
Abstract
Abstract
Background and Objectives:
For patients with melanoma, the choice between an inguinal lymph node dissection (ILND) alone and both an ILND and a pelvic lymph node dissection (PLND) is controversial. Although Cloquet's node (CN) is considered the sentinel pelvic node, evaluation of this factor to predict pelvic node status has produced varied results. We investigated inguinal and pelvic lymphatic drainage patterns and focused on CN to clarify whether CN status could be an indicator of PLND.
Methods:
Patients with primary cutaneous lower limb melanoma who underwent lymphatic mapping and sentinel lymph node biopsy (SLNB) using dynamic lymphoscintigraphy and SPECT/CT were retrospectively reviewed.
Results:
Thirty-two patients underwent lymphatic mapping and SLNB. Each patient's CN was identified by SPECT/CT. A radioactive CN was detected in only 37.5% (12/32) of patients, and no lymphatic drainage to CN occurred in 62.5% (20/32). In 37.5% (12/32) of patients, the lymph drained directly from the inguinal to the pelvic nodes bypassing CN.
Conclusion:
In melanoma patients, lymphatic drainage from the lower extremity does not always pass from the inguinal node to the pelvic nodes via CN. Tumor-negative status of CN alone is of limited value as an indicator for avoiding PLND.
Introduction
S
One of the most controversial issues in treating patients with lower limb melanoma is the choice between performing an inguinal lymph node dissection (ILND) alone and performing both an ILND and a pelvic lymph node dissection (PLND).1–4 When external iliac or obturator nodal metastasis is suspected clinically or radiologically in addition to inguinal nodal involvement, ILND and PLND is generally recommended.1,2,5,6 In contrast, ILND plus PLND has not been widely recommended for patients with positive SLNs or palpable inguinal nodal disease alone because there is little evidence showing an overall survival benefit with the addition of PLND.7,8
However, several authors have advocated both ILND and PLND for regional control because 30%–50% of patients with palpable inguinal nodal disease also have microscopic pelvic nodal involvement.2,7–11 As predictive factors for pelvic nodal disease, (1) a metastatic Cloquet's node (CN), (2) four or more metastatic inguinal nodes, (3) metastatic inguinal nodes with extracapsular extension, and (4) palpable inguinal nodes, have been proposed, and additional PLND for patients with these factors has been considered.2,7–12 However, evaluation of these factors has produced varied results.
