
Abstract
Background:
Anecdotal evidence collected by a community organization suggested high prevalence of lymphatic filariasis (LF) in Sitapur district, Uttar Pradesh. Village volunteers subsequently conducted a line listing in 13 villages of Pisawan block and recorded 261 cases of known LF complications, namely hydrocele and lymphedema. This being far higher than official projections, a block-wide cluster survey was conducted to estimate the disease burden more accurately.
Methods:
Cluster sampling techniques were applied, and 41 clusters selected within Pisawan block. Survey teams comprising one woman and man interviewed member of all households in the cluster, recording details of individuals suffering from hydrocele or lymphedema within them. Age and gender were noted, as well as duration of symptoms and details of any treatment availed.
Results:
A total of 1851 patients (1256 males and 595 females) were reported to have lymphedema, hydrocele, or both in the 6931 households surveyed. This equates to a prevalence rate of 4.95% (with 9.75% margin of error) in Pisawan block. With these calculations, an estimated 11,049 + 1077 patients with LF complications in Pisawan block, Sitapur, UP in 2016.
Conclusions:
The high prevalence rate of LF complications in Pisawan block is disconcerting, especially considering India's commitment to eliminate LF by 2020. Compliance with Mass Drug Administration (MDA) must be improved. Furthermore, the Morbidity Management and Disability Prevention (MMDP) component of the National Programme for Elimination of Lymphatic Filariasis (PELF) must be strengthened so that such patients can lead a productive life.
Introduction
Lymphatic filariasis (LF) is a neglected tropical disease with 1.39 billion people estimated to be at risk globally. 1 Filaria, a tissue nematode, resides in human lymphatics and produces microfilaria that are found in the blood stream during late hours, and are spread by mosquito bites. About 120 million people are estimated to be infected. In endemic areas, children can be infected at an early age and begin to develop subclinical damage. Acute dermatolymphangioadenitis (ADLA) can occur due to secondary bacterial infections in the lymphatic system, 2 or as a direct affect by the filarial worms. Repeated infections result into long-term conditions such as lymphedema, hydrocele, elephantiasis, and chyluria—it is reported that there are 40 million such patients worldwide. Although LF is rarely fatal, lifelong ill health and disability impact quality of life as well as mental health.3,4
WHO established the Global Programme for Elimination of Lymphatic Filariasis (GPELF) in the year 2000. The programme has two main components—(1) Elimination of the Disease by Mass Drug Administration (MDA) of filaricidal drugs and (2) Morbidity Management and Disability Prevention (MMDP) through hydrocelectomy (for hydrocele) plus limb washing and self-care for lymphedema. This was subsequently incorporated in India's National Health Policy 2002 and the task of eliminating LF given to the National Vector Borne Disease Control Programme (NVBDCP), 5 which runs under the National Centre for Disease Control (NCDC).
MDA in India has resulted in a falling incidence of microfilaremia with 137 of the original 255 affected districts declared filaria free. 6 However, some of these districts subsequently failed to clear the Transmission Assessment Survey (TAS), which was required for official certification. It seems unlikely that India will meet its goal of eliminating LF by 2020. 7
LF continues to be endemic in many parts of Uttar Pradesh, including Sitapur district (see Map Fig. 1A, B). Volunteers associated with a community organization (Sangtin) had taken up this issue in 2015, focusing on Pisawan block, which is in the western part of the district. A line listing done by them recorded 261 cases—in 13 villages, which included 137 patients with hydrocele, 119 with lymphedema, and 5 with both. 8 A morbidity management camp was subsequently co-organized with a Delhi-based resource group (with expertise in treating LF) and the State Health Department. 8 A physical examination of 95 of the recorded cases by a surgeon confirmed that 90% were due to filariasis. The exceptions were hernia instead of hydrocele in three patients, and joint disease or heart/kidney disease instead of lymphedema in seven patients. 8

The mismatch between expected incidence based on the line listing implied 60,000 plus cases in Sitapur district. This varied greatly from the quoted government figure of 41179 and needed to be addressed. To get an accurate estimate of the disease burden in Pisawan block, a cluster survey was conducted in June 2016.
Methods
According to the 2011 census, there were 40,801 households in Pisawan block comprising 223,674 persons. 10 These were divided into 188 revenue villages, with a population range between 6 and 4124 in each. The current list of revenue villages was obtained from the Pisawan Block office and correlated with census data. This list was parsed to group together small villages within the same Panchayat and break up larger ones, with the help of local volunteers familiar with the region. The process resulted in Pisawan block being split into 183 clusters with a mean and median household size of 223.
