Fig. 2c). The conversion factor for millimeters to milliliters is 1 mm of vertical displacement = 8.78 ml of volume. 4
Data analyses
Descriptive statistics were calculated for measurements taken for each sample for each tester as well as for pooled data.
Reliability of Perometer
Intraclass Correlation Coefficients (ICC2,1) with 95% confidence intervals and Percent Close Agreement (PCA) were used to determine intra-rater and inter-rater reliability of hand volume measurements determined with perometry. Paired t tests were also performed to determine whether there was a difference between means of test-retest data. Reliability was considered poor when the ICC2,1 was <0.40, moderate between 0.40 and 0.75, substantial between 0.75 and 0.90, and excellent when >0.90. 10
Agreement between Perometer and water volumeter measurements
A limit of agreement analysis 11 and Lin's concordance correlation 12 were used to evaluate the relationship between measurements taken with the Perometer and with water volumetry using the first value for hand volume obtained with the Perometer method.
Statistical analyses were conducted with SPSS 16 for Windows (version 16, SPSS, Chicago) and significance was set at α = 0.05.
Results
Reliability
Measurements using the Perometer demonstrated excellent inter- and intra-rater reliability. The difference in volume between two raters was 6.6 ± 4.4 ml and between the two measurements by Rater 1 was 7.7 ± 6.9 ml. The intra-rater ICC2,1 was 0.989 (95% CI: 0.979–0.994) and inter-rater ICC2,1 was 0.993 (0.986–0.996) (Table 2). Paired t-tests showed that there were no significant differences in hand volume between the measurements undertaken by different raters and between the two measurements undertaken by Rater 1 (Table 2). PCA showed that there was less than 9 ml difference in hand volume for 80% of the measurements undertaken by two raters and 73% of the measurements undertaken by a single rater (Fig. 3).
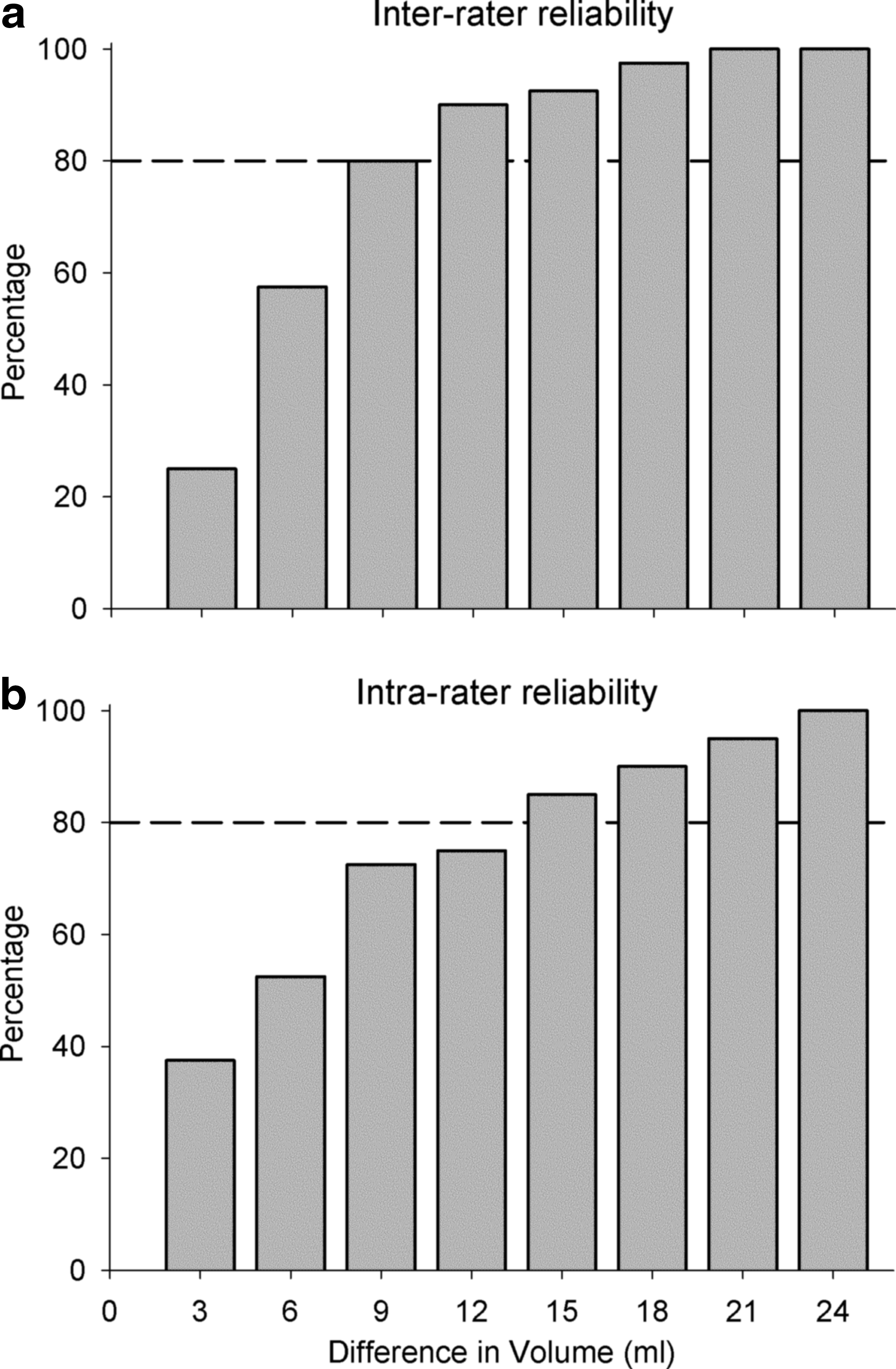
Percent close agreement between raters and between measurements by the same rater. Graph
Agreement
There was a strong concordance between Perometer hand volume measures and those undertaken with water volumetry (rc = 0.88). Comparison of the volumes derived from two methods, using limits of agreement analysis (Table 3), revealed that the Perometer tended to overestimate the volume of hand obtained from water volumetry (bias: 7.5%; Fig. 4).