Cloquet's node, which was first described by Jules Germain Cloquet in the 19th century, is defined as the highest node of the inguinal basin lying in the femoral ring just medial to the femoral vein at the level of the inguinal ligament13,14 (Fig. 1). CN is considered the “SLN” of the pelvic field. 9 However, to our best knowledge, there has been no investigation of the actual rate of lymphatic drainage from the lower limb to CN.
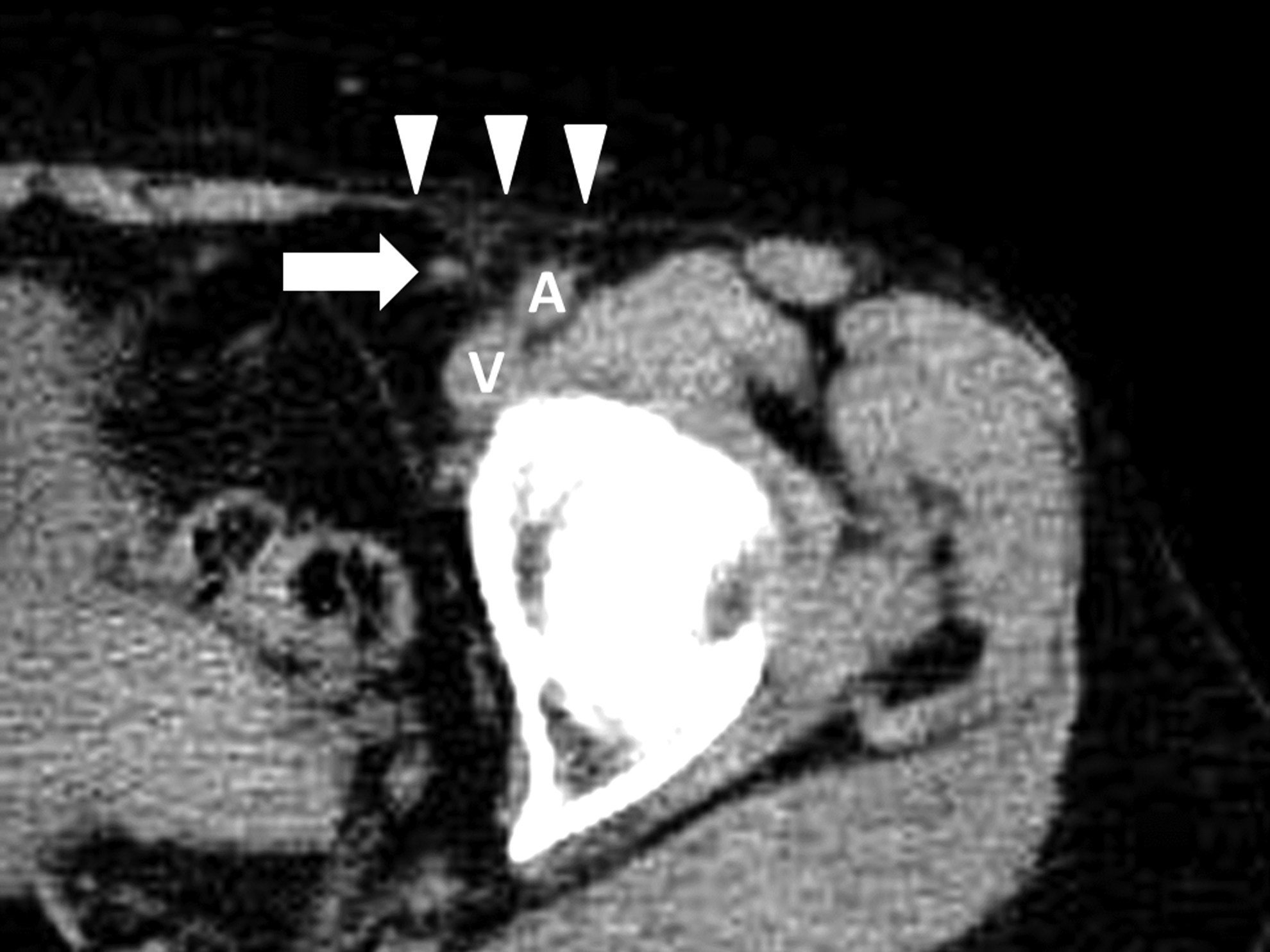
Axial view of a plain CT showing a Cloquet's node identified medial to the femoral vein under the inguinal ligament (left inguinal area). White arrow, Cloquet's node; A, femoral artery; V, femoral vein; arrowheads, inguinal ligament.
Conventional lymphoscintigraphy provides information regarding lymphatic drainage patterns and the number and approximate location of SLNs. Based on the concept that the lymphatic drainage runs in an orderly stepwise fashion, the second-tier node is considered to be the next lymph node involved when the SLNs have metastasis. 15 Early dynamic images can distinguish SLNs from the second-tier nodes, which receive lymphatic drainage directly from SLNs. Although the exact anatomical positions of SLNs and second-tier nodes cannot be evaluated preoperatively by lymphoscintigraphy alone, the advent of hybrid single-photon emission computed tomography combined with CT (SPECT/CT) has made it possible to visualize and evaluate the exact anatomical location of these nodes preoperatively.16–18
In this study, we investigated lymphatic drainage patterns in the inguinal and pelvic areas of patients with lower limb melanoma, with a particular focus on lymphatic drainage to CN, by using dynamic lymphoscintigraphy and SPECT/CT, and we evaluated whether the status of CN alone could be used as an indicator for determination of PLND.
Materials and Methods
Patients
Patients with primary cutaneous melanoma of the lower limb who underwent lymphatic mapping and SLNB between April 2009 and April 2014 at Saitama Medical University International Medical Center were included in the study and retrospectively reviewed. The consent of patients was obtained. The study was approved by the institutional review board and human research ethics committee at our institution, which was conducted in accordance with the ethical guideline of the 1975 Declaration of Helsinki, revised in 2008. Patients were excluded from the study if they had distant metastases or clinical evidence of inguinal nodal metastases. Patients who had already undergone ILND or PLND due to other malignancies such as colon or uterine cancer, who had chronic lymphedema of the lower limb, or who had a history of severe injuries of the lower limb, were also excluded from the study.