A cluster sampling approach was used to calculate the number of households to be surveyed 9 —in this approach the number of households (nh) to be surveyed is estimated as

where
z is the level of confidence desired = 95% confidence interval = 1.96
r is the expected prevalence, estimated at 2% = 0.02
f is the sample design or clustering effect deff, which is further estimated as
deff = 1 + roh (b − 1)
where roh is the cluster homogeneity, estimated at 0.0210
b is the cluster size = 223
Thus f = deff = 5.44
k is a multiplier to account for nonresponse, estimated here as 1.1
p is the proportion of target population to total population = 1
ň is the average household size = 5.4 for Pisawan block
e is the margin of error, taken here to be 15% of r = 0.15r
Using these values, the number of households to be surveyed was calculated to be 9271 households or 41.57 clusters. Using a random number generator, 42 clusters were identified from the list of 183 with a plan to survey all households within the cluster.
The survey tool was adapted from the NVBDCP “Patient Card” used for disease burden estimation. Training on this tool, the disease and patient identification were provided using the NVBDCP guidelines 11 for six teams, each comprising one woman and one man. Strategies on obtaining information from reticent families were also developed. The survey was then conducted in June 2016. All households in each cluster were approached and male as well as female members independently asked if anyone in their family suffered from lymphedema or hydrocele. If the answer was yes, further details of the patient(s) were noted in the form of age, gender, problem, duration of symptoms, and what treatment had been undertaken, if any.
Some scheduling problems were encountered. The team had to complete the survey in 10 days. Furthermore, some villages had fewer households than listed in the 2011 Census. Also, some variance in the physical location of the hamlets significantly added to travel time. Therefore, finally only 41 clusters having a total of 6931 households and a population of roughly 37,427 could be surveyed. The data from the survey tool was entered and analyzed in an open-source processing software tool (LibreOffice Calc).
Results
In the 6931 households surveyed, LF affected patients were identified in 1696 households with a total of 1848 patients. This consisted of 594 women and 300 men suffering from lymphedema, 905 men suffering from hydrocele, and 47 men with both conditions. For two males no details were recorded. Three infants below the age of two were recorded but were removed from the percentage calculation, with the assumption that their conditions were congenital and could not be because of LF.
Based on these numbers, the prevalence rate of LF complications in Pisawan block was calculated as 4.94%. Using this number and the reduced cluster size, the margin of error was recalculated to be 9.75%. Thus, with 2011 census numbers, the case load in Pisawan block was calculated to be 11,049 ± 1077 cases. Assuming a similar prevalence rate for Sitapur district (population 4,483,992) would result in 221,509 ± 21,597 cases.
