
Abstract
Background:
Lymphedema results from inadequate lymphatic function causing swelling in subcutaneous tissues. Lymph is transported proximally through valved lymphatic channels and muscle contraction. The purpose of this study was to determine lymphatic function in nonambulatory patients with lower extremity neuromuscular disease.
Methods and Results:
Our Lymphedema Program database of 700 patients was reviewed for nonambulatory patients with lower extremity neuromuscular disease. Patient age, gender, disease, body mass index (BMI), and lymphoscintigram result were recorded. Eight patients were included in the study: myelomeningocele (n = 6), spinal muscle atrophy type 2 (n = 1), Charcot Marie Tooth (n = 1). Patient ages were between 15 and 36 years; five were female. BMI range for patients without swelling or a normal lymphoscintigram (n = 4) was 22–27. Four subjects with lymphatic dysfunction by lymphoscintigram all were obese (BMI 36–74; p = 0.03).
Conclusions:
Nonambulatory patients with lower extremity neuromuscular dysfunction and swelling can exhibit normal lymphatic function. Obesity is associated with abnormal lymphoscintigram result and lymphedema in this patient population. Individuals should be advised to maintain a normal BMI.
Introduction
Lower extremity lymphedema occurs when lymphatic load exceeds the ability of the lymphatic vasculature to transport lymph fluid proximally. Because muscle contraction stimulates lymphatic flow, individuals who are nonambulatory with lower extremity neuromuscular dysfunction may be at increased risk of developing bilateral lower extremity lymphedema.1–3 The purpose of this study was to evaluate lymphatic function in patients with lower extremity neuromuscular disease.
Materials and Methods
This study was approved by the Committee on Clinical Investigation at Boston Children's Hospital, and the procedures followed were in accordance with the ethical standards of the Helsinki Declaration of 1975, as revised in 2008. Our Lymphedema Program database was reviewed for nonambulatory patients with neuromuscular dysfunction. Patient age, gender, body mass index (BMI), and disease were recorded. The presence of swelling and lymphoscintigram result were recorded. Patients underwent lymphoscintigraphy to assess their lymphatic function; the test is 96% sensitive and 100% specific for lymphedema. 4 Lymphatic dysfunction on lymphoscintigram included delayed transit of radiolabeled colloid, dermal backflow, asymmetric tracer uptake into inguinal lymph nodes, or presence of popliteal nodes or collateral lymphatic channels. BMI between patients with normal and abnormal lymphatic function was compared using the Mann–Whitney U test. Statistical computation was performed with VassarStats. 5
Results
Eight of 700 patients (1%) in the database met inclusion criteria (Table 1). Patient age ranged from 15 to 36 years and three were male. Six patients had myelomeningocele, one individual had spinal muscle atrophy type 2, and one subject had Charcot Marie Tooth disease. BMI range of the four patients without swelling or a normal lymphoscintigram was 22–27. Four subjects with lymphatic dysfunction by lymphoscintigram all were obese (BMI 36–74; p = 0.03) (Fig. 1).
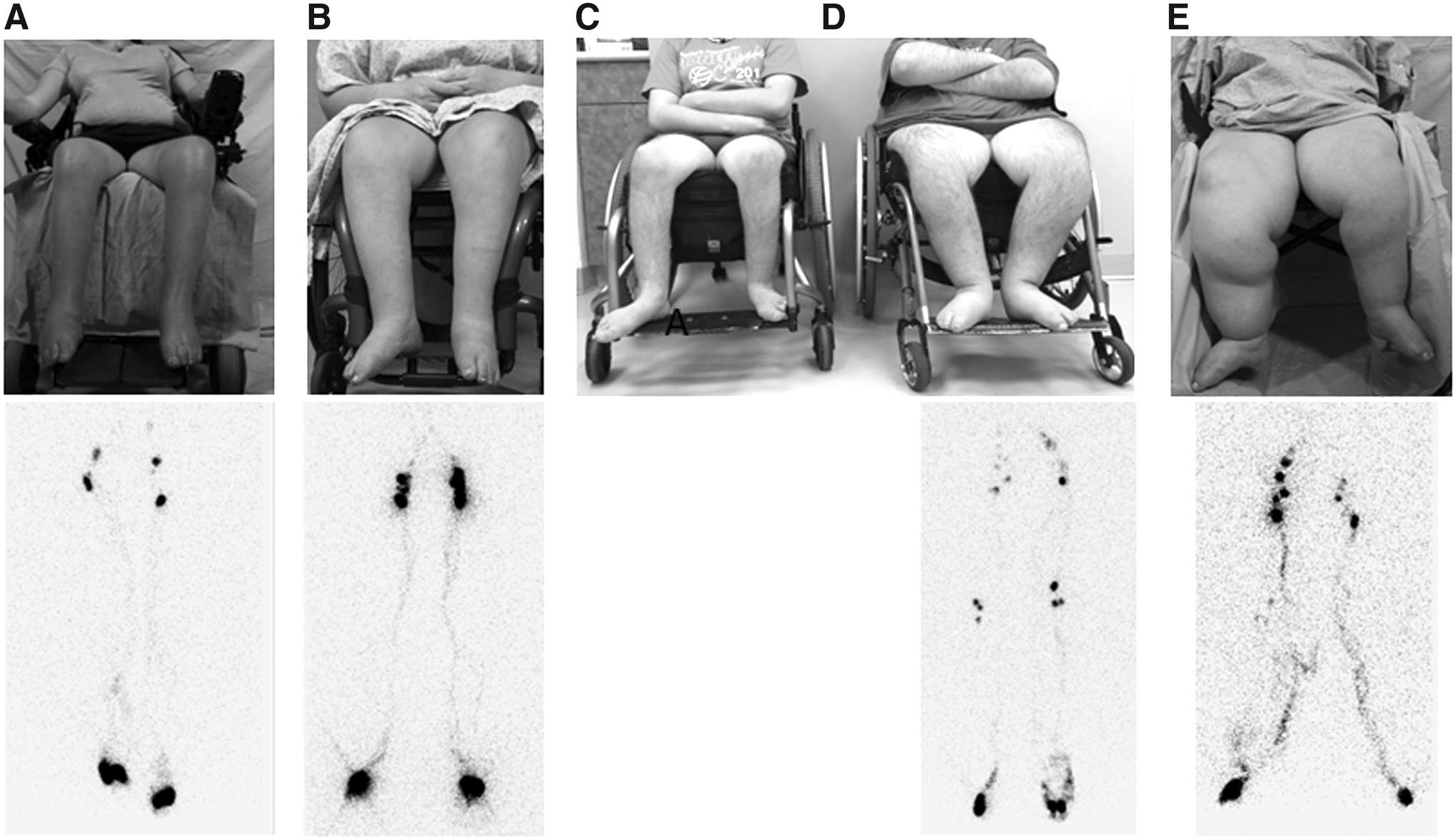
Obesity (BMI >30) is associated with lymphatic dysfunction in nonambulatory patients with lower extremity neuromuscular disease.