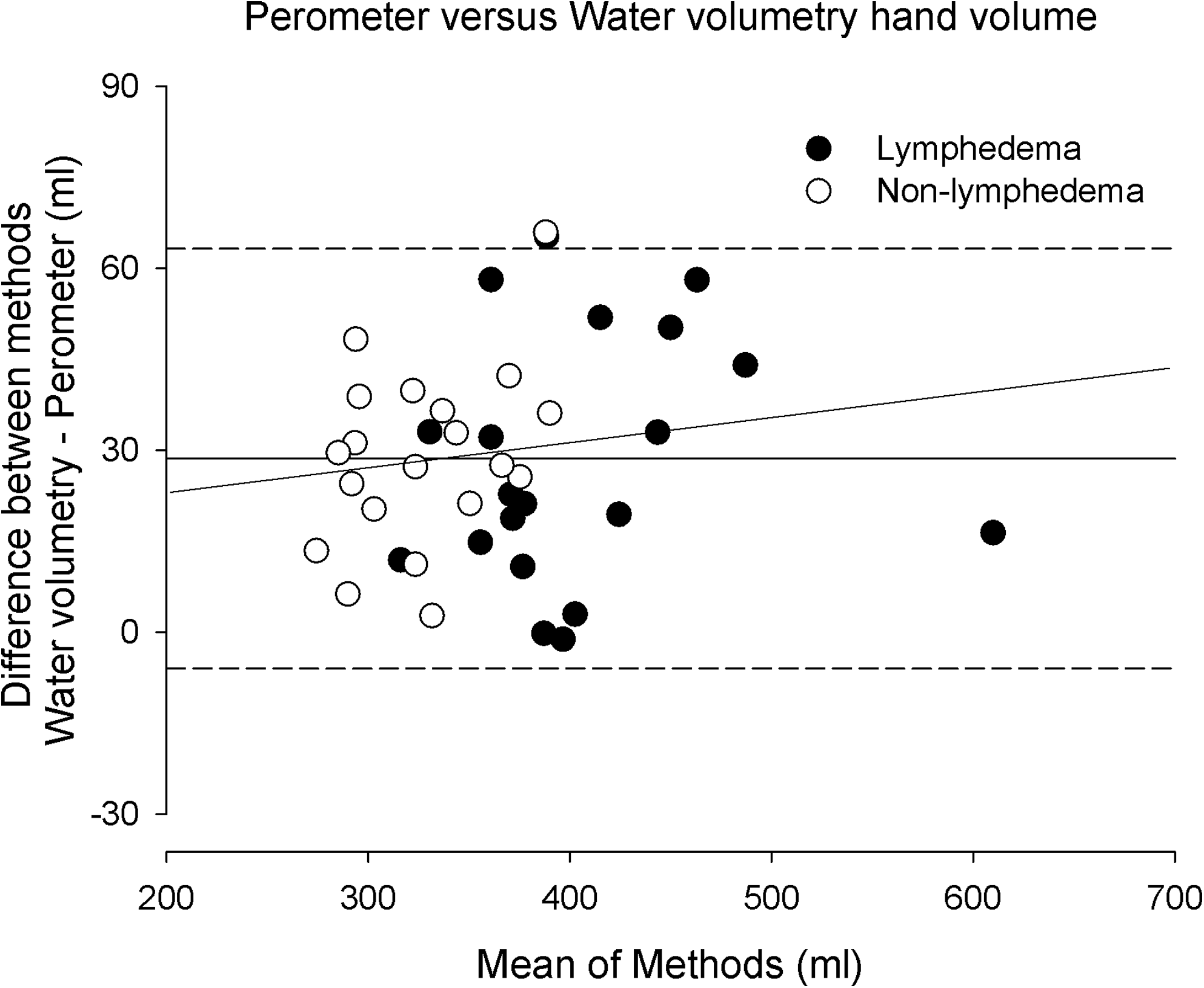
Bland and Altman plot shows the average of hand volumes from Perometry and water volumetry against the difference between the two measurements. The positive direction of difference between the two measurements in hand volumes indicates Perometer values overestimate hand volumes compared to water volumetry method. The solid line represents the mean, and the short dashed lines represent 1.96 times the standard deviation of the difference between the two measures. The long dashed line represents the regression of the mean of the methods on the difference between methods.
