
Abstract
Background:
Gut-lymph in animal models of acute disease is altered by intestinal ischemia and contributes to the development of systemic inflammation and organ dysfunction. Investigating gut-lymph in humans is hampered difficulty in accessing the thoracic duct (TD) for lymph sampling. The aims of this study were to develop and pilot a technique of intraoperative TD cannulation with delayed embolization to serially measure TD lymph pressure, flow, and composition (including markers of intestinal injury) during the early postoperative period and in response to enteral feeding and vasopressor treatment.
Methods:
A Seldinger technique was used for percutaneous TD cannulation during an Ivor Lewis esophagogastrectomy. Lymph flow rate and pressure were measured. TD lymph and plasma were sampled at 12 hourly intervals for up to 120 hours after surgery and before TD embolization. Biochemistry, lipids, cytokines, and markers of intestinal injury were measured before and after enteral feeding commenced at 36 hours.
Results:
Intraoperative TD cannulation was technically feasible in three of four patients. Delayed TD embolization was only successful in one of three patients, with two patients requiring a re-thoracotomy to treat chylothorax. Profound changes in TD composition, but not flow rate, occurred over time and in response to enteral feeding and vasopressors. TD lymph compared with plasma had significantly higher lipase (1.4–17 × ), interleukin-6 (8–108 × ), tumor necrosis factor-α (2.7–17 × ),
Conclusions:
Although TD cannulation and lymph sampling were successful, TD embolization failed in two of three patients. The composition of sampled TD lymph changed dramatically in response to enteral feeding, indicating intestinal ischemia that could be exacerbated by nonselective vasopressors. The higher concentration of proinflammatory cytokines and gut injury markers in TD lymph, compared with plasma, lends support to the gut-lymph concept.
Introduction
The “gut-lymph” concept states that lymph draining from the intestine in acute disease undergoes profound compositional changes that contribute to systemic inflammation, organ dysfunction, and worse outcome.1,2 This occurs because this altered gut-lymph bypasses the liver to enter the systemic circulation through the thoracic duct (TD). 3 Up to 70% of the lymph in the TD is gut-lymph derived from the abdomen. In the experimental setting, hypovolemia, in association with acute disease and major surgery, causes reflex splanchnic vasoconstriction and a degree of intestinal ischemia, 4 which in turn can cause gut injury, impairment of gut barrier function, and changes in gut-lymph composition. 5 A significant barrier to the study of gut-lymph composition and its role in disease has been a safe, acceptable, and reliable method of sampling lymph from the TD in human subjects.
An expanding body of experimental evidence, almost exclusively from animal studies, supports the gut-lymph concept.1,2,6 In addition to intestinal ischemia in acute disease, 4 gut dysfunction results in the loss of intestinal mucus, 7 endotoxemia, 8 mitochondrial dysfunction, 9 increased endothelial permeability, 10 altered gut microbiome, 11 and enteral feeding intolerance. 12 Nonocclusive mesenteric ischemia (NOMI) can occur in association with acute and critical illness, 13 and after major surgery. 14 The significant changes in the composition of gut-lymph in a number of acute diseases 1 correlate with disease severity. 15 For example, that levels of several pancreatic proteases in gut-lymph are significantly elevated (up to 40-fold) in acute pancreatitis. 16 In other studies it is has been reported that lipase generates free unsaturated fatty acids in gut-lymph, which are toxic to endothelial cells 17 and are associated with organ dysfunction in vivo. 18 It has also been found that preventing gut-lymph from reaching the systemic circulation in acute diseases can attenuate, if not prevent, the associated cardiac 19 and respiratory dysfunction, 20 reduce bacterial translocation, 21 and improve animal survival.22,23
There is a limited clinical literature supporting the gut-lymph concept. 24 Historically, long-term (>4 weeks) TD lymph drainage has been used to induce immunosuppression in the transplantation setting, and short-term drainage to reduce the inflammatory response. 24 A study in patients with acute pancreatitis reported improved pulmonary function and oxygenation with external TD lymph drainage. 25 Although these historical studies were underpowered and uncontrolled, they did support the concept that TD lymph in acute disease promotes inflammation and organ dysfunction. Despite this limited evidence, equipoise remains and consequently, further clinical studies are required, which will in turn necessitate access to TD lymph in human subjects.
Access to TD lymph for studies can be obtained in three ways: (1) open surgical cannulation of the TD in the left neck26,27 (which can be complicated by wound infection and chyle leak), (2) percutaneous radiological cannulation (either antegrade or retrograde), and (3) opportunistic surgical cannulation, performed during thoracic or neck surgery. One of the common surgical procedures in which the TD is routinely exposed (and ligated) is an Ivor Lewis esophagogastrectomy. Surgical cannulation of the TD cannulation, with delayed TD embolization makes it possible to sample TD lymph for several postoperative days. Esophagectomy patients provide an opportunity to study aspects of the pathophysiology of gut-lymph in the postoperative setting, especially in relation to enteral feeding and the effect of inotropes. These patients are often given enteral feeding through a feeding jejunostomy, which allows a within-subject controlled study of TD lymph composition changes while investigating the transition from the fasted to fed state. The role of hyperosmolar enteral feeding in the development of NOMI, 28 thought to be owing to the increased metabolic demand on blood supply, can also be studied in this setting. Enteral feeding can induce ischemia, especially in the context of hypovolemia and persisting reflex splanchnic vasoconstriction.29,30 Another opportunity is to study the effect of vasopressors (including noradrenaline) in causing ischemic injury of the intestine28,31–33 by increasing splanchnic vasconstriction. The effect of the combination of early enteral feeding and inotrope use in the postoperative period is also worth studying.
The aims of this study were to develop and pilot a technique of intraoperative TD cannulation (and delayed embolization) and to serially measure TD lymph pressure, flow, and composition (including markers of intestinal injury) during the early postoperative period and in response to enteral feeding and vasopressor treatment.
Methods
Patient recruitment
All patients undergoing an Ivor Lewis esophagogastrectomy at our institution were eligible for inclusion. The only exclusion criterion was a previous neck dissection or TD intervention. Four patients undergoing Ivor Lewis esophagogastrectomy for adenocarcinoma of the distal esophagus at Auckland City Hospital by two surgeons (J.A.W., G.B.) were recruited and gave written consent for intraoperative TD cannulation. Ethical approval for the study was obtained from the national Health and Disability Ethics Committee (12/NTB/67).
Cannulation
To increase intraoperative lymph flow and facilitate TD identification before cannulation, patients were administered either 50 mL of olive oil (patients 1 and 2) or 200 mL of dairy cream (patients 3 and 4) by infusion through the jejunostomy feeding tube (12 Fr silastic Foley catheter; C.R. Baird, Inc., Covington, GA) immediately before repositioning the patient for the right thoracotomy.
The TD was identified as it ran on the aorta, 3–4 cm caudal to the azygous vein, and proximal to where it crossed over to the left side of the patient. It was isolated, looped, and ligated. Caudal to the ligation a small transverse ductotomy was performed with fine scissors, assisted by loupe magnification. A Tuohy needle was used to insert a 5 Fr cholangiography catheter (Endoscopic Cholangiography Set, ESC 500 Tuohy; Cook Medical, Bloomington, IN) with a fixed core guidewire (G00650; Cook Medical) through the skin and chest wall tissues of the lateral intercostal space one level above the thoracotomy incision. This allowed the catheter and guidewire to approach the TD “in-line.” The caudal end of the TD was cannulated through the ductotomy using a Seldinger technique with the guide wire inserted ∼10–20 cm, over which the catheter was passed. The catheter was secured with two ligatures around the TD, and the redundant intrathoracic portion of the catheter withdrawn to allow the catheter to lie against the lateral thorax so as to not impede subsequent lung expansion. The catheter was also secured by suture to the skin, curled up, and dressed (Tegaderm; 3M Health Care, St Paul, MN). The catheter was connected to sterile saline primed pressure tubing (Edwards Lifesciences TruWave 3cc; Haina, San Cristobal, Dominican Republic) through a ureteric catheter connector (Cook Medical). The tubing was passed off the sterile field and connected to the three-way stop-cock included in the pressure tubing kit to allow for lymph collection during the thoracotomy and afterward. In between sampling periods, this set up occluded flow in the cannulated TD (Fig. 1).
