
Abstract
Abstract
Background:
The head and neck region is the most common site for lymphatic malformations. The aim of the present study was to analyze the exact localizations of lymphatic malformations of the neck.
Methods and Results:
The patients' charts of 48 patients with lymphatic malformations of the neck were retrospectively analyzed regarding gender, age at diagnosis, age at initial presentation, morphologic type, size, and localization. The median age of the patients at presentation was 11.9 years. Macrocystic malformations were observed in 13 patients (27%), mainly in the lateral neck. Microcystic lesions occurred in 22 patients (46%), predominantly in the floor of mouth. Mixed lymphatic malformations occurred in 13 patients (27%) without a preferred localization. The morbidity of patients with microcystic and mixed lesions was higher than of patients with macrocystic lymphatic malformations.
Conclusion:
The cause for the different localization of microcystic and macrocystic lymphatic malformations is still not clarified. One reason may is the different structure of the surrounding connective tissue, which is compact in the floor of mouth and loose in the neck lateral neck so that macrocystic cysts can arise. Maybe both types of malformation have a different etiology. However, this will have to be clarified in further studies.
Introduction
Lymphatic malformations are typically present at birth, but some only become manifest at a later stage. They grow proportional to the patients' body growth but may be subject to further enlargement in life, particularly due to infection and trauma or during puberty and pregnancy. The incidence of lymphatic malformations is estimated to 1.2–2.8 lymphatic malformations per 1000 births 4 and 2.8 patients per 100,000 hospital admissions. 5
The majority of lymphatic malformations occur in the head and neck region. 6 Less often, they can involve the trunk and extremities. Kennedy 7 supposed that the complexity of the cervical lymphatic system is a possible explanation for the fact that the head and neck region is the most common site for lymphatic malformations.
The treatment of lymphatic malformations of the neck depends on the morphologic type and on the exact localization. It is often challenging due to the density of important structures in the neck area. Therefore, the aim of the present study was to analyze the localizations of lymphatic malformations of the neck.
Methods
From July 1997 to May 2010, 761 patients with vascular anomalies presented at the Department of Otolaryngology, Head, and Neck Surgery. Of these, 48 had lymphatic malformations of the neck. The charts of these patients were retrospectively analyzed regarding gender, age at diagnosis, age at initial presentation, morphologic type, size, localization, the Cologne Disease Score, 8 and the classification according to de Serres et al. 9 The Cologne Disease Score is a clinical staging system for patients with lymphatic malformations of the head and neck on the basis of five morbidity items (disfigurement, dysphagia, dysphonia, dyspnea, and an observer statement towards progression). 8 The morbidity items were assessed with zero, one or two points, a maximum score of ten points can be reached in case of five normal parameters. The classification of de Serres et al. 9 differentiates lymphatic malformations in five stages according to their localization in the neck. In stage I, the spread is unilateral infrahyoidal, in stage II suprahyoidal unilateral, stage III lesions are located unilateral supra- and infrahyoidal, stage IV lesions bilateral suprahyoidal, and stage V lesions bilateral supra- and infrahyoidal. MR and ultrasound images were evaluated to analyze the size and localization of the lymphatic malformations.
Results
In all, 48 patients with lymphatic malformations of the neck were analyzed. The male to female ratio was 1:1. The average age at first diagnosis of lymphatic malformation was 4.5 years. In 4 patients (8.3%), the lymphatic malformation was recognized prenatally, in 26 children (54.2%) at birth, in 6 patients (12.5%) up to the age of 2 years, and in 5 patients (10.4%) until the age of 10. The age of the oldest patient at diagnosis was 43 years. At the time of initial presentation to the Department of Otolaryngology, the median age of patients was 11.94 years. Twenty-nine patients (60%) had been treated at other hospitals before presenting at our department. The symptoms at presentation ranged from swelling, pain, recurrent bleeding (especially in tongue involvement), malocclusion, macroglossia, and dysphagia to life-threatening dyspnea. A sonography was carried out in all patients, in 42/48 patients additional MRI was performed. In 22 patients (45%), the lymphatic malformations were located on the left side of the neck, in 13 (27%), on the right side, and in 13 cases (27%) on both sides of the neck.
According to classification of de Serres, 9 the patients could be divided into the following groups: 5 patients (10.4%) had stage I, 15 (31.3%) stage II, 11 (22.9%) stage III, 5 (10.4%) stage IV, and 12 (25.0%) stage V.
