
Abstract
Background:
Primary lymphedema results from the anomalous development of the lymphatic system that typically presents during infancy, childhood, or adolescence. Adult-onset primary lymphedema is rare and has not been studied. The purpose of this investigation was to characterize patients with primary lymphedema that developed after the pediatric time period to better understand the condition.
Study Design:
Patients treated in our Lymphedema Program between 2009 and 2018 were reviewed. Diagnosis was determined based on history, physical examination, and imaging studies. Patients with primary lymphedema developing in adulthood (>21 years) were identified. Sex, age of onset, location, severity, morbidity, family history, associated features, and lymphoscintigraphy findings were documented.
Results:
Twenty-six patients (10%) of 259 with primary lymphedema developed the disease during adulthood. Sixteen individuals were female, and the disease occurred at an average age of 40 years (range, 24–72). It affected the lower extremity (85%) (unilateral 82%, bilateral 18%) or upper limb (15%) (unilateral 80%, bilateral 20%). Twenty-seven percent of patients suffered infections. Ninety-five percent of lymphoscintigrams exhibited delayed transit of radiolabeled tracer and 73% showed dermal backflow. None of the patients had systemic lymphatic involvement or associated vascular anomalies. One patient had a family history of lymphedema.
Conclusions:
Adult-onset primary lymphedema is typically unilateral, affects the lower extremity, and is not associated with systemic lymphatic anomalies; hereditary transmission is rare. Because adult-onset lymphedema is much less common than the pediatric condition, the disease should be confirmed with lymphoscintigraphy. Imaging of the axillary or inguinal nodes is also considered to rule out a lesion causing secondary lymphedema.
Introduction
Primary idiopathic lymphedema is rare, affecting ∼1/100,000 persons in the pediatric age group. 1 The disease almost always involves the lower extremities, but the arms and genitalia can be affected. 2 Primary lymphedema is a pediatric disease, and patients typically develop swelling during infancy, childhood, or adolescence. 3 Although adult-onset lymphedema has been described in case reports and as part of larger series of primary lymphedema, a cohort of these patients has not been studied. The purpose of this investigation was to analyze individuals with adult-onset primary lymphedema to better understand the condition.
Materials and Methods
The Committee on Clinical Investigation at Boston Children's Hospital approved this study. Patients evaluated in our Lymphedema Program between 2009 and 2018 were reviewed for primary lymphedema. Subjects with adult-onset disease were then evaluated. Individuals with a body mass index (BMI) >40 were excluded because of their risk of having secondary obesity-induced lymphedema.4,5 Diagnosis was made by history, physical examination, and lymphoscintigraphy. Sex, age of onset, family history, BMI, morbidity, associated features, and lymphoscintigraphy findings were recorded. Clinical severity was documented based on the International Society of Lymphology criteria of increased limb volume: mild <20%, moderate 20%–40%, and severe >40%. 6 Abnormal lymphoscintigraphy findings included delayed transit of radiolabeled tracer to the axillary or inguinal nodes and dermal backflow.7,8
Results
Twenty-six patients (10%) of 259 individuals in our database with primary lymphedema developed the disease during adulthood (Table 1). Sixteen subjects were female, and the disease occurred at an average age of 40 years (range, 24–72 years). Lymphedema affected the lower extremity (n = 22, 85%) (unilateral n = 18, 82%; bilateral n = 4, 18%) or upper limb (n = 5, 15%) (unilateral n = 4, 80%; bilateral n = 1, 20%) (Figs. 1 and 2). Average BMI was 27 (range, 20–36). The right and left extremities were affected similarly. Twenty-seven percent of patients suffered infections. Twenty-two individuals had lymphoscintigrams: 21 exhibited delayed transit of radiolabeled colloid to the axillary or inguinal lymph nodes, and 16 had dermal backflow. We did not observe an association between location of lymphedema, lymphoscintigraphy findings, and disease severity. None of the patients had systemic lymphatic dysfunction or associated vascular anomalies. One subject (Patient No. 14 in Table 1) had a male child with left leg lymphedema (onset at 14 years of age); none of the other patients had a family history of lymphedema.