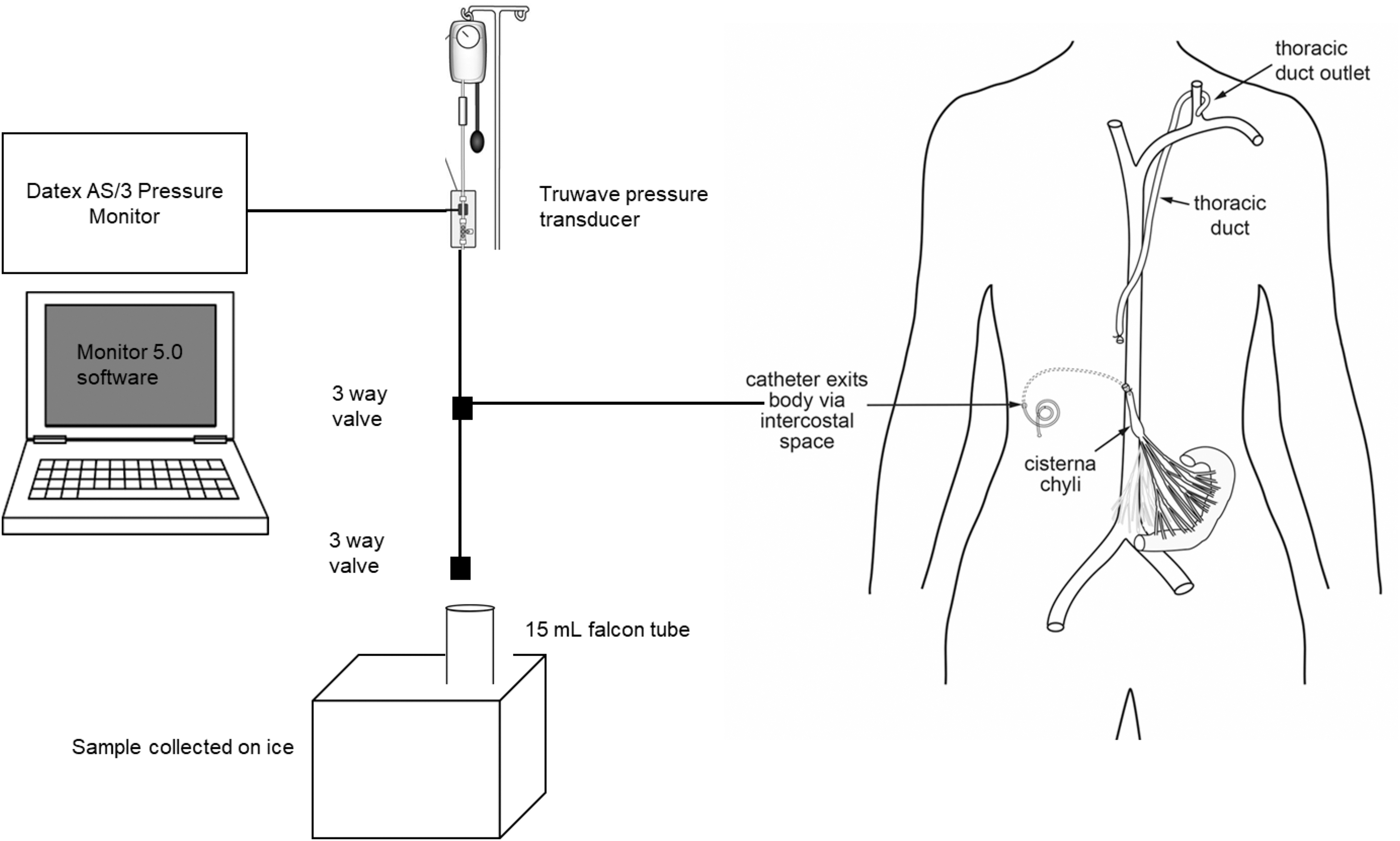
Schematic representation of the operative TD cannulation, pressure monitoring and lymphatic drainage apparatus. TD, thoracic duct.
Lymph collection
Collecting TD lymph was facilitated by opening the three-way stop-cock at the end of the pressure tubing to air and closing it at the manometer end. The saline in the pressure tubing was discarded. Lymph was then collected directly into 15 mL tubes (Greiner Bio-one, Rainbach, Austria) directly on ice. TD lymph was collected for an hour intraoperatively and then the following morning for 2 hours (0700–0900 hours) and the evening for an hour (1900–2000 hours) (Fig. 2). The TD lymph collection period was subdivided into 15-minute intervals to alternate the collection of lymph into “neat” 15 mL tubes and 15 mL tubes containing 370 μL of ethylenediaminetetraacetic acid (EDTA; 40 ng/mL) (Life Technologies) for compositional analysis. At the end of each 15-minute collection period the volume produced was recorded. These volumes were then summed to calculate the volume of lymph collected during each hour of collection. After each collection period the pressure tubing was disconnected from the TD catheter at the ureteric catheter connector and was occluded (Fig. 1) by a SmartSite valve (Becton, Dickson and Company, Franklin Lakes, NJ). This intentionally occluded the TD lymph flow between collecting periods for 10 (after the morning collection) or 11 (after the evening collection) hours, respectively.
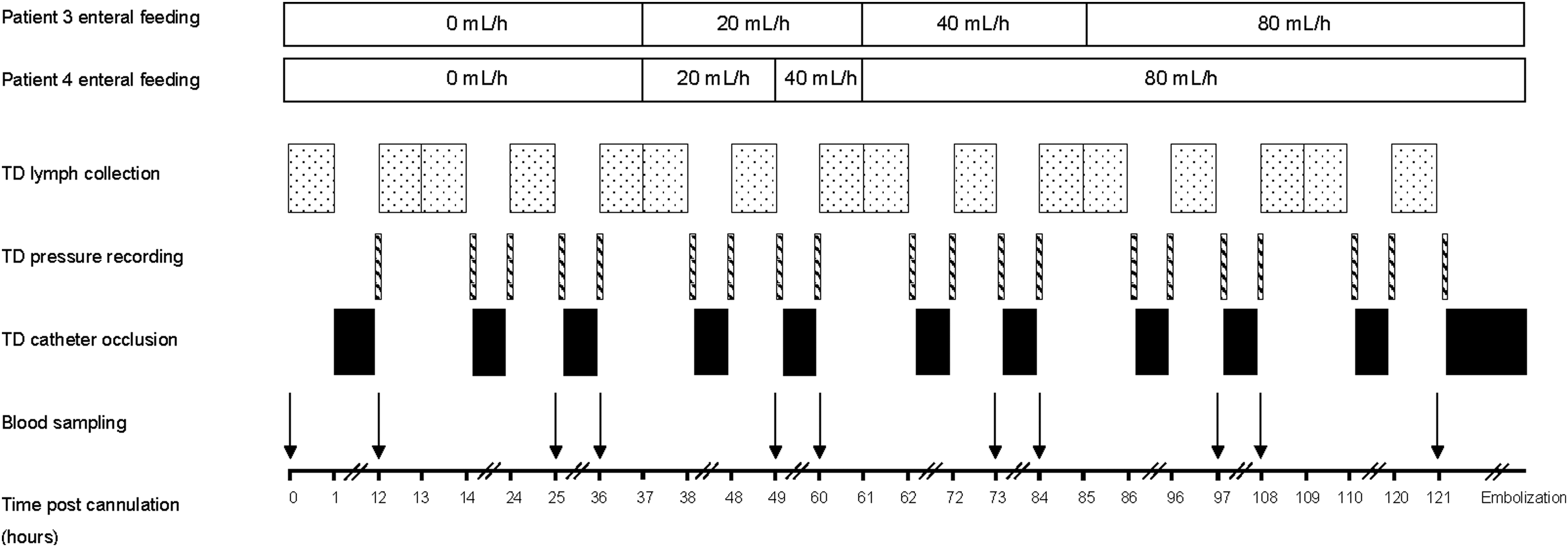
The study protocol showing the timing of TD lymph collection (for 1- or 2-hour intervals), TD pressure recording (for 15-minute intervals), TD catheter occlusion (for 10- or 11-hour intervals), TD embolization and blood sampling (matched to before and after lymph sampling), as well as the EF rates for patients 3 and 4. EF, enteral feeding.
Matched peripheral blood samples (10 mL) were taken at 0700 and 2000 hours using the radial arterial line. For plasma 5 mL went into K2 EDTA vacutainer (10.8 mg); for serum 5 mL into silica-coated serum vacutainer (Becton, Dickson and Company) (Fig. 2). This timing coincided with scheduled lymph collection, thus providing matched blood and lymph samples. The TD lymph and plasma were centrifuged at 1500 g for 10 minutes then at 3000 g at 4°C for 10 minutes before being stored in 1.5 mL microcentrifuge tubes (Axygen, Union City, CA) at −80°C. TD lymph and plasma were collected intraoperatively, in the High Dependency Unit and on the surgical ward. Cannulation of the TD was not possible in patient 2, and no lymph was collected.
Enteral feeding
Enteral feeding with Nutrison Standard (1.0 kcal/mL; 3.9 g fat per 100 mL; 0.6 g medium chain fatty acid per 100 mL) (Wuxi, Peoples Republic of China) was gradually introduced from the second postoperative day with rate increases at 0800 hours.