Lymphatic malformations were divided into macrocystic, microcystic, and mixed lesions. Macrocystic malformations were observed in 13 patients (27%), of which 4 cases were located on the right and 9 on the left side of the neck, mainly in the lateral neck. Microcystic lesions occurred in 22 patients (46%), including 8 cases on the right, 7 on the left, and 7 on both sides of the neck. The predominant localization was the floor of mouth. Mixed lymphatic malformations occurred in 13 patients (27%). They were localized in 2 patients on the right, in 6 patients on the left, and in 5 patients on both sides of the neck. In all, mixed lymphatic malformations were bigger in size than microcystic and macrocystic lymphatic malformations. Figure 1 shows the localization of lymphatic malformations as a function of morphological type. All patients were additionally classified according to the Cologne Disease Score. 8 Patients with macrocystic malformations scored on average better than patients with microcystic and mixed lymphatic malformations. Therefore, patients with macrocystic malformations belonged to the moderate disease group (>8 points) according to Wittekindt et al., 8 while all patients with advanced (5–7 points) and severe disease (<4 points) had microcystic or mixed lymphatic malformations (Fig. 2).

Localization of macrocystic
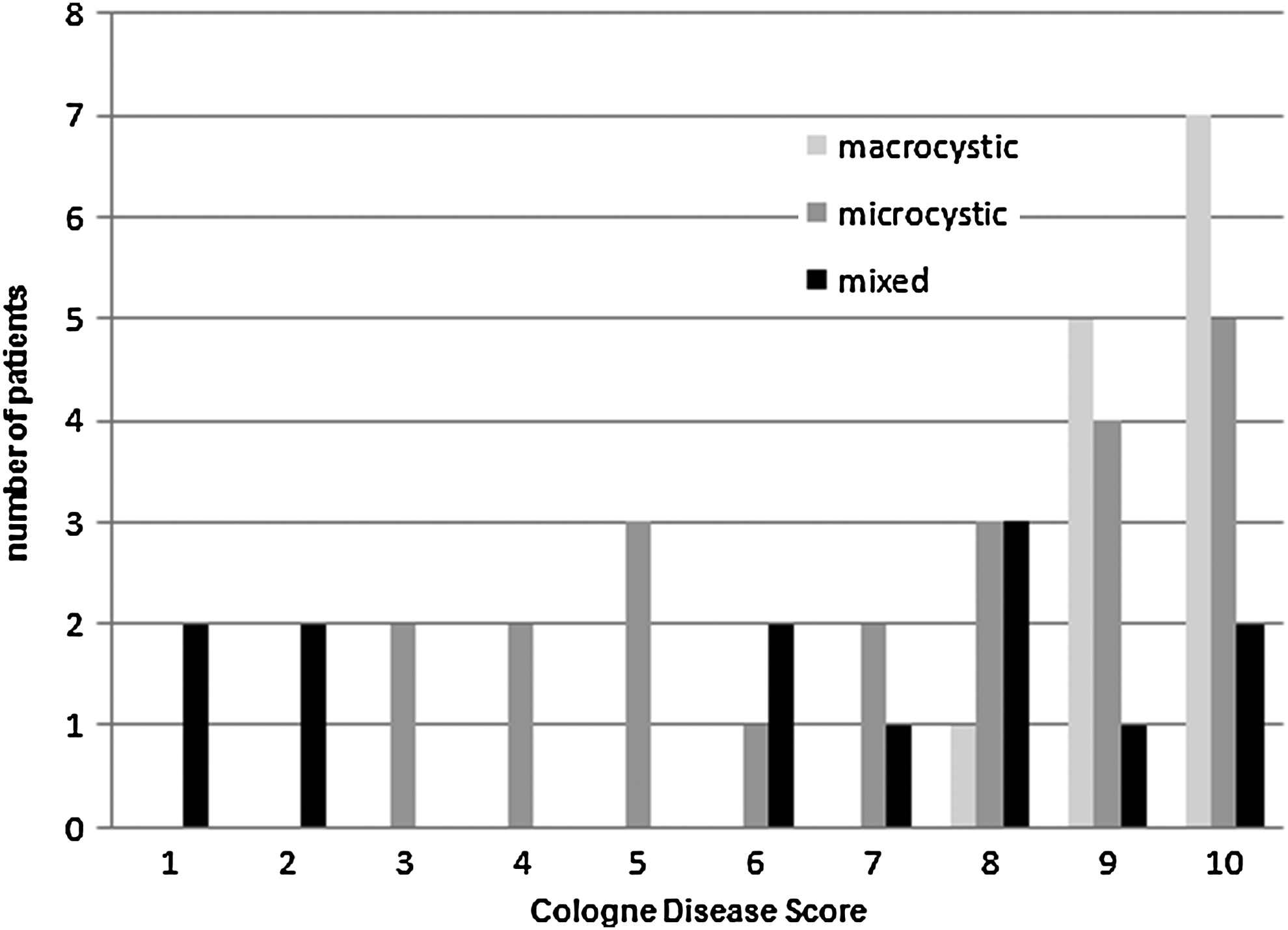
Cologne Disease Score of patients with macrocystic, microcystic, and mixed lesions showing that patients with macrocystic lymphatic malformations scored better than patients with microcystic and mixed lesions, which were accompanied by considerably lower scores.