Lymphoscintigraphy and SPECT/CT
Lymphoscintigraphy was performed after intradermal injection of approximately 80 MBq of technetium-99m tin colloid (Japan Mediphisic, Tokyo, Japan) in four equal deposits around the primary site on the day before SLNB. Dynamic images were taken immediately after injection of the radioisotope tracer to detect SLNs and second-tier nodes (Fig. 2). Static images were made by SPECT and CT scans from the inguinal to the pelvic area 4 hours after injection, and an image fusion of SPECT and CT scans was performed to identify the exact anatomical location of CN, SLNs, second-tier nodes, and the other radioactive nodes higher up the lymphatic chain (Figs. 1 and 3).
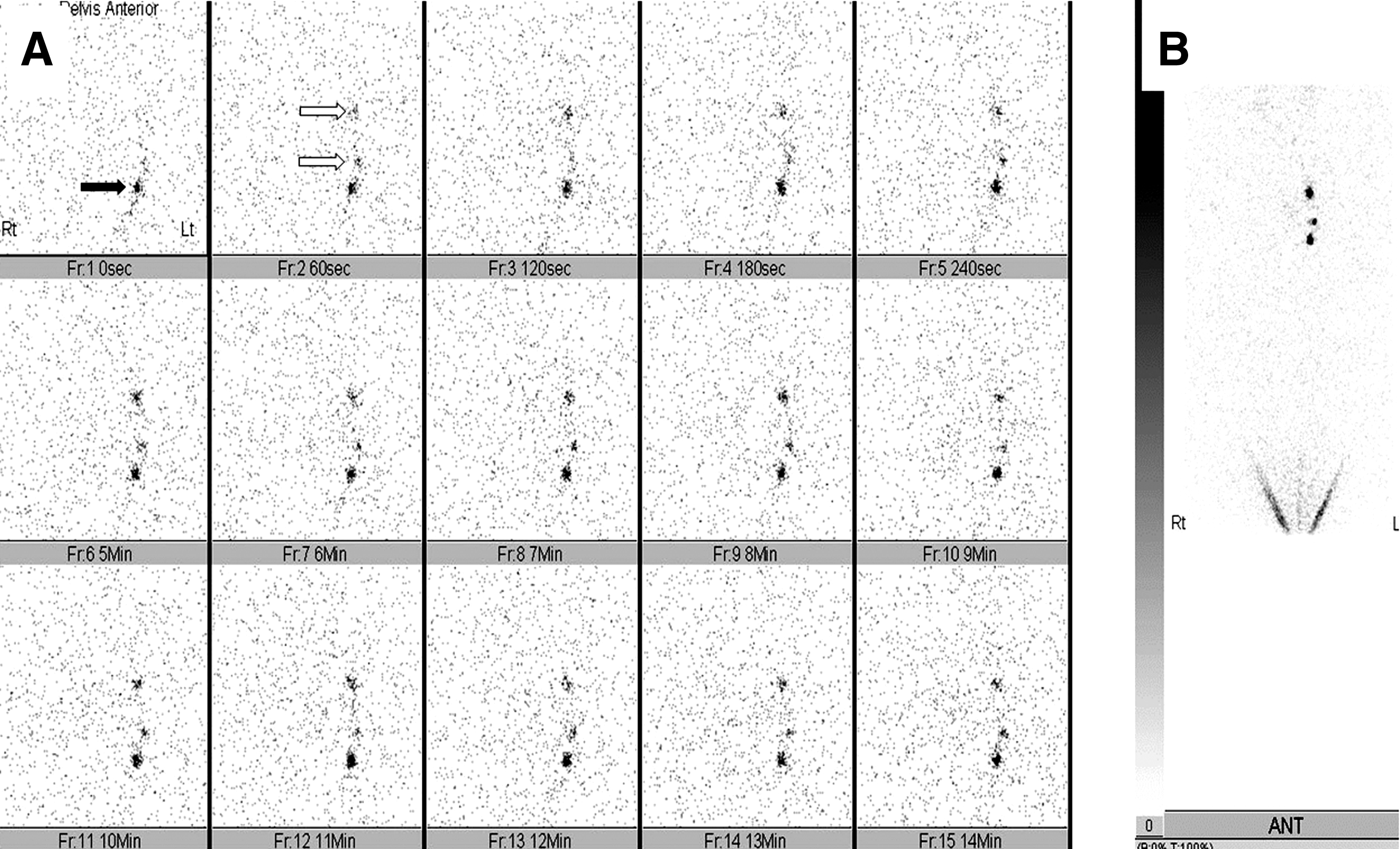
Lymphoscintigraphy.