Discussion
The aim of the study was to investigate the reliability and criterion validity of the Perometer for measuring hand volume using samples of asymptomatic and symptomatic participants. The current data indicate that hand volume can be measured with high reliability using the Perometer. Further, there was strong agreement between measurements taken with the Perometer and using the gold standard water displacement method. The difference between measurements taken with the two methods may be attributed to a technical issue associated with hand volume measurements using the Perometer that can be accounted for when interpreting measurements taken with the Perometer. Thus, the Perometer appears to offer an alternative to water displacement method for measuring arm volume in the presence of lymphedema in both the clinic and research environments.
Although our method for assessment of hand volume with the Perometer was highly reliable, there was a mean volume difference of up to 24 ml volume differences between methods that equated to a difference of approximately 6% of volumes taken. Hand volumes determined by the Perometer were systematically higher than those determined by the water displacement methods. Such overestimation may simply reflect that the Perometer detected the interdigital spaces as tissue volume. In an attempt to correct for this, subjects were instructed to hold their digits tightly together that included the thumb against the index finger; however, such positioning did not eliminate all potential spaces and the Perometer detected the digits and hand as an elliptical object, and calculated air spaces between the digits as tissue volume. Previous studies have also highlighted the effect on the accuracy of the volume measurement of incorrect positioning of a limb within the Perometer device.7,13–15 For example, Man et al. 15 showed that the angle of the knee joint could affect the volume determined by the Perometer by up to 11%. Therefore, while we recommend that the patient hold the fingers and thumb approximated during measurements using the Perometer, some volume overestimation may be inherent to the method.
While there may be an overestimation bias associated with the Perometer, there remain several advantages associated with using the Perometer to evaluate hand lymphedema compared to the water displacement method. First, it is convenient and quick, conferring a significant advantage for the clinician over water displacement methods. This is a product of: (i) the reduced set-up time for Perometry, which does not require stabilization of water temperature, calibration of a water level meniscus, 4 or cleaning of the volumeter for hygiene; (ii) shorter measurement time, which is prolonged for water volumetry because of the duration that must be allowed for water to cease dripping from the volumeter. Second, excellent inter- and intra-rater reliability for Perometry means that a patient does not need to be evaluated by the same therapist between or within sessions, as long as the standardized protocol is followed. This is a significant advantage for chronic conditions in which patients may be followed for years after surgery. Finally, the Perometer can be used even in the presence of infections or other skin conditions contraindicated for measurement using the water displacement method when water-borne infection may be a risk.
A potential disadvantage of the Perometer method is that it is not interchangeable with the water displacement method because of the issue of the volume overestimation. A pragmatic solution may be to use the Perometer for day-to-day or week-to-week measurements in the clinic to reliably assess for effects of treatment or disease progress. If highly accurate measurements are required, then month-to-month or even longer duration measurements can be taken with the water displacement method. Such practice is similar to how a clinician may use serial circumferential tape measurements to estimate changes within a limb segment over time; however, tape measurements would only provide an analogue measure of overall limb volume. Alternatively, given that the bias is systematic using the Perometer and that the method is reliable, the clinician or researcher may choose to ignore the overestimation bias if the aim of measurement is to assess for intervention effects.
Conclusion
The Perometer may be used to determine volumes of hand with and without lymphedema with high reliability and acceptable validity. However, clinicians and researchers would need to standardize measurements and careful positioning of fingers and hand to reduce the measurement bias. If such issues are acknowledged, the Perometer is a useful alternative to the water displacement method for measurements of hand volume. Future research is required to describe the significant clinical changes in hand volume.
Footnotes
Acknowledgments
This research was supported by a grant from the RT Hall Foundation and the National Breast Cancer Foundation, Australia.
Author Disclosure Statement
No competing financial interests exist.