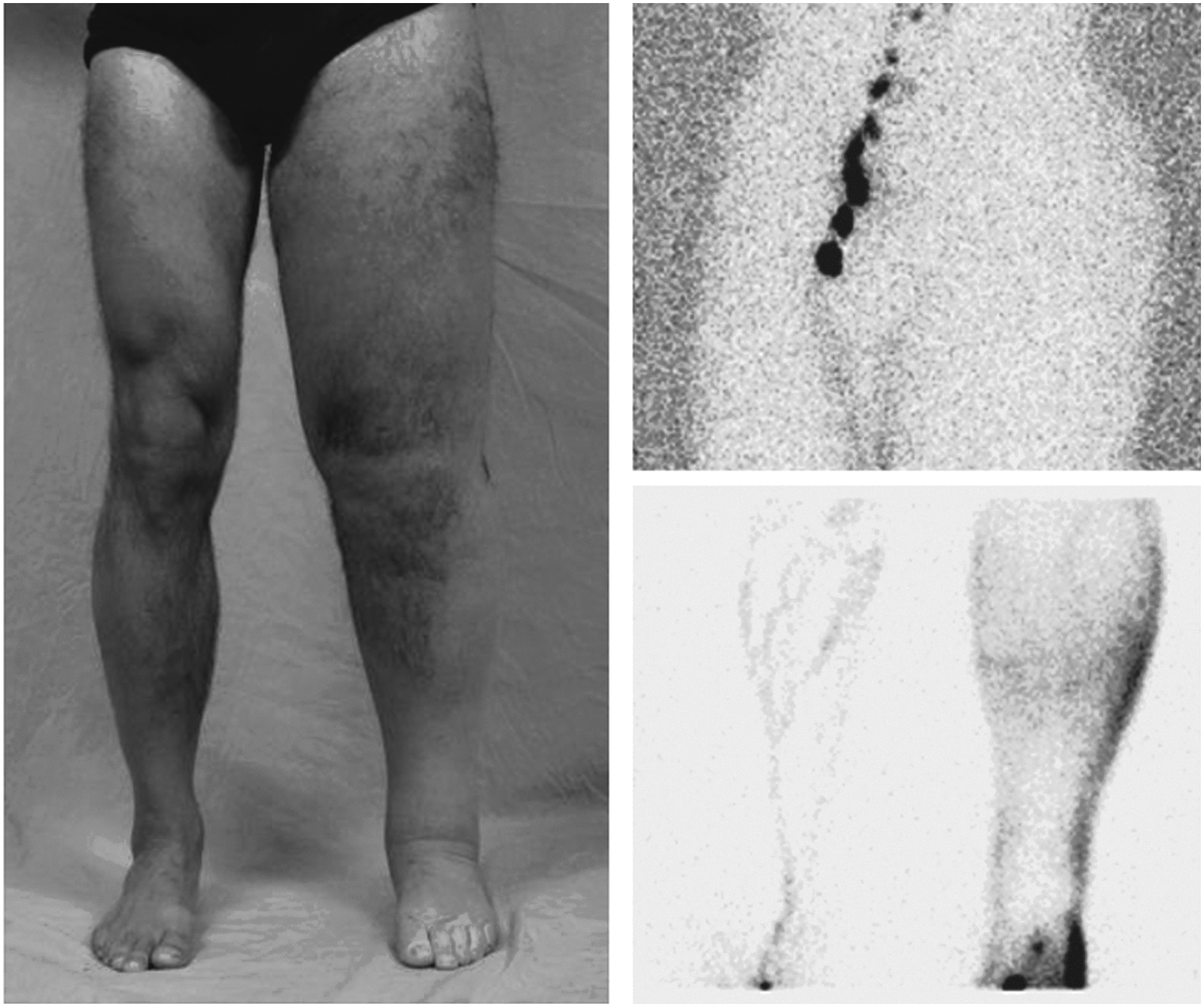
Adult-onset primary lymphedema of the lower extremity. A 45-year-old male developed left leg lymphedema (Patient No. 19 in Table 1). His lymphoscintigram showed no transit of radiolabeled tracer to the left inguinal nodes and dermal backflow 2 hours after injection.