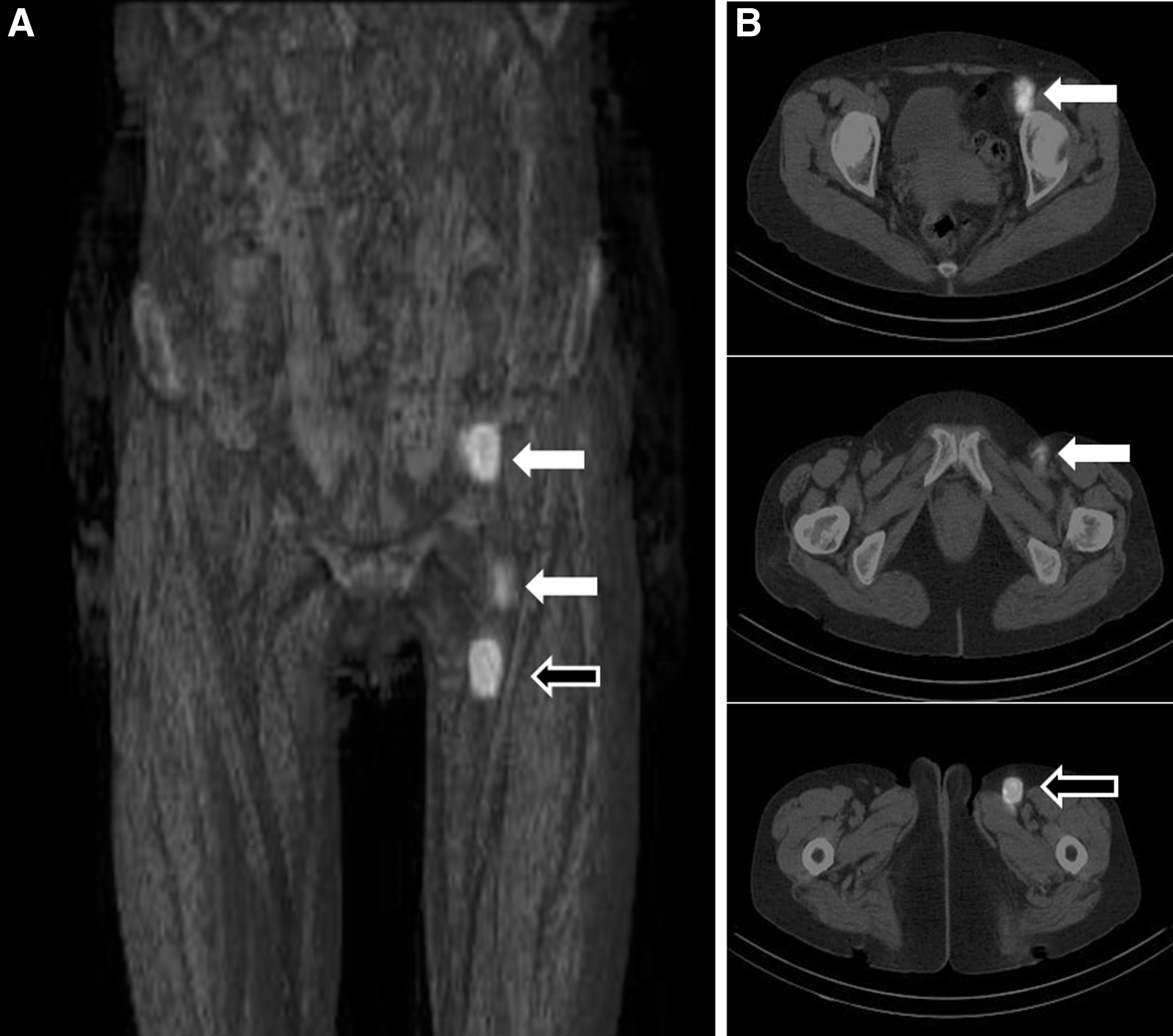
SPECT/CT.
A SLN was defined as a lymph node that receives the lymphatic drainage directly from the primary tumor site. 19 A second-tier node was defined as a lymph node that lies on a direct lymphatic drainage pathway from the SLN. If CN showed radioactivity in the SPECT/CT, the pattern of its radioactivity was evaluated to determine whether it corresponded to a SLN, a second-tier node, or a higher-tier node.
