
Abstract
Abstract
Background:
Lymphedema is an irreversible inflammatory condition caused by accumulated lymph fluid and is associated with chronic swelling and increased risk of cellulitis. Our objectives were to: (1) describe the patient population referred to a Canadian lymphedema center and (2) compare lymphedema characteristics between patients with cancer and patients with noncancer diagnoses.
Methods and Results:
A retrospective cohort study was conducted of new patients referred for suspected lymphedema to a hospital-based center over a 2-year period. The mean age of the patients (n = 429) was 61.4 years; 85% were female and 81% had a history of cancer. Lymphedema characteristics were primary (7%) versus secondary (92%); upper body (51%) versus lower body (45%); unilateral (74%) versus bilateral (25%); and history of cellulitis (22%). Patients with noncancer diagnoses (n = 82) were more likely than patients with cancer diagnoses (n = 347) to have a history of cellulitis (44% vs. 17%), to have bilateral (61% vs. 16%) and lower limb (89% vs. 37%) lymphedema, and to experience a long delay between symptom onset and referral (14.0 vs. 3.5 years) (p < 0.001).
Conclusion:
Most patients referred to our lymphedema center were female with a history of cancer. However, patients with noncancer diagnoses were more likely to have bilateral lower body lymphedema with an important history of cellulitis; this subgroup is at great risk of missed and delayed diagnoses in the medical setting and of experiencing long-term issues with mobility, recurrent hospitalizations, and poor quality of life.
Introduction
L
Less well recognized is noncancer lymphedema. Most cases of chronic lower limb edema coexisting with obesity, chronic venous disease, or immobility are in fact manifestations of lymphatic transport failure or lymphedema, for which current treatments to control the condition are available, but are underutilized. 3 Deep vein thrombosis and chronic venous insufficiency compromise both lymphatic and venous drainage and lead to chronic lymphedema (sometimes referred to as mixed edema). 12 Early diagnosis and prompt initiation of adequate treatment are required to reduce morbidity associated with potential cellulitis and sepsis. 1
Without proper treatment, chronic edema tends to progress, leading to recurrent subcutaneous tissue infections, poor wound healing, and frequent hospitalizations. 3 Reduced mobility, pain, and reduced physical function are commonly reported. 13 Chronic lymphedema is associated with decreased quality of life and increased medical costs to patients and to the health care system.14–16 Numerous studies have found that lymphedema has a negative impact on psychosocial and sexual functioning, work, and leisure activities.13,17–19
Lymphedema management is lifelong and complex, requiring patient adherence to several concurrent treatment modalities, including compression bandaging, compression garments (often custom-made and expensive), exercises, weight control, and skin care. Unfortunately, lymphedema is greatly underdiagnosed and undertreated due to lack of knowledge in the medical community and to limited funding for appropriate management and specialized clinical services.3,20,21
Despite the impact of lymphedema on patient functioning and the health care system, little is known about the characteristics of the lymphedema population, particularly noncancer cases. Our objectives were to describe the lymphedema patient population referred to a Canadian hospital-based lymphedema center, according to medical history, lymphedema characteristics, and cellulitis history and to compare these characteristics between patients with cancer and patients with noncancer diagnoses.
Materials and Methods
Study design
A retrospective cohort study was performed of new patients assessed at the McGill University Health Centre (MUHC) Lymphedema Program between April 1, 2012 and March 31, 2014. Approval for this study was granted by the MUHC Research Ethics Board.
Program description
Located in Montreal, Canada, the MUHC Lymphedema Program was established in 1994 by Dr. Anna Towers, a family physician trained in palliative care and lymphedema therapy. In 2008, the center received charitable support to expand to a multidisciplinary clinical service with the addition of a lymphedema-trained physiotherapist, an exercise trainer, and a volunteer from the Lymphedema Association of Quebec. Currently, the program offers medical assessment and diagnosis, education on individualized self-management and exercise, and referral to community lymphedema therapists for combined decongestive therapy and/or to private suppliers for compression garments.
Population
As part of the MUHC Cancer Care Mission and the Supportive and Palliative Care Services, the program referral criteria are currently limited to patients with cancer-related lymphedema. However, due to the substantial number of requests for assessment of noncancer lymphedema, up to 2014, all referrals were accepted regardless of etiology. Patients with suspected lymphedema are referred from all of Quebec and parts of eastern Ontario and are followed at the clinic every three to 12 months depending on case complexity and need for lymphedema management.