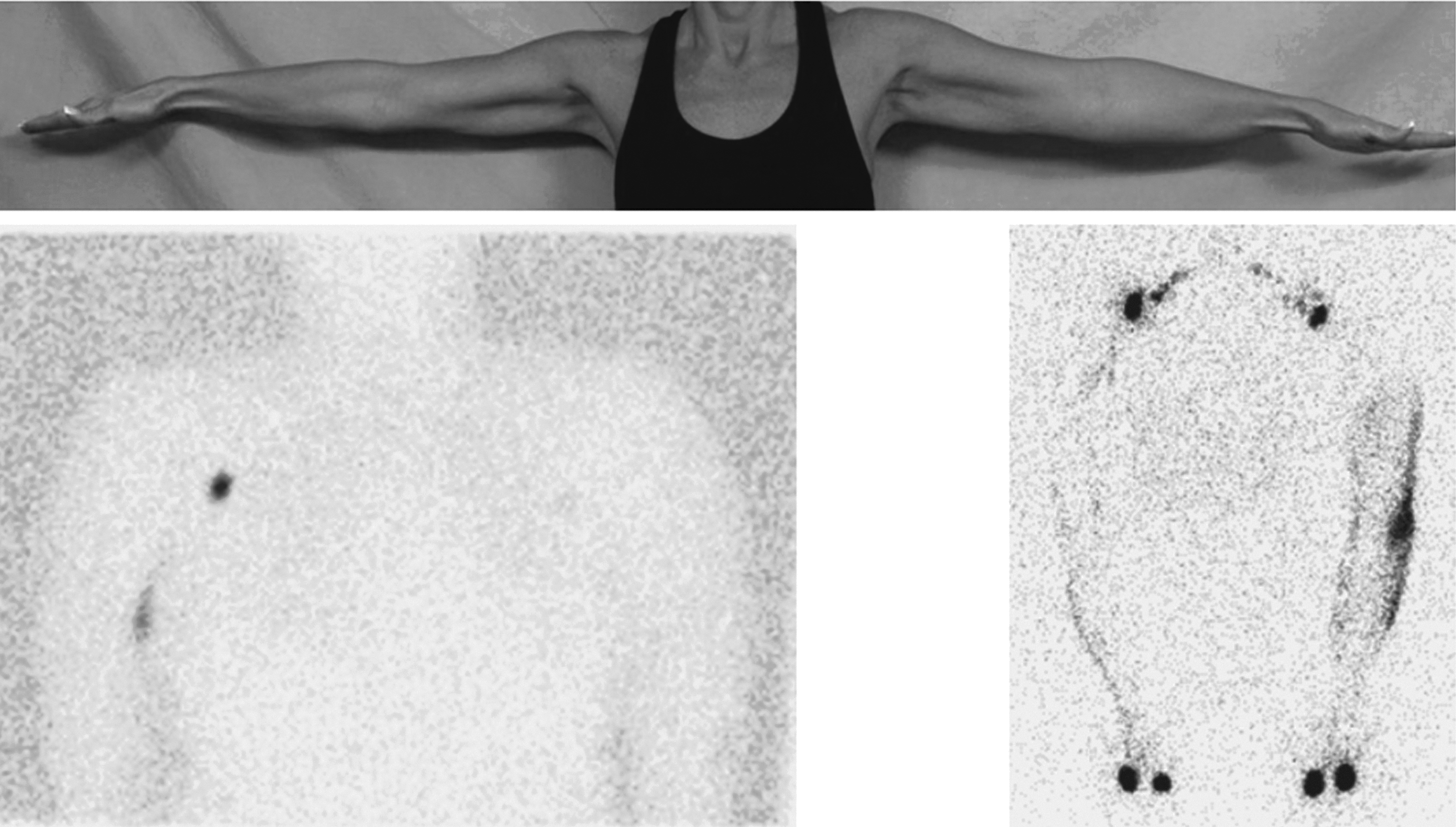
Adult-onset primary lymphedema of the upper extremity. 50-year-old female developed left arm swelling (Patient No. 22 in Table 1). Her lymphoscintigram illustrated no uptake of radiolabeled tracer to the left axillary nodes 35 minutes after injection (left image) and dermal backflow 2 hours after the injection (right image).