Results
The patient characteristics are shown in Table 1. Thirty-two patients underwent lymphatic mapping and SLNB. Patients consisted of 19 males and 13 females. The mean age was 67.6 years (range, 35–86 years). Twenty-six patients had melanoma of the foot, 8 melanoma of the heel, and 4 melanoma of the toe. The most frequent histological type was acral lentiginous melanoma (25/32 patients, 78.1%).
ALM, acral lentiginous melanoma; NM, nodular melanoma; SSM, superficial spreading melanoma.
Cloquet's node was visualized and identified in the SPECT/CT in all patients. Radioisotope accumulation in CN, which indicates lymphatic drainage to CN, was detected in 12 of 32 patients (37.5%) (Fig. 4). In all of these patients, the radioactive CN was observed in both the dynamic images and/or SPECT/CT. In the classification of CN based on the pattern of radioactivity, CN was identified as a SLN in 2 patients, a second-tier node in 6 patients, and a third- or higher-tier node in 4 patients (Fig. 4). In one of 2 patients whose CN was identified as a SLN, the radioactive CN was detected in the SPECT/CT alone and was not depicted in early dynamic images.
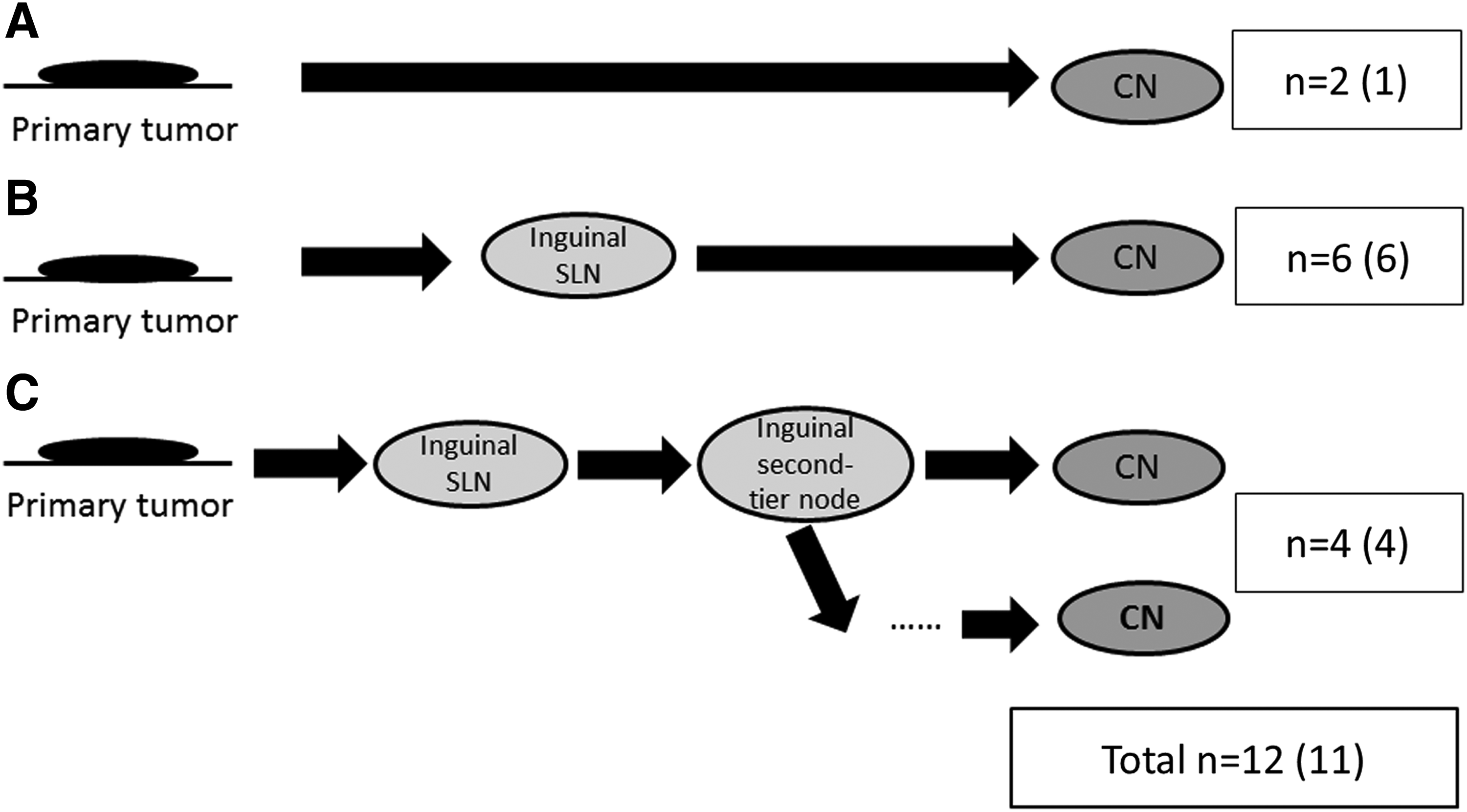
Lymphatic drainage patterns in 12 patients with a radioactive Cloquet's node (CN).