Outcome measures
Since 2012, data from patient assessments have been compiled in an electronic database. The following information from the initial assessments was extracted: patient demographics, medical diagnosis and surgical history, lymphedema characteristics, and number of cellulitis episodes. Relevant history of surgeries contributing to lymphedema had been obtained from the patients. Regarding cellulitis, patients had been asked about bacterial infections in the affected limb(s) requiring oral or parenteral antibiotics, with or without hospitalization. Paper-based medical records were also reviewed as necessary.
Data analysis
Statistical analyses were performed using the JMP statistical software (version 12). Descriptive statistics was used to characterize the patient population and analysis of variance and chi-squared tests were used to compare subgroups.
Results
Patient characteristics
Within the study period, information was collected on 429 new patients suspected to have lymphedema (Table 1). Of the 347 patients with cancer diagnoses, 95.7% had one cancer only (n = 332), 2.6% had two cancers (n = 9), and 1.7% also had a noncancer-related diagnosis contributing to their lymphedema (n = 6) (Fig. 1). Of the 82 noncancer patients, 36.6% had primary lymphedema (n = 30) while the remaining had secondary sources of lymphedema (Fig. 2).
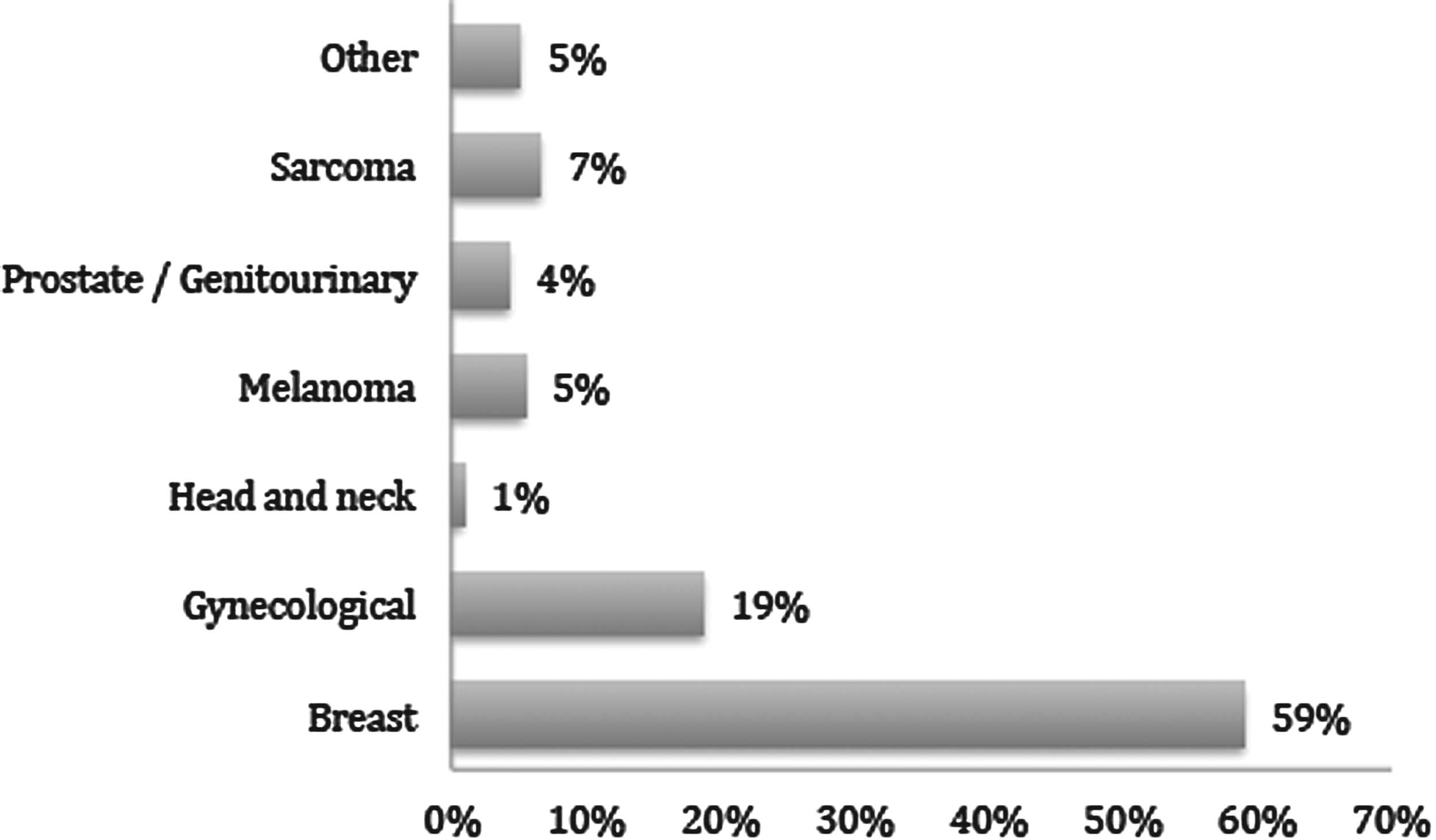
Medical diagnoses in patients with cancer-related lymphedema (one cancer only, n = 332).