Vasopressor therapy
Noradrenaline (0.1 mg/mL) at a rate of 0.1–1.0 mg/h was administered in the high dependency unit to maintain a mean arterial blood pressure greater than 70 mmHg. This was only necessary for patient 4.
Embolization
At the conclusion of lymph collection and after a lymphangiogram through the catheter, the TD was embolized by an interventional radiologist (A.H.H., B.N.C.) in the Digital Subtraction Angiography suite. Embolization used a Progreat microcatheter (Terumo International Systems, Somerset, NJ) inserted down the TD catheter to facilitate the deployment of a series of tightly packed platinum microcoils (Nester/Tornado Embolization Coil, Cook Medical). A completion lymphangiogram was performed to confirm that contrast did not leak cephalad to the coil nests.
Laboratory methods
Concentrations of standard biochemical analytes were measured in plasma and neat TD lymph samples for patients 3 and 4 on a Hitachi 902 Autoanalyzer (Hitachi High Technologies Corp., Tokyo, Japan) using various methods: enzymatic colorimetric (glucose, triglyceride, cholesterol, and lipase); immunoturbidimetric (apolipoprotein A-1 [APOA1], apolipoprotein B [APOB]); enzyme-linked kinetic ultraviolet (alanine transaminase [ALT], aspartate aminotransferase [AST], lactate dehydrogenase [LDH]); kinetic UV (urea); homogenous enzymatic colorimetric (gamma glutamyltransferase [GGT], high-density lipoprotein [HDL], low-density lipoprotein [LDL]); kinetic colorimetric (creatinine); colorimetric (total protein, albumin); Diazo colorimetric (bilirubin); UV-test (creatine kinase [CK]); and direct potentiometric using ion selective electrodes (electrolytes). All the reagents were purchased from Roche (Mannheim, Germany).
Concentrations of proinflammatory cytokines interleukin 6 (IL-6) and tumor necrosis factor alpha (TNF-α) were measured in plasma and neat TD lymph for patients 3 and 4 using the MILLIPLEX MAP Human Cytokine/Chemokine Magnetic Bead Panel kit (Cat. No. HCYTMAG-60K-PX29; EMD Millipore Corp., MA) on a MAGPIX instrument using xPonent software (Luminex Corp., Austin, TX).
The plasma and neat lymph levels of biomarkers of gut injury were determined for patients 3 and 4 using commercial kits in accordance with the manufacturer's instructions:
Results
Technique of TD cannulation and sampling
The results of TD cannulation, lymph collection and TD embolization, length of stay and complications are summarized in Table 1. Intraoperative TD cannulation during Ivor Lewis esophagogastrectomy was successful in three of the four cases. In patient 2 the narrow caliber of the TD lumen prevented cannulation with the guide wire and the procedure was abandoned. The technique increased the length of the operation by a mean of 20 minutes. Of the three cases that were successfully cannulated, TD lymph was sampled postoperatively for 3 (patient 1), 4 (patient 4), and 5 (patient 3) days.
Summary of Intraoperative Thoracic Duct Cannulation, Duration of Postoperative Lymph Sampling, and Results of Thoracic Duct Embolization
N/A, not applicable; TD, thoracic duct.
Technique of TD embolization
Patient 1 had TD embolization on the third postoperative day with a total of eight coils (3 × MWCE-18S-7/3 Tornado; 5 × MWCE-18-14-3-Nestor). The completion lymphangiogram (Fig. 3A) did not demonstrate any extravasation of contrast, and the catheter was removed immediately. The following day a left pleural effusion developed. A computed tomography (CT) scan with oral contrast did not reveal any evidence of an anastomotic leak. Ultrasound-guided aspiration confirmed a chylothorax. Conservative treatment of the chylothorax was attempted by switching enteral feeding to medium chain triglyceride (Monogen; Nutricia, Fulda, Germany) for a week, and then a trial of nil by mouth and parenteral nutrition. When this failed to resolve the chylothorax, the patient had a second thoracotomy on postoperative day 14. The chyle leak at the site of TD cannulation was identified and suture ligated.
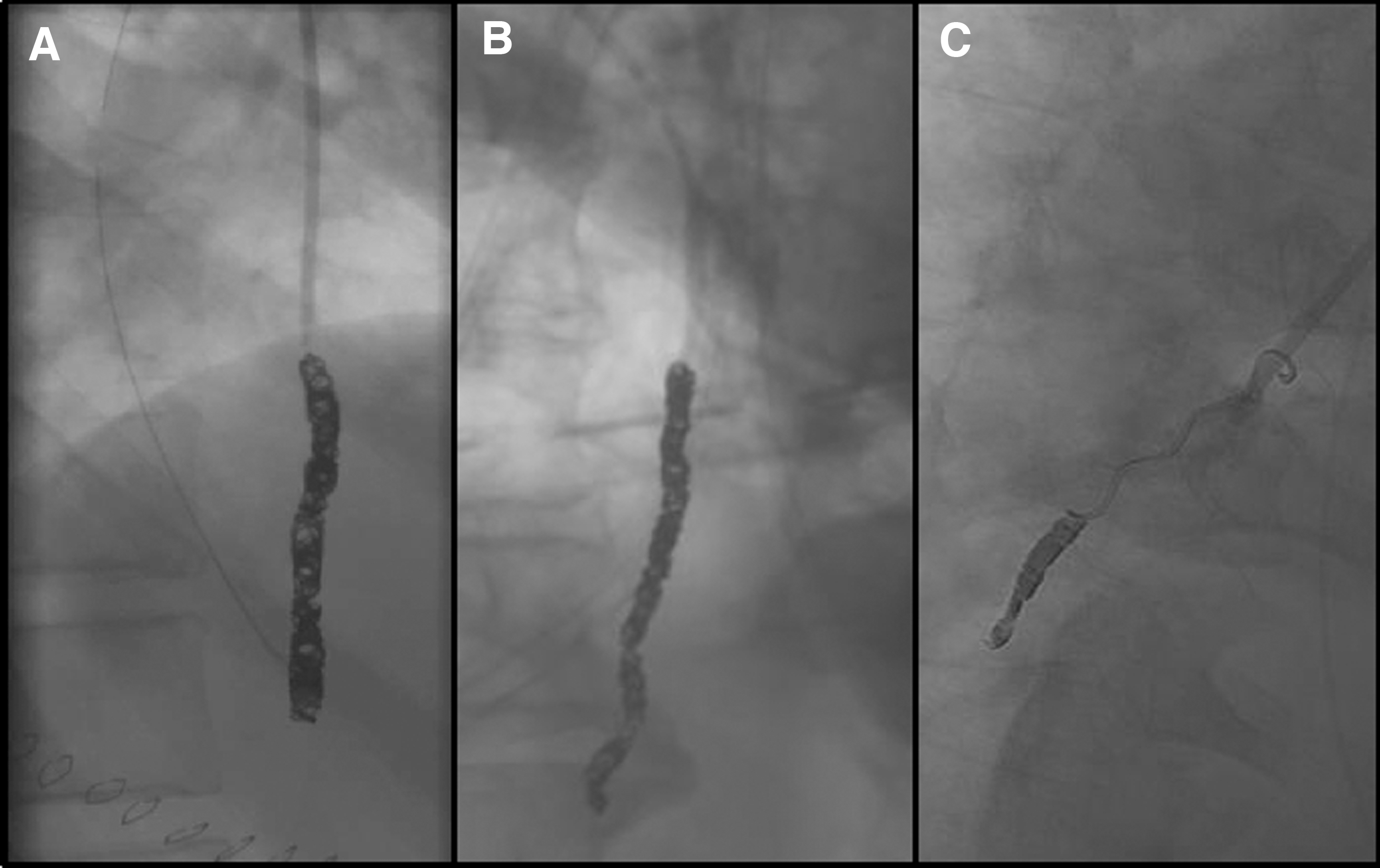
TD lymphangiograms following embolization for patients 1
Patient 3 had TD embolization 8 days after the operation using 11 coils (1 × MWCE-18S-7/3 Tornado; 7 × MWCE 35-7-4 Nestor; 2 × MWCE 18-14-4 Nester; 1 × MWCE 18-14-3 Nester). The chest drain (19 Fr Blake) had been retained because of the experience with the first case. The completion lymphangiogram did not demonstrate any flow of contrast beyond the microcoils (Fig. 3B), but the catheter was not removed for a further 48 hours. A small right pleural effusion was aspirated the following day but showed no signs of a chylothorax.
Patient 4 developed a chylothorax 5 days after resection, which was initially managed by the retained operative chest drain. This was before any attempt at TD embolization, which was attempted on the 6th day after the operation. The initial lymphangiogram demonstrated that the catheter had migrated out of the TD by ∼8 cm because the suture had loosened at skin level allowing the catheter to inadvertently be withdrawn. The interventional radiologist was able to place a microcatheter into the TD and a further lymphangiogram confirmed successful TD cannulation. Two microcoils were successfully deployed but while attempting a third coil, the microcatheter migrated out of the TD. Despite repeated attempts at cannulation no further microcoils could be deployed (Fig. 3C). The chylothorax persisted and required a re-thoracotomy for TD ligation at the site of cannulation.