Nonambulatory Neuromuscular Disease Patient Cohort
(—) Lymphoscintigram not performed.
BMI, body mass index.
Conclusions
Proximal lymph flow is generated by the contraction of intrinsic smooth muscle as well as extrinsic skeletal muscles; valves prevent retrograde flow.2,3 Nonambulatory patients with lower extremity neuromuscular dysfunction theoretically should have a reduced ability to clear lymphatic fluid from the extremity and have an increased risk of lymphedema because of inhibited muscle contraction.1,6 However, paraplegia has not been associated with lymphedema, except for a possible increased risk with myelomeningocele.7–9
Our results suggest that BMI may be a critical determinant for the development of lymphedema in nonambulatory patients with paraplegia. All four subjects in our cohort with a BMI <30 had either no edema or intact lymphatic function by lymphoscintigraphy. In contrast, the four individuals with abnormal lymphatic function were obese (BMI >30). Obesity negatively affects the lymphatic system: (1) it is a major risk factor for the development of secondary arm lymphedema after breast cancer treatment,10–12 (2) it increases the morbidity of patients with established lymphedema, 13 and (3) extreme obesity (BMI >50) can independently cause lymphedema.14–16 Experimental data also support the clinical findings that obesity adversely affects lymphatic function.17–20 We hypothesize that obesity may be a “second hit” to the lymphatic system in patients who already have a reduced ability to transport lymph fluid because of neuromuscular compromise.
Individuals with myelomeningocele might have an increased risk of lymphedema not because of maldevelopment of the lymphatic system (i.e., primary lymphedema), but as a result of obesity. One study showed that patients with myelomeningocele and lymphedema were more likely to be obese (although lymphatic function was not evaluated by lymphoscintigraphy). 7 Adult patients with myelomeningocele also have an increased risk of obesity compared with the general population.7,21 A case series of three patients with myelomeningocele with lymphedema included one patient with lymphoscintigraphic evidence of lymphatic dysfunction, but BMI was not presented. 8
An advantage of this study is that 7/8 patients had their lymphatic function objectively documented with lymphoscintigraphy. Although lymphoscintigraphy is extremely sensitive for detecting lymphedema, the test has a 4% false-negative rate 4 and thus it is possible that a nonambulatory patient with a normal test could have undetected lymphatic dysfunction. Because of the overwhelming evidence that obesity negatively effects lymphatics, we believe that it is prudent to counsel nonambulatory patients with neuromuscular disease to maintain a BMI <30 to lower their potential risk of developing irreversible lymphedema. This is consistent with our current practice of advising all individuals with lymphedema, or those at risk for developing the disease, to maintain a normal body weight. Patients with lymphatic dysfunction have an increased risk of infection and subcutaneous fibroadipose deposition in their legs. 8 Further insight into the etiopathogenesis of lymphedema in nonambulatory patients with neuromuscular disease will be accomplished by studying additional patients.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this study.