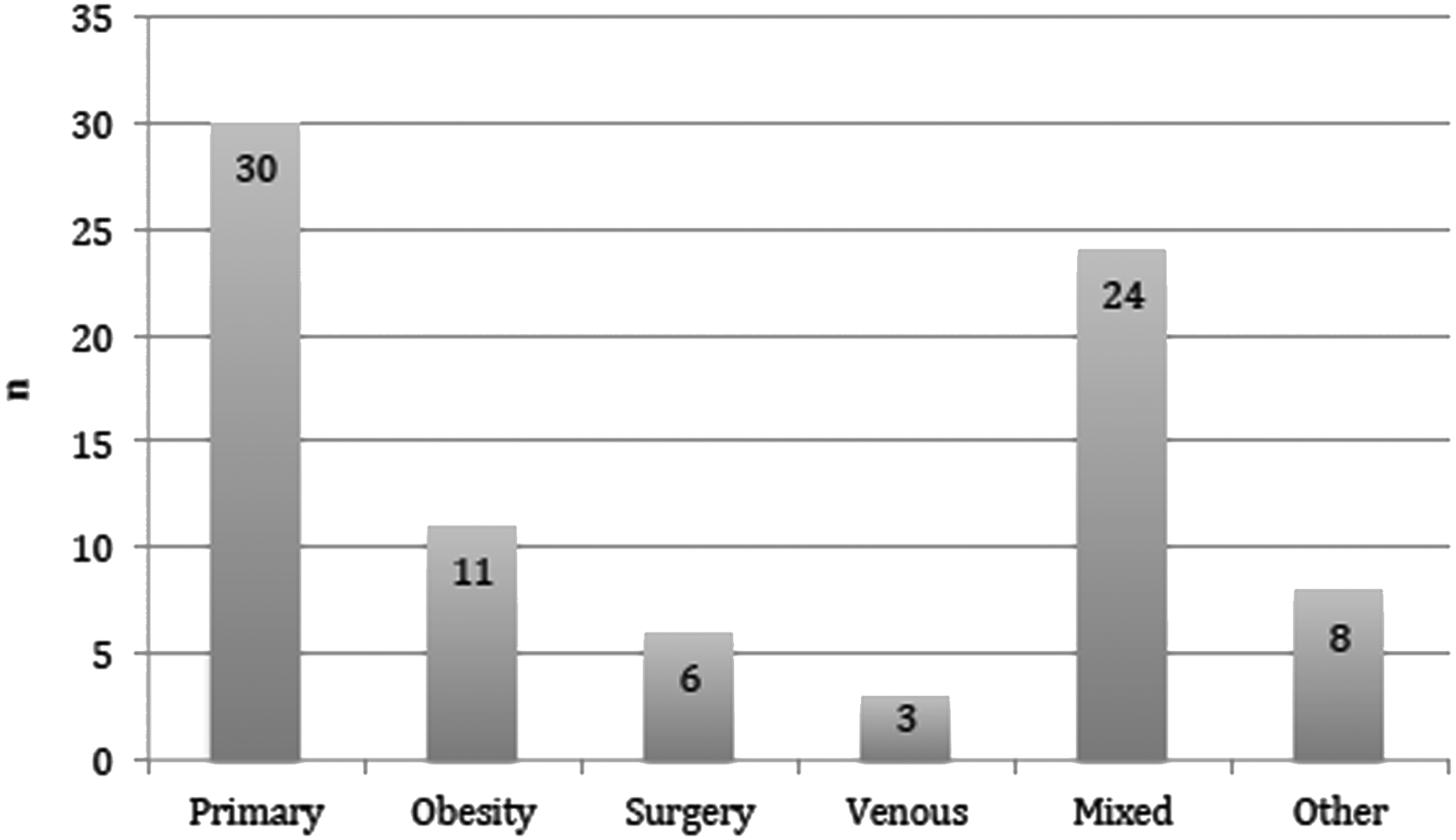
Lymphedema etiology in patients with noncancer diagnoses (n = 82).