Complications of TD cannulation and embolization
Two of the four patients developed a chylothorax requiring a re-thoracotomy. Patient 1 failed TD embolization because only three coils were used, which was at variance with the agreed protocol. Patient 4 developed a chylothorax before TD embolization because the catheter had migrated out of the TD and it was not possible to introduce more than two coils. The other complications that occurred in the four patients are summarized in Table 1. The most serious complication was an anastomotic leak in patient 4. This became clinically apparent 24 hours after the re-thoracotomy and surgical ligation of TD. This resulted in a prolonged intensive care and hospital stay (46 days). Both patients have been followed up for 36 months.
TD lymph pressure and flow
The hourly volume of lymph flow is given in Table 2. When the hourly flow rate of the patients was subdivided into 15-minute periods, the highest flow rate was found immediately after release of the occlusion on 15/22 (68%) of the study sampling periods. In the first hour of the morning and the evening, collection periods tended to be on average 11% higher (excluding one outlying values from patient 4) than second hour in the morning when the TD catheter had already been open for an hour. For patient 3 there was no collection at hour 13 postcannulation owing to a temporary blockage of the TD catheter that was subsequently unblocked with a 5 mL (50 IU) heparin flush. The striking finding was that there was no increase in TD lymph flow with the commencement of enteral feeding (Fig. 3). TD pressure fell from a range of 80–110 mmHg at the beginning of sampling to between 10 and 20 mmHg at the end of the sampling period.
Hourly Volumes (mL/h) of Thoracic Duct Lymph Collected from Patients 3 and 4
Enteral feeding
Enteral feeding through a tube jejunostomy was commenced on the second postoperative morning at 0800 hours in patients 2, 3, and 4 only. Enteral feeding for patient 1 did not commence until after TD embolization on the third postoperative day. The rates of enteral feeding are given in Figure 1. The rate of increase was more rapid in patient 4, which meant there was only one TD lymph sampling at the 40 mL/h rate. Both patients 3 and 4 had received 24 hours of enteral feeding at the peak rate (80 mL/h) before discontinuation of TD lymph sampling on days 5 and 4, respectively.
TD lymph compositional analysis
Biochemistry results
Compositional analysis was performed on the TD lymph sampled from patients 3 and 4 only. The plasma and TD lymph results before and after the commencement of enteral feeding for each biochemical assay are given in Table 3. The electrolytes sodium, chloride, and glucose showed minimal variation with commencement of the enteral feeding. Creatinine and urea showed little variation between the plasma and lymph compartments, but both peaked on the first postoperative day.
Plasma And Lymph Values for Biochemical Analytes (Mean ± Standard Deviation) Before and After the Introduction of Enteral Feeding in Patients 3 and 4
The most significant findings are highlighted in Figures 4–7. These show differences between the lymph and plasma compartments that occur with the commencement of enteral feeding. Total protein and albumin levels were notably lower in TD lymph than plasma throughout the postoperative period (Fig. 5). Postoperatively albumin levels fell in both the plasma and TD lymph (Fig. 6). The measurements of liver function were generally higher in plasma than TD lymph, although they exhibited a mixed picture with both transaminases (AST and ALT) decreasing immediately postresection, whereas GGT increased after the introduction of enteral feeding in patient 3. Lipase was notably higher in TD lymph compared with plasma. Over the sampling period lipase was 1.4–17-fold greater in the lymph (Fig. 7), with the lymph values in patient 3 being above the normal plasma reference range (16–67 U/L). The changes in creatine kinase levels were different between patients 3 and 4 (Fig. 6); however, TD lymph values in both patients were above the normal plasma reference range (38–176 U/L).
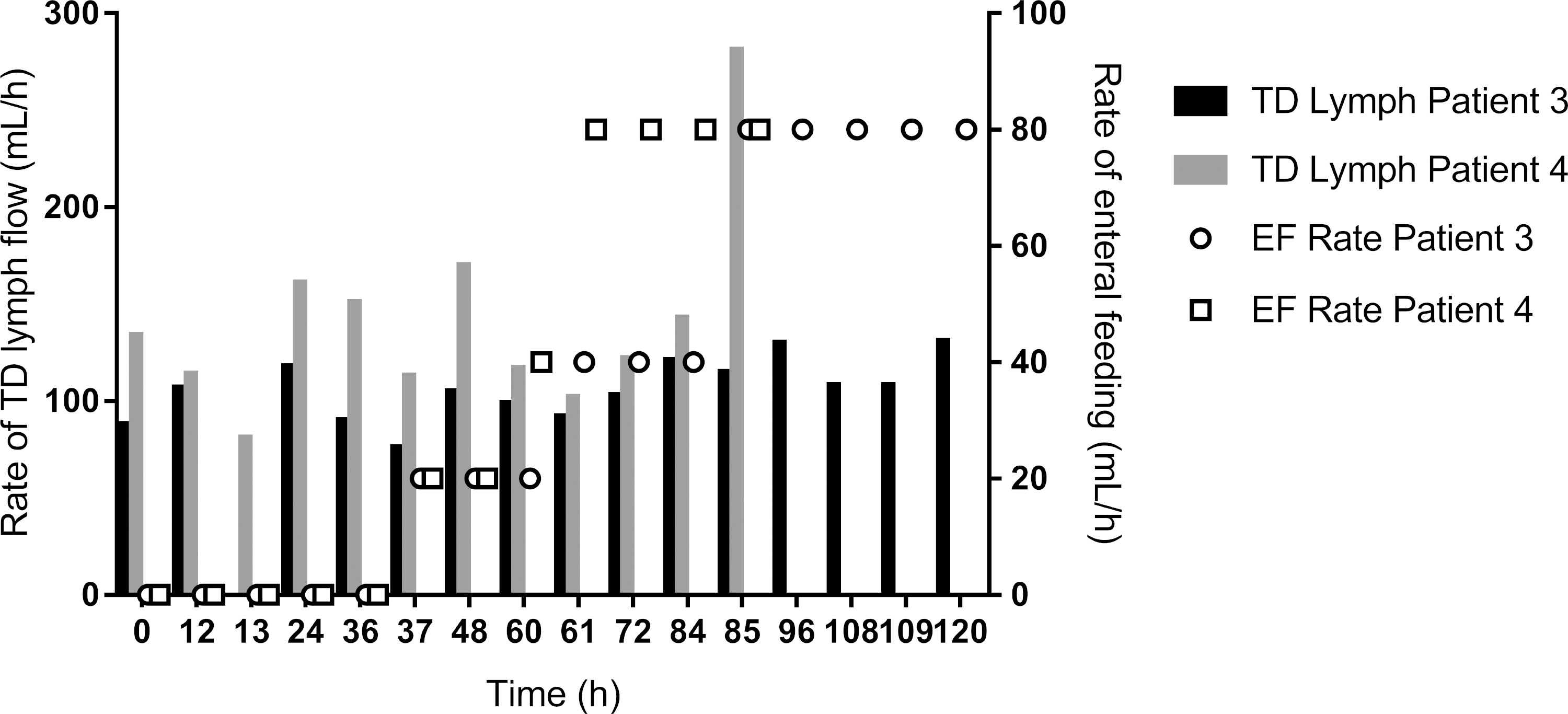
Demonstrates that the rate of TD lymph flow (mL/h) is unaffected by the increased rate of EF (mL/h) in postoperative period for patients 3 and 4.