Phenotypes of Adult-Onset Primary Lymphedema
Inguinal nodes of affected extremity had significantly less radiolabeled tracer uptake at 45 minutes compared with the nonaffected extremity.
−, not available; BLE, bilateral lower extremity; BMI, body mass index; BUE, bilateral upper extremity; F, female; HTN, hypertension; LLE, left lower extremity; LUE, left upper extremity; M, male; RLE, right lower extremity; RUE, right upper extremity; VSD, ventricular septal defect.
Discussion
Historically, the onset of primary lymphedema had been divided into one of three categories: congenital, praecox, or tarda.9,10 Because these periods do not have standardized definitions, we have advocated the use of biologically accepted terms to define age of onset (i.e., infancy, childhood, adolescence, adulthood). 11 Adulthood is defined as age >21 by the American Academy of Pediatrics, the U.S. Department of Health, and the Food and Drug Administration.12,13
Our finding that 10% of patients with primary lymphedema developed the condition in adulthood is similar to a lymphangiographic study where 12% presented during the “tarda” period (i.e., after age 35 years). 10 We found that adult-onset primary lymphedema has a similar gender distribution and risk of upper versus lower extremity disease to the pediatric presentation. 3 However, patients with adult-onset disease have a much lower risk of bilateral leg involvement (18%) compared with the pediatric-onset population (52%). 3
Patients who develop swelling in adulthood may have a less severe developmental anomaly compared with children with the disease, and thus it takes longer for lymphatic function to fail. This hypothesis is supported by a lymphangiographic investigation that showed patients who presented in adulthood had less severe lymphatic aplasia or hypoplasia compared with individuals who exhibited the condition in early childhood. 10 Seventy-three percent of our cohort exhibited dermal backflow on lymphoscintigraphy, which is higher than the overall prevalence of dermal backflow in patients with primary lymphedema (31%). 7 Patients with adult-onset primary lymphedema may have different lymphatic structural abnormalities compared with children with the disease. Alternatively, adults might have less compensatory ability to transport lymphatic fluid than children who were born with more severely malformed lymphatics.
Only one patient in our study had a family history of lymphedema. Familial transmission and germline mutations have not been reported in subjects with adult-onset disease.9,10,14,15 It is unclear if adult-onset lymphedema has a different etiopathogenesis than the pediatric condition. Adult patients may also contain germline or somatic mutations in a gene known to cause familial pediatric lymphedema (e.g., VEGFR3, FOXC2, SOX18, PTPN14 GJC2, CCBE1). 14 Alternatively, adult-onset primary lymphedema may result from a novel germline or somatic mutation. The disease could also be a form of secondary lymphedema if an individual predisposed to lymphedema develops the condition because of other factors. Although patients with adult-onset lymphedema developed clinical swelling later than pediatric patients, we did not find that they had less morbidity. Some individuals had minimal progression, while others had significant problems, including infections; none developed a lymphangiosarcoma. 16
Because adult-onset lymphedema is the least common period to develop the condition we advocate for lymphoscintigraphy to confirm the disease. 7 One fourth of patients referred to a lymphedema center with “lymphedema” have another condition, and many other diseases can cause an overgrown limb.17,18 In the adult population, if lymphedema is documented by lymphoscintigraphy we will also image the axilla or inguinal region with MRI to ensure the patient does not have a lesion causing secondary lymphedema. Patients with suspected adult-onset lymphedema should be referred to specialists focused on this disease.
Footnotes
Author Disclosure Statement
The authors have no financial interest in this article.