SD, standard deviation.
Table 2 provides information on lymphedema characteristics. The patients with unilateral arm lymphedema (n = 212) had a mean limb volume difference of 16.6% (95% confidence interval [CI]: 13.5%–19.6%). In this subgroup, 78.8% of the patients were classified as having mild (≤20% excess limb volume) lymphedema, 11.3% as moderate (20%–40% excess limb volume), and 9.9% as severe (>40% excess limb volume). The patients with unilateral leg lymphedema (n = 96) had a mean limb volume difference of 18.2% (95% CI: 13.9%–22.4%); 68.8% were classified as mild, 24% as moderate, and 7.3% as severe. This classification method cannot be used for lymphedema of bilateral limbs or other body parts. 1 History of cellulitis episodes is reported in Table 3.
Patients in the “no lymphedema” category had cancer-related risk factors, but no edema at the time of initial assessment.
Time between reported date of initial lymphedema onset and recorded date of first clinical assessment, n = 392.
SD, standard deviation.
Number of cellulitis episodes reported at initial assessment.
Comparisons between patients with cancer diagnoses and patients with noncancer diagnoses
Table 4 and Figure 3 demonstrate comparisons between subgroups. Of the 58 patients with cancer who had a history of cellulitis, 81.0% had 1–3 episodes, 12.1% had 4–6 episodes, and 6.9% had >6 episodes. Of the 36 noncancer patients with a cellulitis history, 75% had 1–3 episodes, 11.1% had 4–6 episodes, and 13.9% had >6 episodes.
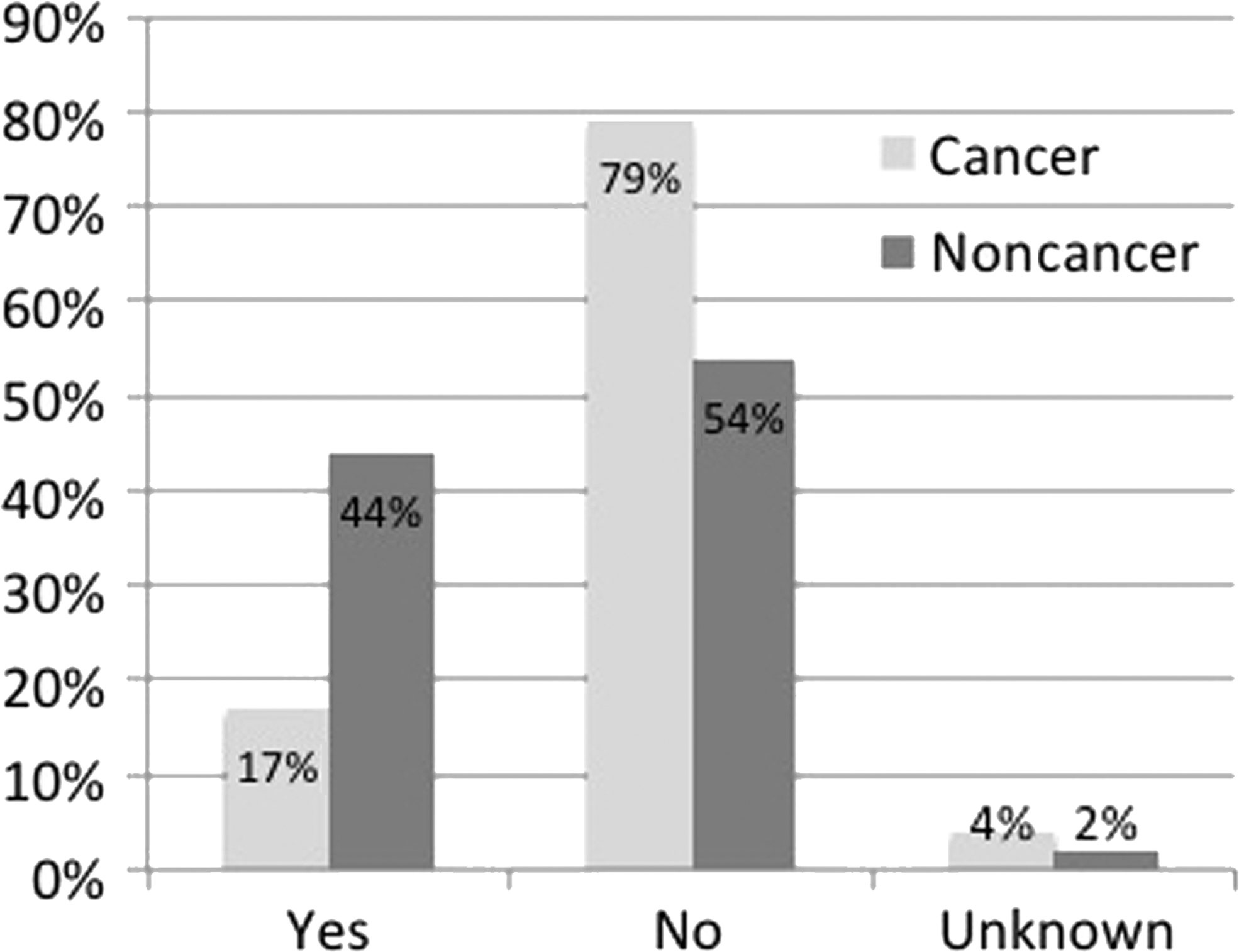
Comparisons of cellulitis history at initial assessment between patients with cancer diagnoses (n = 347) and patients with noncancer diagnoses* (n = 82). *p < 0.0001.
Location categories not mutually exclusive.
Time between reported date of initial lymphedema onset and recorded date of first clinical assessment, n = 318 for patients with cancer diagnoses and n = 74 for patients with noncancer diagnoses.
SD, standard deviation.
Discussion
Patient population
To date, lymphedema following breast cancer has been the most thoroughly and widely documented and, hence, the manifestation most recognized by physicians. DiSipio et al. in their meta-analysis of 72 studies reported that more than one in five women who survived breast cancer developed lymphedema. 22 It is not surprising therefore that this demographic accounts for the largest number of referrals to our clinic. However, it is noteworthy that almost half of our patients presented with lymphedema of the lower body related to diagnoses other than breast cancer. This demographic has not been reflected in the literature until very recently, since studies investigating incidence and risk for lower limb lymphedema have been lacking.