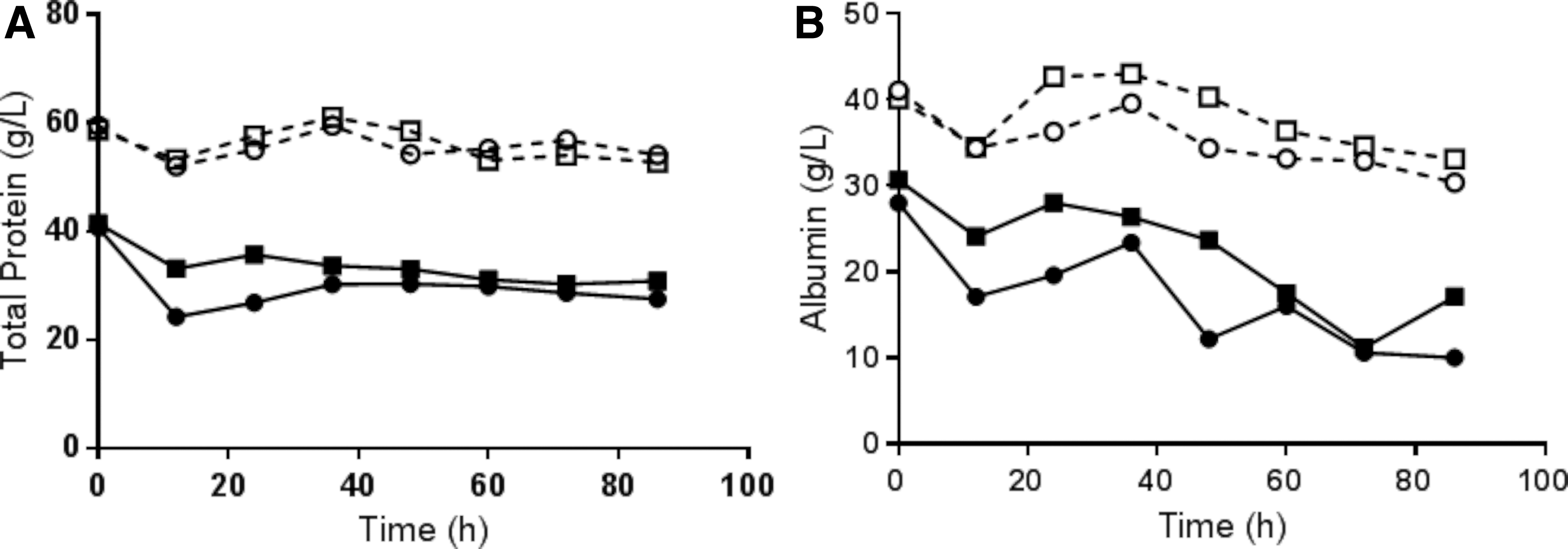
Postoperative total protein (g/L)
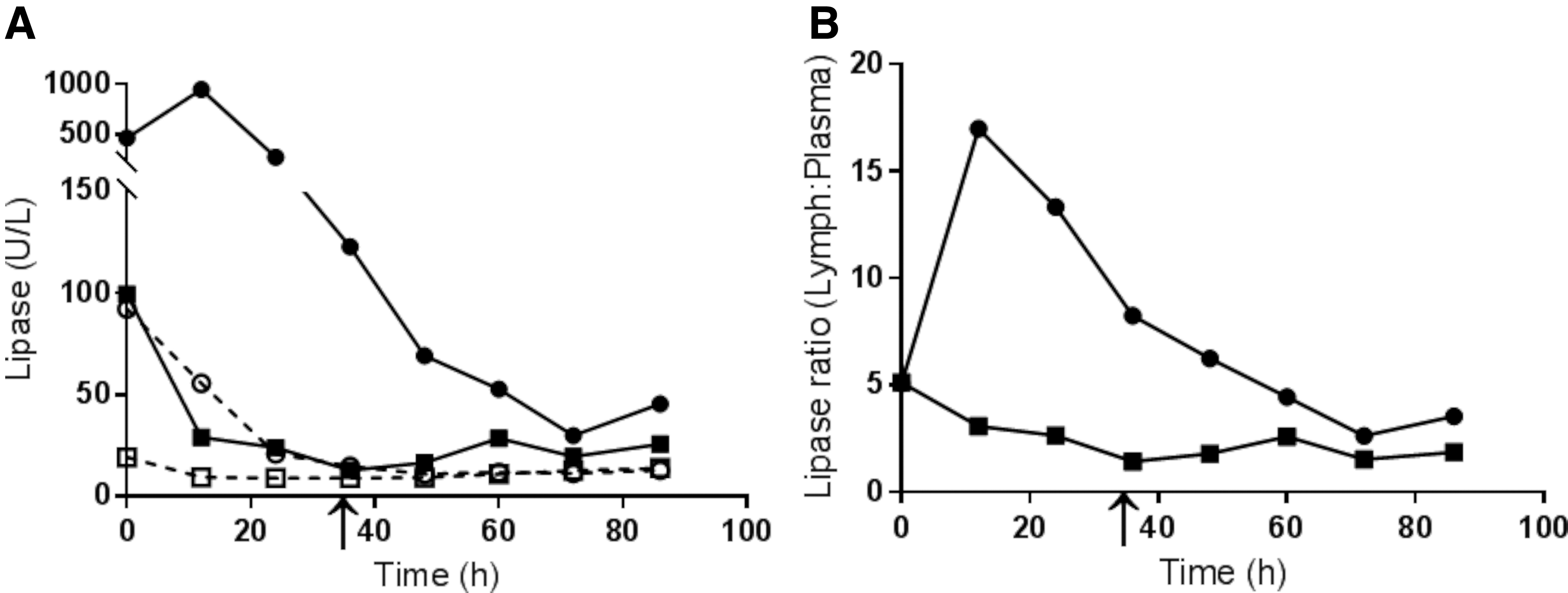
Postoperative lipase (U/L) in plasma (dotted line) and TD lymph (solid line) for patients 3 (circles) and 4 (squares)
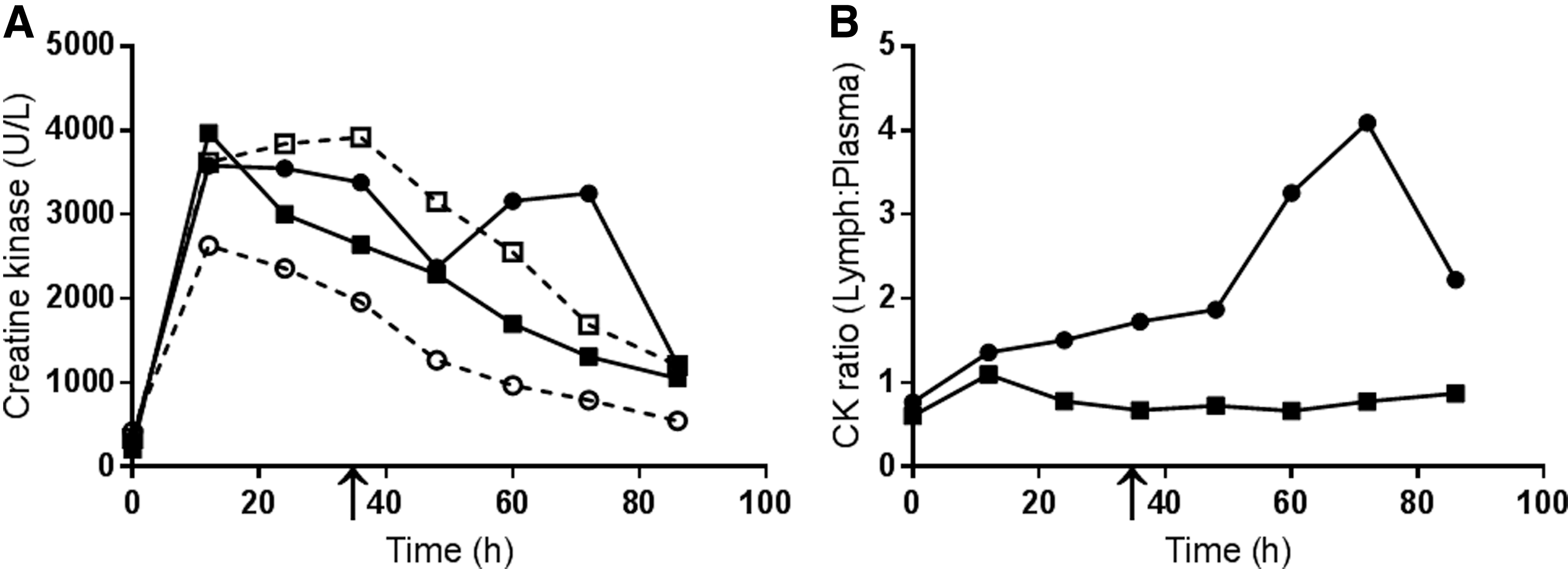
Postoperative serial creatine kinase (U/L) measurement in plasma (dotted line) and TD lymph (solid line) for patients 3 (circles) and 4 (squares)
Lipid results
Triglyceride level was the only lipid found at higher concentration in the TD lymph than plasma at every time point except before the commencement of enteral feeding (Fig. 8). When enteral feeding was commenced the triglyceride level in the TD lymph dramatically increased to a peak of 13.8-fold (patient 3) and 9.2-fold (patient 4) higher once enteral feeding reached a peak of 80 mL/h. The other lipids were all consistently higher in plasma than in lymph and did not change with the commencement of enteral feeding, with all showing a steady decline in plasma levels postresection.