Discussion
There are different theories regarding the etiology of lymphatic malformations, but none of these theories has been proven to be the correct one. 1 Lymphatic malformations occur most frequently in regions where the lymphatic system is formed during embryogenesis from the primary lymph sacs. 1 This suggests that the development of malformations is closely related to the maturation of the lymphatic system. 10 In 1:250 fetuses in the prenatal ultrasound nuchal brightening, the first sign of a lymphatic malformation is found, but the incidence of lymphatic malformations at birth is only 1:5000. This suggests that there is a significant degree of excessive lymphatic growth and constant conversions, which is dysregulated in certain cases, and thus results in the clinical presentation of lymphatic malformation. 11
To achieve a better assessment of prognosis and surgical outcome, de Serres et al. 9 classified lymphatic malformations in five stages. De Serres et al. 9 showed a correlation of symptoms and complications in the five stages, which were confirmed in a study of Hamoir et al. 12 In the present study, there were patients in all stages and, as described previously, 13 patients in greater stages often have more symptoms and complications.
All patients were evaluated according to the Cologne Disease Score. 8 We could show that patients with macrocystic lymphatic malformations had a lower morbidity with higher values according to the Cologne Disease Score than patients with microcystic and mixed lesions, which were accompanied by considerably lower scores.
Macrocystic lymphatic malformations are usually found in the neck, but also in the axilla and side of the chest. In the present study, macrocystic lymphatic malformations were predominately located in the lateral neck. The reason for this may be the loose connective tissue in that region which does not prevent an expansion of the lymphatic malformation. Therefore, macrocystic cysts can arise. They typically have clear margins and can be easily differentiated from the surrounding tissue. Almost all microcystic lymphatic malformations in this study were located in the floor of the mouth where a more compact connective tissue predominates. This may lead to a different structure of the malformation since the growth of the malformation is hampered by the compact tissue. It is well known that microcystic lymphatic malformations often have an infiltrative nature, lack well-defined visible or palpable margins and therefore are often incompletely excised. For these reasons, the risk of harming functionally important structures during surgery is much higher in microcystic lesions.
Another possibility for the different localization of macrocystic and microcystic lymphatic malformations may be that both types of malformation have a different etiology. Macrocystic lymphatic malformations occur in neck regions where many lymph nodes are located, while in the floor of mouth and tongue, which are the predominant localizations of microcystic lymphatic malformations, lymph nodes are sparse. Therefore, further studies will have to clarify if both types of malformations have a different origin.
This study has several limitations. Due to the retrospective nature of the study, it was not possible to get the earliest imaging before the first treatment of the patients who were previously treated at other hospitals. It is possible that macrocystic lymphatic malformations became mixed or microcystic lymphatic malformations after previous treatment with OK-432. Moreover, the extent of the malformations may have changed due to previous surgery at other hospitals. In addition to the problems of collecting retrospective data, another factor may have confounded the results presented. Intralesional hemorrhage in macrocystic lymphatic malformations produces distinctive fluid levels within the cystic portions. In rare cases macrocystic lymphatic malformations with intralesional bleeding can appear as mixed or microcystic malformations on imaging.
Conclusion
The cause for the different localization of microcystic and macrocystic lymphatic malformations is still not clarified. One reason may be the different structure of the surrounding connective tissue, which is compact in the floor of mouth and loose in the neck lateral neck so that macrocystic cysts can arise. Maybe both types of malformation have a different etiology. Therefore further studies would be required to investigate this question.
Footnotes
Author Disclosure Statement
No competing financial interests exist.