In contrast, 20 of 32 patients (62.5%) showed no radioactivity in CN (Fig. 5). Eight of these 20 patients had radioactive nodes, which included SLNs and second- or higher-tier nodes in the inguinal area alone but no radioactive nodes in the pelvic area in both dynamic lymphoscintigraphy and SPECT/CT images. In the remaining 12 patients, radioactive nodes were identified in both the inguinal and pelvic areas, and these patients had at least one second- or higher-tier node in the pelvic area. If the former 8 patients were excluded from the analysis because those patients had a possibility of drainage to the pelvic nodes after SPECT/CT, 12 of 24 (50%) patients would have shown drainage to the pelvic area without passing through CN (Fig. 5).
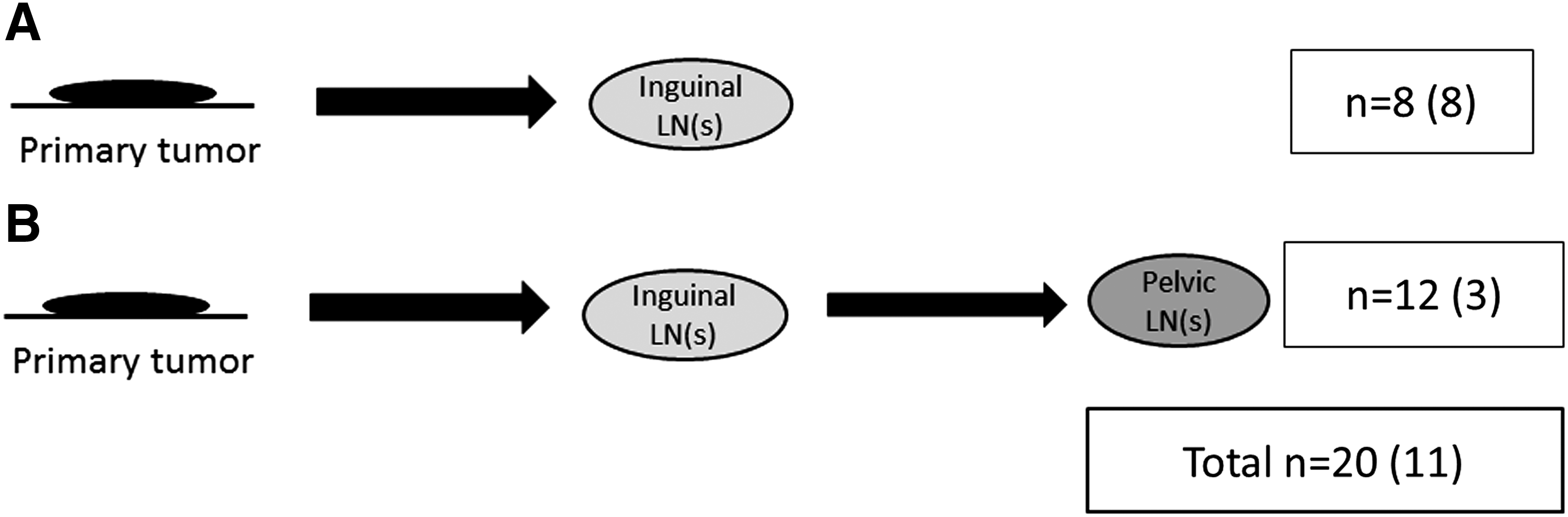
Lymphatic drainage patterns in 20 patients with no radioactive Cloquet's node.
Discussion
Cloquet's node has previously been considered the SLN of the pelvic area. To date, six reports have investigated the validity of CN status as a predictive factor of pelvic nodal status in lower limb melanoma patients. However, these studies showed conflicting results.