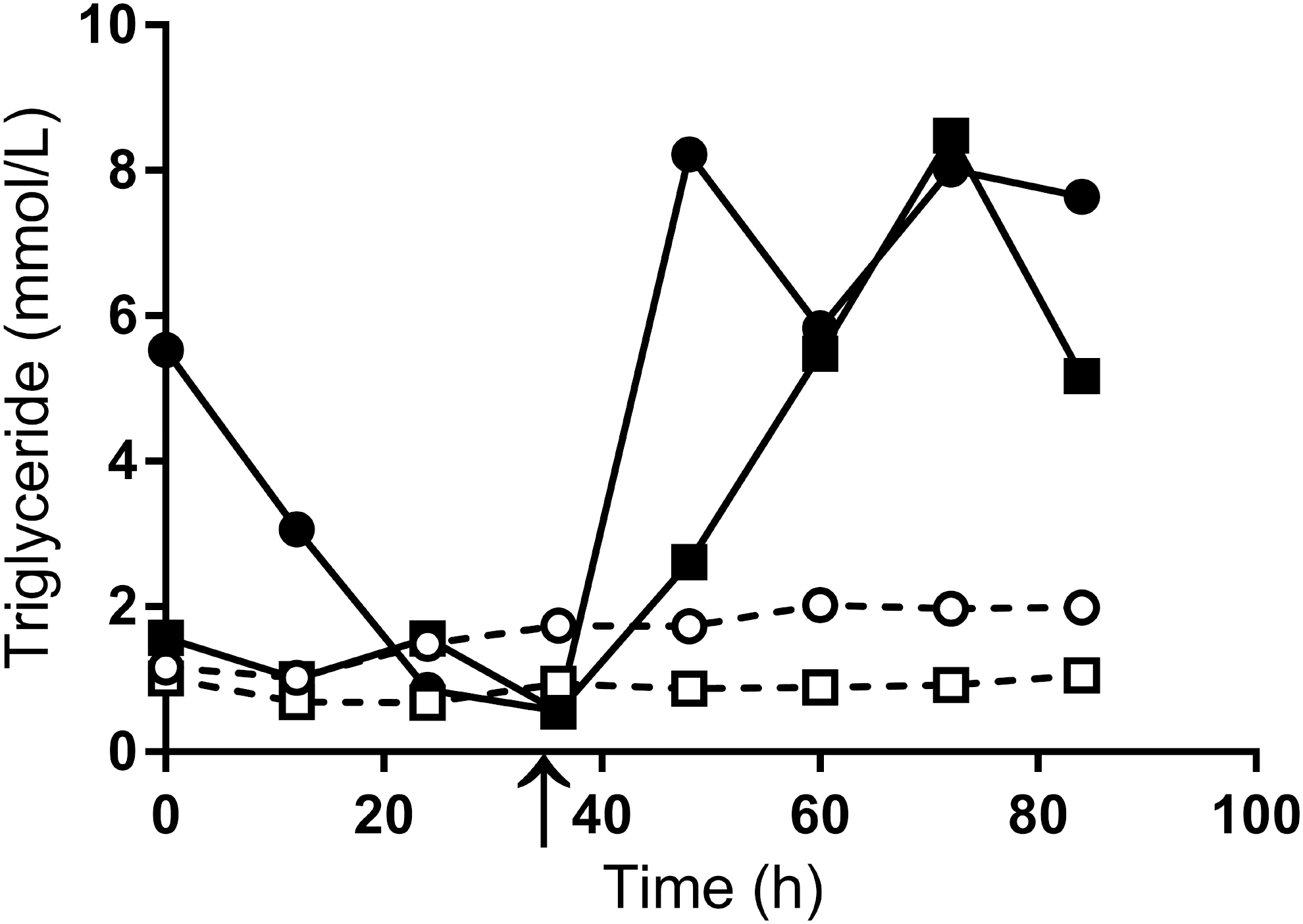
Postoperative triglyceride level (mM) in plasma (dotted line) and TD lymph (solid line) for patients 3 (circles) and 4 (squares) over the elapsed time after cannulation. The arrow marks the introduction of EF.
Cytokine results
Both the proinflammatory cytokines IL-6 and TNF-α were found in much higher concentrations in TD lymph than plasma (Fig. 9A, B). TNF-α demonstrated a bimodal peak, with the second peak occurring after enteral feeding was commenced (Fig. 9B). The lymph-to-plasma ratio for IL-6 was 8:1 to 108:1 over the sampling period (Fig. 9C), and the ratio for TNF-α was 2.7:1 to 17:1 (Fig. 9D).
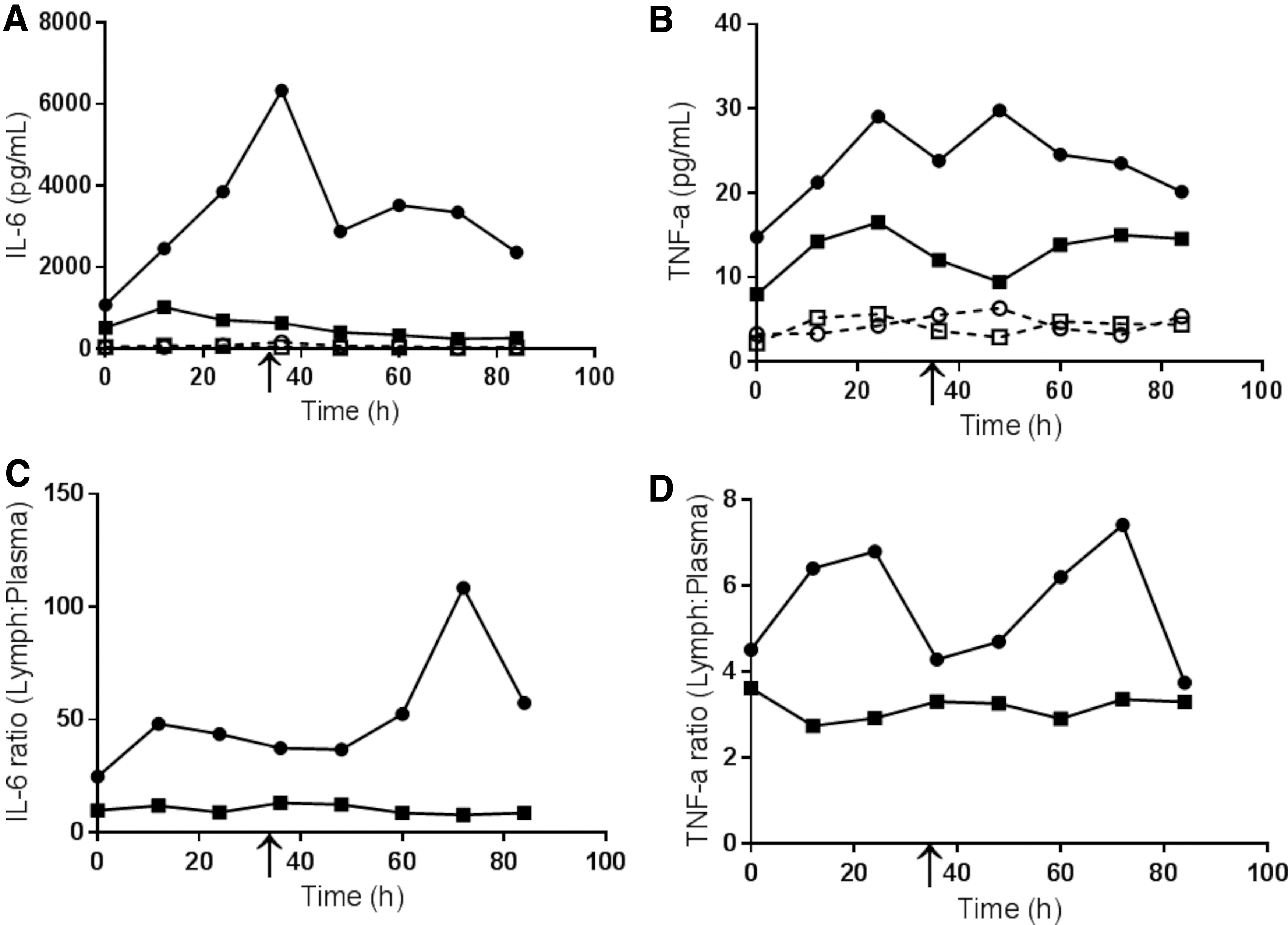
Change in the measurement of proinflammatory cytokines IL-6 (pg/mL)
Markers of intestinal injury
The highest levels of bacterial derived
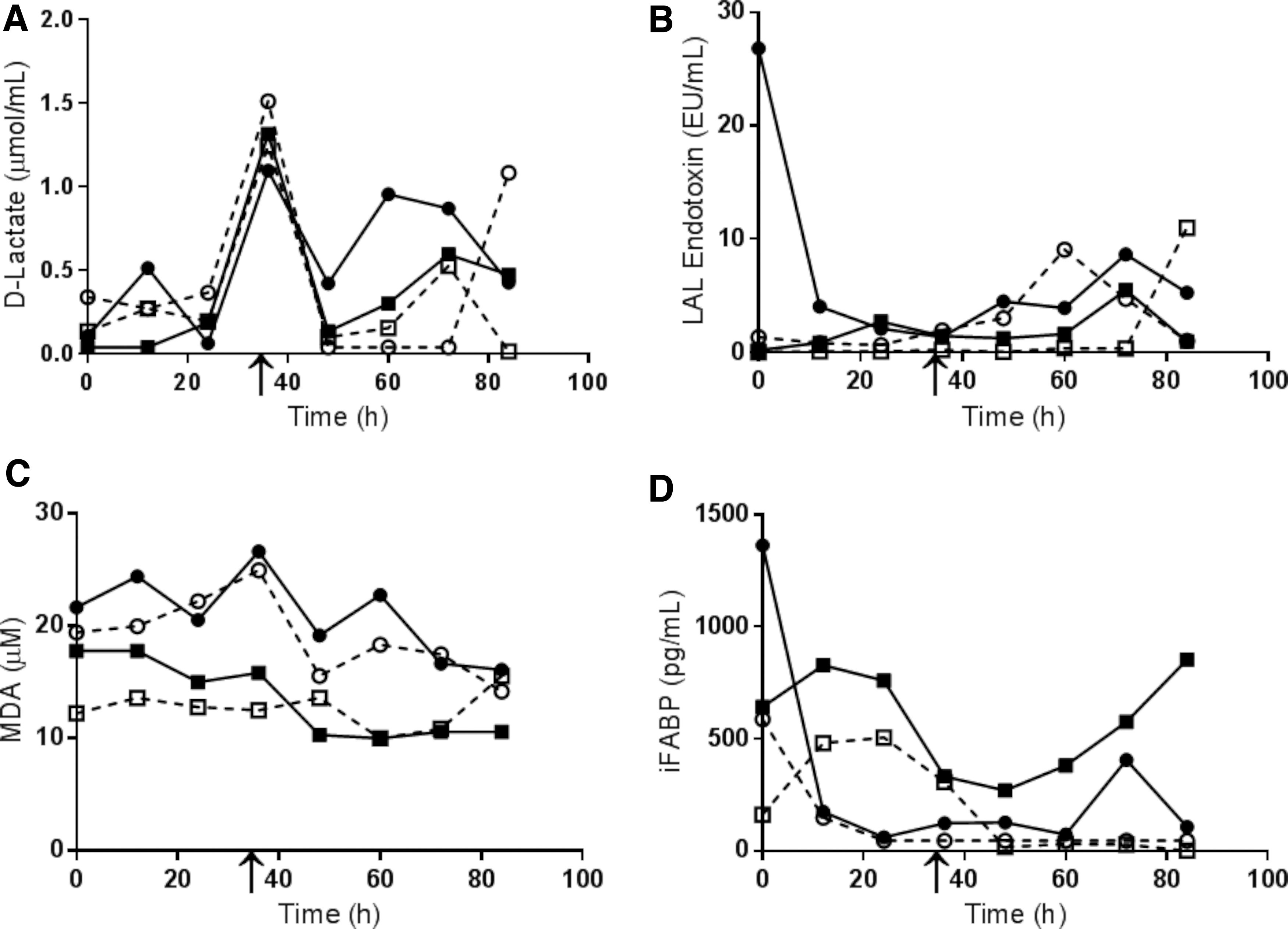
Markers of gut dysfunction in plasma (dotted line) and TD lymph (solid line) for patients 3 (circles) and 4 (squares) over the elapsed time after cannulation.
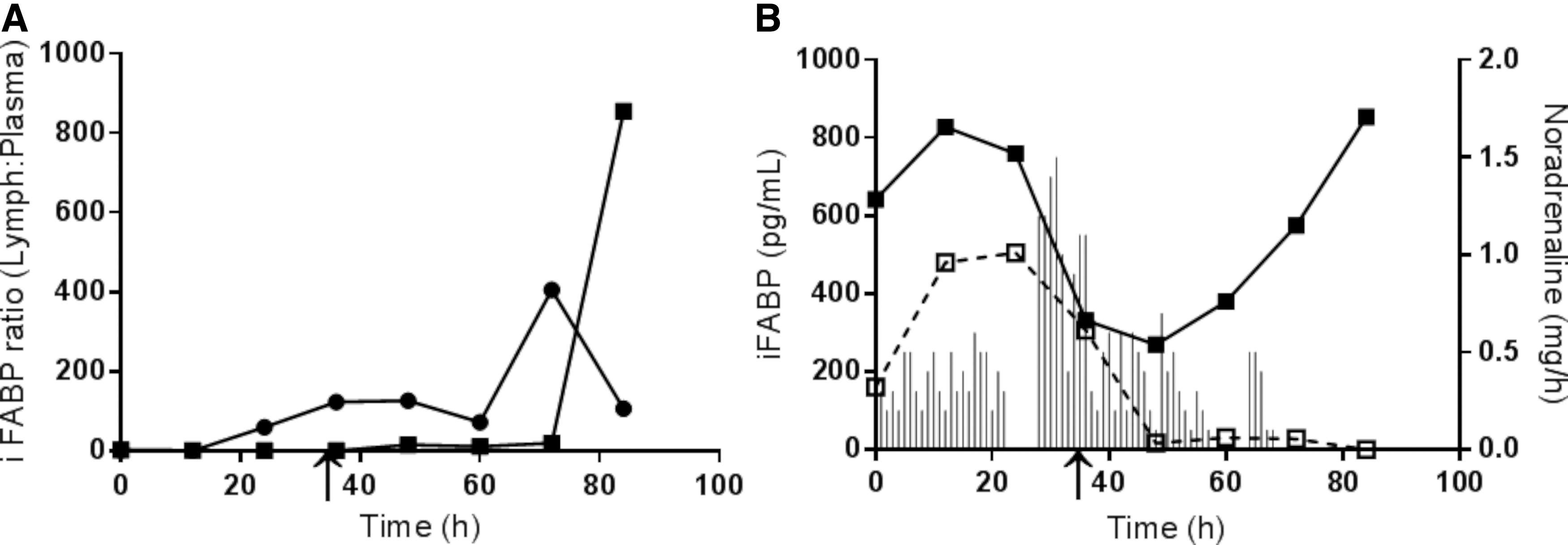
iFABP assay ratio of TD lymph-to-plasma iFABP for patient 3 (circles) and patient 4 (squares) plotted against time in
Discussion
This study details the pilot of a new operative technique of TD cannulation and delayed embolization to allow access to TD lymph for longitudinal sampling in patients undergoing esophagectomy. This was technically feasible in the three of the four patients. This study provides the first evidence of changes in TD pressure, flow, and composition after major surgery and in response to enteral feeding and vasopressor treatment. The principle of cannulating and sampling TD lymph close to its origin has demonstrated that TD lymph, largely derived from gut lymph is markedly