Likewise, the prevalence of noncancer lymphedema is unclear. Two previous studies have reported lymphedema rates ranging from 24% of cases seen in a palliative care setting to 75% in an epidemiological study of chronic edema cases within a geographical region based in the United Kingdom.21,23 It has been noted that the incidence of chronic edema increases with age. 21 Our analyses were strikingly similar, however, to those reported by Sitzia et al. in their prospective survey of 27 lymphedema treatment clinics (603 referrals) in the United Kingdom. 24 Both studies describe a patient population that is majority female with an average age in the early 60s and presenting mostly with cancer-related lymphedema. Similar outcomes of mean percentage excess volume 25 in cases of unilateral limb lymphedema are found in the two studies. A recent analysis of 225 referrals to a lymphedema program also reported more females than males, including children. 26
Comparisons between subgroups
Cellulitis is a common, potentially life-threatening bacterial infection of the skin and subcutaneous tissues for which lymphedema is one of the main risk factors.27,28 In the United States, cellulitis has been reported to account for 14% of emergency visits and up to 7% of hospital admissions. 27 In our review, the reported number of cellulitis episodes was 2.5 times greater among the noncancer population than in the cancer group. Importantly, we also reported cellulitis recurrence on four or more occasions in over 10% of the noncancer population with lymphedema. These findings may be attributed to a high risk of cellulitis in patients with noncancer lymphedema, as well as to issues with delayed diagnoses and tardy treatment onset in this population. In individuals with lymphedema, each cellulitis episode can further compromise the lymphatic system thus setting up a vicious cycle and facilitating future recurrence. 29 Physicians should be alert to the relationship between chronic edema and the risk of cellulitis and septicemia, particularly in patients with lower limb lymphedema regardless of etiology. 30 Physicians are also encouraged to refer early to lymphedema specialists for appropriate management.