Several authors have advocated CN tumor status as a reliable predictive factor to determine pelvic nodal disease. Coit et al. 20 reported a high sensitivity and negative predictive value of CN status of 90% and 95%. Shen et al. 9 reported that the sensitivity of CN status was 82% with the use of immunohistochemical staining. Essner et al. 21 also reported the sensitivity of CN status to be 80%, with positive and negative predictive values of 66% and 97%, respectively.
In contrast, other authors have questioned the predictive value of CN tumor status for pelvic nodal disease. Illig et al. 22 tested the role of diagnostic excision of CN, and its sensitivity to predict pelvic nodal involvement was only 44%. Similarly, in the study of Strobbe et al., 11 CN status had a low sensitivity of 41%, and additional immunohistochemical staining of CN resulted in a limited increased sensitivity of no more than 65%. Positive and negative predictive values were 69% and 78%, respectively. Recently, Chu et al. 14 investigated the predictive value of CN status for pelvic nodal disease in SLN-positive melanoma patients and found a low sensitivity of CN status of 25%, although the negative predictive value of 94% was relatively high. These negative results have led to the conclusion that CN tumor status has a limited value as a predictive factor of pelvic node involvement.
The studies described above were based on the association between the histologic status of CN and that of pelvic nodes and lacked information of lymphatic drainage patterns in the inguinal and pelvic areas, including CN. In addition to conventional lymphoscintigraphy, recently introduced SPECT/CT techniques enable visualization of the exact anatomical location of radioactive nodes. Therefore, we investigated the drainage patterns in the inguinal and pelvic areas, and we used these images to focus particularly on CN.
To our knowledge, this is the first report investigating the lymphatic drainage patterns to CN for its validity as a predictive factor for pelvic nodal status. In the present study, CNs could be detected in all patients using CT scan image of SPECT/CT, although several authors advocate that CN is not anatomically constant. 23 Only 37.5% of patients (12/32) had lymphatic drainage to CN, and more than 60% of patients (20/32) showed no lymphatic drainage to CN. Furthermore, 37.5% of patients (12/32) showed a lymphatic drainage pattern flowing directly from the inguinal nodes to the pelvic nodes without passing through CN. These data indicate that the tumor-negative status of CN has limited utility as an indicator for avoiding PLND.
Two similar lymphoscintigraphic studies showed lymphatic drainage “skipping” directly to the pelvic nodes, although the CN status was not investigated in these studies.24,25 For example, the lymphoscintigraphic study reported by van der Ploeg et al. 24 demonstrated 6 of 84 SLNs (7%) and 56 of 90 second-tier nodes (62%) in the pelvic area. They concluded that a high frequency of pelvic second-tier nodes indicates the need for PLND in many patients with positive inguinal SLNs. There are also several reports stating that 9%–17% of patients with a microscopically positive inguinal SLN also have positive pelvic nodes,26–28 which may implicate a direct lymphatic drainage from the SLN to the pelvic nodes. These findings, together with data in the present study, suggest that PLND should be selectively performed based on confirmation of the location of second-tier nodes on lymphoscintigraphy and SPECT/CT in patients with positive inguinal SLNs.
Understandably, the present study has some limitations in that it focused on lymphatic drainage patterns and lacks information on the clinical outcome of patients who have regional lymph node metastases. Patients who had radioactive nodes in the inguinal area alone have a possibility of showing drainage to CN and subsequent nodes in the pelvic area after at the time of SPECT/CT imaging. Moreover, in this study, we used tin-colloid as a tracer, which has a large particle diameter. If we had used smaller diameter particle tracers (such as human serum albumin and phytate), we might have detected more radioactive nodes in the pelvic area.
However, a significant percentage of patients with direct lymphatic drainage to the pelvic nodes, skipping CN, does exist, and the exact evaluation of the anatomical location of the SLN and subsequent nodes using both dynamic lymphoscintigraphy and SPECT/CT might guide the extent of complete LND in patients who have such a lymphatic drainage pattern.
In conclusion, CN is not always the SLN of the pelvic area, and lymphatic drainage from the lower extremity does not always pass from inguinal nodes to the pelvic nodes via CN.
Footnotes
Acknowledgments
This work was partly supported by the National Cancer Center Research and Development Fund (26-A-4).
Author Disclosure Statement
No competing financial interests exist.