different from plasma.1,2 The composition of sampled TD lymph changed dramatically in response to enteral feeding, with some signs indicating a degree of underlying intestinal ischemia. The higher concentrations of proinflammatory cytokines and markers of gut injury in lymph (compared with plasma) provides further clinical support for the gut-lymph concept.
The most important outcome of this pilot study was that two patients developed a chylothorax that required re-thoracotomy. The risk of failed TD embolization based on that experience was deemed too high, and it was appropriate that the study was terminated early. A critical analysis of the reasons for the failure of the TD embolization technique suggests that they were both preventable. In patient 1 there was an insufficient number of tightly packed coils inserted, and this was an unintentional breach of the agreed protocol. In patient 4 there was migration of the catheter because of a failure of the skin fixation stitch and failure to check for this problem. If the catheter had not migrated, it was reasonable to expect that sufficient number of coils could have been successfully deployed based on our experience with patient 3.
The intraoperative failure of initial TD cannulation in patient 2 was related to the TD anatomy. The narrow caliber TD could not be cannulated, raising the possibility of a dual TD. A recent literature review highlighted the range of anatomical variations in the commencement, course, duplicity, and termination of the TD. 3 The presence of multiple TD channels in the upper thorax was estimated at 28% in a large cadaveric study. 34 The variations in TD anatomy suggests that prior imaging of the TD may help identify patients in whom TD cannulation may prove difficult.