Importantly, patients with noncancer diagnoses suffered from lymphedema for a much longer time period before evaluation compared to those with cancer. These findings also suggest that the noncancer subgroup is at greater risk of missed and delayed diagnoses. Late diagnosis and inappropriate prereferral tests and treatment have been related to more difficult management of these complex cases.24,26
Similar to Sitzia et al., we discovered higher rates of bilateral edema for the noncancer group than the cancer group. 24 Treatment of bilateral lymphedematous limbs can be significantly more time-consuming, costly, and challenging than for unilateral limbs. Deng et al. found that in patients with lower limb primary lymphedema, those with bilateral edema were more likely than those with unilateral edema to report at least one cellulitis episode and to experience symptom burden. 31 A unique finding in our study was the high prevalence in the noncancer population of lower limb lymphedema, which can have long-term debilitating effects on physical functioning and mobility.32,33 Such effects may subsequently lead to further complications such as weight gain and worsened lymphedema.
Another important finding of our study was the age difference between the two groups, with the noncancer group being younger by a mean of 6 years. This difference may be attributed to the nature of lymphedema etiology with noncancer sources of lymphedema, such as primary lymphedema and obesity, often presenting earlier in life than cancer-related lymphedema. With lymphedema manifesting at a younger age, the noncancer group is particularly at risk of developing long-term issues such as recurrent infections, functional problems, and other complications.
These findings of differences in age, lymphedema distribution and onset, and, most importantly, cellulitis history greatly emphasize the need for timely diagnosis and appropriate management of patients with noncancer lymphedema. This population is underserved and often misdiagnosed. 26 Improved clinical and diagnostic services are necessary to support this subgroup and prevent some of the long-term complications associated with noncancer lymphedema.
Strengths and limitations
Our report provides the first analysis, with information on cellulitis episodes, of a cohort of 429 new patients referred for suspected lymphedema to a Canadian hospital-based center. Thus, we offer a snapshot of a poorly recognized and underreported lymphedema population in Canada.
Aside from pediatric lymphedema clinics, most Canadian lymphedema programs are developing under oncology services. As a result, those with chronic noncancer lymphedema or mixed edema are poorly documented and are less frequently referred for thorough investigation. Two previous non-Canadian studies have reported higher prevalence of noncancer lymphedema than our findings.21,23 Moffatt et al. performed an epidemiological study of patients with chronic edema 21 while our study was a retrospective review of patients referred to a specialized lymphedema clinic. Therefore, a possible study limitation is that our findings may underestimate the true prevalence of noncancer lymphedema in Canada.
Our data related to history of cellulitis episodes were recorded categorically and as prevalence figures. Given that patients with noncancer-related lymphedema were generally referred much later after symptom onset than those with cancer-related lymphedema, it is possible that the incidence rate of cellulitis infection over time (i.e., episodes per year) may not have differed between the two groups. However, each cellulitis episode is associated with subsequent worsening of lymphedema, other patient complications, and thus, increased costs to the health care system.34,35 The late referral pattern of noncancer cases for specialized management is an important finding in itself and warrants attention in the medical community. Therefore, these differences are noteworthy and highlight the critical need to provide timely and appropriate services for the noncancer population.
Conclusions
Most patients referred to our lymphedema center were older females with a history of cancer. Patients with noncancer diagnoses were more likely to be younger, and to have bilateral, lower limb lymphedema of longer duration before referral. This subgroup was also more likely to have an important history of cellulitis infection. Patients with noncancer lymphedema are at great risk of missed and delayed diagnoses in the medical setting and of experiencing chronic issues with mobility, recurrent hospitalizations, and poor quality of life. These patients frequently present as more complex cases and require more intensive multidisciplinary treatments, often including home care. Family physicians and specialists (vascular, wound care, infectious diseases, oncology, and palliative care) need improved education and understanding to diagnose lymphedema in a timely manner, prescribe adequate treatment, and assist patients in avoiding the many complications associated with this condition. Health professionals trained in lymphedema assessment and treatment are present in various settings across North America, but are not always known to the medical community. Lymphedema associations provide patient education and information on local resources. Better integration of lymphedema treatment within health care networks, more health professionals trained in lymphedema management, and specialized clinical services for noncancer lymphedema are also greatly needed to better support this population.
Footnotes
Acknowledgments
The authors thank Kevin Yu-Chueh Lin, Sarah Khan, Natasha Grant, Angela Yung, and Michael Liben for their assistance with data entry and extraction.
Author Disclosure Statement
No competing financial interests exist.