The study design of TD occlusion and intermittent sampling meant that there was a pressure build-up in the TD between sampling periods. The highest TD pressures were recorded immediately before sampling and the highest flow rates in the first 15 minutes of sampling. It was expected that lipid-rich enteral feed would increase TD lymph flow, 35 as this is the primary route of absorption, but this did not occur even at the peak feeding rate of 80 mL/h. Intravenous fluid and inotropic therapy did not appear to affect TD pressure and lymph flow, despite evidence of this in animal models. 36 Although the sample size of this study is too small to make any meaningful statistical conclusions regarding changes in pressure and flow, it would appear that the effect of TD occlusion masked any effect on pressure and flow from the introduction of enteral feeding or vasopressor therapy. In dogs increases in TD pressure have resulted in reductions to the lipid content of TD lymph. 37 It has previously been suggested that the backpressure from TD occlusion may temporarily reduce the production of gut lymph (and hence mitigate the effect of enteral feeding) until collateral flow to the systemic circulation develops. 38
The changes in composition of TD lymph compared with plasma are consistent with the gut-lymph concept. The higher concentration of markers of both gut injury and dysfunction and the proinflammatory cytokines in the lymph compared with plasma is consistent with altered gut-lymph contributing to the systemic inflammatory response after surgery. The changes in TD lymph composition after the commencement of enteral feeding are consistent with its potential role in promoting intestinal ischemia especially in the context of hypovolemia, when the metabolic demand of the hyperosmolar feed may result in inadequate mucosal blood supply. 13
The activation of pancreatic proteases is an important early pathophysiological event in acute pancreatitis and has been linked to the generation of reactive oxygen species, the activation of neutrophils and other proinflammatory mediators.39–41 In 1960 Dumont et al. 42 observed that both amylase and lipase were taken up into the TD from pancreatic interstitial fluid. Subsequently TD lymph from both human 43 and animal 44 subjects with acute pancreatitis has demonstrated higher concentrations of amylase and lipase than plasma. A proteomic analysis of mesenteric lymph from rats with acute pancreatitis compared with a sham model showed a significant increase, in some cases up to 40-fold, in the concentration of seven pancreatic proteases. 16 The presence of lipase in lymph from an experimental hemorrhagic shock model converts lymph to a cytotoxic fluid by the generation of free fatty acids. 17 Proteases have been implicated in the development of acute lung injury in critical illness. 45 The up to 17-fold increase in TD lymph lipase in this study confirms significant pancreatic enzymatic uptake into TD lymph.
Both the proinflammatory cytokines, TNF-α and IL-6, have a key role in the response to injury (surgery) and in mediating the inflammatory response. TNF-α is predominantly produced by activated macrophages and T lymphocytes into active membrane associated (26 kDa) and soluble (17 kDa) forms. 46 It mediates its proinflammatory effects through the vascular endothelium and endothelial leukocyte interactions. 46 IL-6 encompasses a family of cytokines that are released in response to tissue injury or an inflammatory stimulus to mediate the acute phase response. IL-6 also induces the production of immunoglobulin by B cells, the differentiation of T cells, endothelial cell activation, platelet production, and hematopoesis. 47 Both cytokines have previously been measured in human TD lymph in patients with systemic inflammation and multiple organ dysfunction syndrome (MODS).48–50 In 6 patients with acute pancreatitis that had TD lymph externally drained for up to 8 days, the lymph TNF-α concentration was identical to that of plasma, but the IL-6 concentration was on average 1.3 times greater in TD lymph. 50 A small case series of four patients with MODS reported lower levels of IL-6 and TNF-α in TD lymph. 48 Our own study found higher levels of both IL-6 and TNF-α in TD lymph with a second peak in both cytokines in patient 3 after the introduction of enteral feeding. The nature of our study precludes us from determining whether the stimulus that increased these cytokines is related to esophagogastrectomy, to enteral feeding, or other factors such as infection or vasopressors. However, the higher concentration of proinflammatory cytokines in TD lymph contributes further evidence to the role of gut-lymph in mediating the inflammatory response.
As a marker of intestinal permeability, 55 the LAL endotoxin assay was developed to detect gram-negative lipopolysaccharide, the presence of which activates the innate immune system. 55 The increase of endotoxin in both TD lymph and plasma after the commencement of enteral feeding indicates an unexpected exposure to gram-negative bacteria. The basis for this is unclear but likely represents a previously unrecognized loss of barrier function owing to the metabolic stress of enteral feeding. The observed difference between the TD lymph and plasma could either represent preferential bacterial transport through lymph or may reflect different endotoxin clearance mechanism or different concentrations of anti-endotoxin antibodies present in TD lymph and plasma.
The TBARS assay was developed to detect MDA, a product of lipid peroxidation and a marker of exposure to free radicals. 56 It is not a particularly sensitive assay because of the complexity of metabolism of in vivo biological samples. The MDA concentration was higher in TD lymph than plasma, but was not affected by the commencement of enteral feeding.
iFABP is an intracellular protein found in enterocytes of the small and large intestine. It is usually undetectable in plasma but rapidly rises with enterocyte injury, 57 especially intestinal mucosal ischemia. Its application to clinical practice has been limited by its sensitivity, with wide variations in the plasma levels. 58 In this study, it was significantly elevated in lymph, so it is possible that the metabolic demand of enteral feed on the enterocytes lead to enterocyte injury and iFABP release into this compartment. In cardiac intensive care patients, a negative laparotomy for presumed ischemia was associated with higher levels of iFABP compared with those who required resection for intestinal infarction. 14 This suggests that iFABP may be a better marker of early than established ischemia. In this study it was significantly higher in TD lymph than plasma and was bimodal. The first iFABP peak reported in this study on day 0 is probably secondary to major surgery-induced enterocyte injury. This second iFABP peak (day 3) might be owing to the commencement of enteral feeding. It might also be because of the effect of nonselective vasopressors in increasing splanchnic vasoconstriction. Against that is that the noradrenaline requirement in patient 4 was falling while the TD lymph iFABP level increased (Fig. 10B). Patient 3 had been weaned off noradrenaline after 36 hours. Another possible explanation for the observed results is that the lipid-rich feed acted as a confounder in the accurate measurement of the lipid-binding iFABP protein. 57
The anesthetic practice of running patients “dry” through long anesthetics to avoid fluid overload and attendant complications may conversely result in hypovolemia and persisting splanchnic vasoconstriction. There is some evidence that if enteral feeding is commenced too soon (i.e., before a patient is volume replete) that it might cause mucosal ischemia. For example, it has been observed in patients with acute pancreatitis that enteral feeding begun 24–48 hours after admission was more effective in reducing multiple organ failure and infective complications than enteral nutrition begun within 24 hours of admission.
59
It has been suggested that a patient should be fully resuscitated before commencing enteral nutrition
60
to avoid exacerbating mucosal ischemia, which may contribute to ileus and enteral feeding intolerance. This suggestion is supported by the changes in TD lymph composition with enteral feeding (i.e., increased concentration of iFABP,
There are significant limitations with this pilot study. The most important is the small sample size because of the study's early termination, preventing statistical analysis. Nonetheless, we think it is important to report our experience in this study. Detailed prospective studies of individual patients can still yield important observations 62 and generate hypotheses. The techniques used in this study are not applicable to nonthoracotomy patients and are therefore not generalizable to other patient settings. Major surgery and anesthesia as proinflammatory states are confounders, especially when assessing the impact of enteral feeding on the proinflammatory cytokines and markers of gut injury. There is also the concern that lipid-rich enteral feeds could influence the compositional assays in lymph. Despite these limitations and the early termination, the pilot study provided valuable experience, demonstrating the feasibility of this postoperative model for the study of composition and toxicity, confirming methods for lymph sampling, storage, and analysis, providing some validation for TD lymph composition findings in animal models, enabling optimization of a number of compositional analyses for human gut-lymph, and it has demonstrated some striking findings in relation to the effect of enteral nutrition and vasopressors on intestinal function, that warrant further investigation.
In conclusion, this pilot study demonstrated that the technique of intraoperative TD cannulation and longitudinal sampling of TD lymph is feasible. Our experience was that the risk of developing a chylothorax with inadequate or failed TD embolization was too high, and the study was appropriately terminated early. Nevertheless, the successful serial sampling of TD lymph and the analysis of compositional changes gave us a unique dataset and resulted in some key observations in human gut-lymph that warrant further investigation. The effect of enteral feeding on TD lymph composition, and in particular on the markers of intestinal ischemia and injury, suggest that intestinal injury occurs with enteral feeding in this context. Further research to optimize the timing, rate, and delivery of enteral feeding is required to ensure that the risk of intestinal ischemia is minimized, especially in patients who are already hypovolemic and on vasopressors.
Footnotes
Acknowledgments
The authors thank Grant Beban for his surgical expertise And Christine Keven for performing the biochemical and cytokine assays.
Authors' Contributions
A.B.J.E. conducted the clinical and laboratory studies, drafted the article and coordinated the revisions. J.H. conducted the laboratory studies and assisted in drafting the article. B.N.C. and A.H.H. oversaw and conducted the thoracic duct embolization procedures. K.L.P. was involved in the first clinical patient and seeking ethical approval for this study. A.R.J.P. oversaw the laboratory-based aspects of this study and edited the article. J.A.W. was the primary investigator supervising this project. He performed the intraoperative thoracic duct cannulations and edited the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The Health Research Council of New Zealand (Grant Number: 15/30) and the Maurice and Phyllis Paykel Trust (Grant Number: 3706308) funded this research.