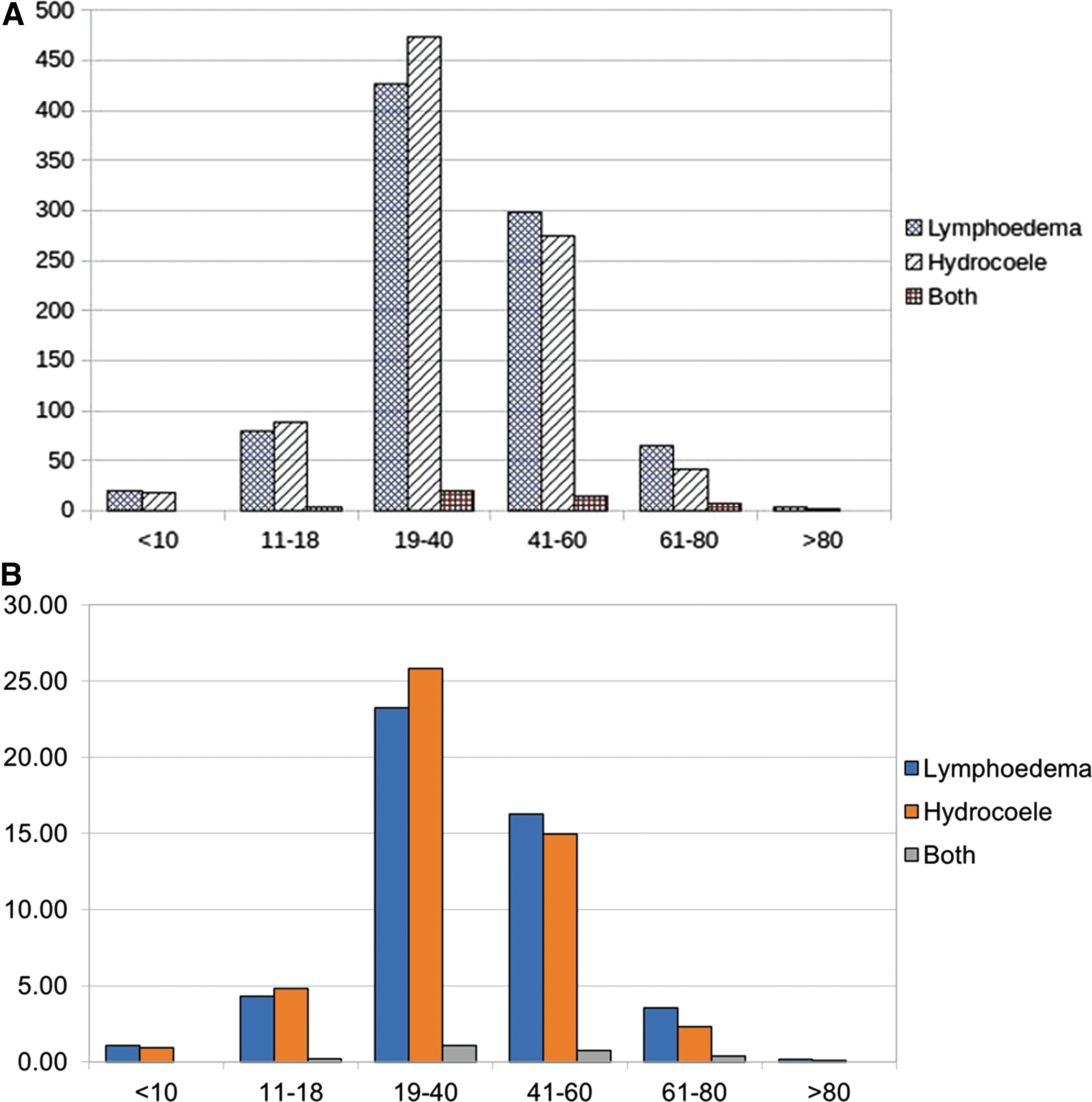
The patient's ages were recorded in 1832 cases and are depicted in Figure 2. 50.2% (n = 919) of the patients are aged 19–40 years, showing that a significant percentage of patients are affected during their most productive years. The duration of illness was recorded in 1805 cases and is shown in Table 1. It ranged from 1 month to 50 years, with a median duration of 48 months. Patients suffering from hydrocele (median duration = 48 months) or both conditions (60 months) tended to report a longer duration of illness than lymphedema patients (36 months).
Reported Duration of Illness
Patients and their families were asked what treatment, if any, had they availed and responses from 1818 patients were recorded. These are shown in Table 2. It is notable that 57.3% (n = 508) of hydrocele patients had not availed of any treatment. Only 5.7% (n = 103) of all patients availed of treatment in a government health facility and an additional 1.6% (n = 30) went to both government and private health facilities. The rest either did not avail of any treatment, went to informal practitioners or to the private health sector.
Type of Treatment Undertaken in the Past by Those Who Had Suspected Hydrocele or Lymphedema
Discussion
Lymphedema in early cases is reversible with the combination of diethylcarbamazine and albendazole (distributed in the MDA programme), but in later stages elimination of the worm does not decrease the progression to long term ill effects. 12 Lymphedema, or what is called elephantiasis, becomes persistent after repeated acute attacks (ADLA) that result in damage to the lymphatic system. Thus, reduced incidence of microfilaremia will not immediately result in reduction of long-term problems such as hydrocele and lymphedema. Most cases develop clinical effects from infestation that occurred in childhood! 12 Thus, even if MDA is successful and LF is eradicated, morbidity management is required for years afterward.
Furthermore, informal interviews within the affected households as well as with health staff and ASHAs in Pisawan block raise questions about the effectiveness of the MDA programme itself. Discussions revealed an extremely low awareness about MDA—most said that they had not received the medicines. The common belief was that only those who were suffering from symptoms needed to take the medication. The survey team itself had been unaware that hydrocele was a manifestation of LF before their orientation. Other studies have shown similar problems in awareness about LF, coverage of MDA, and compliance thereafter.13,14
Although the morbidity management programme is operational in many parts of the country, its utilization is perceived to be low due to lack of awareness, low knowledge of clinical staff, restricted mobility of patients, and so on. 15 Within this study, most patients had not availed of the government programme, instead visiting private practitioners or traditional healers. Some patients told the surveyors that they had visited multiple doctors and healers, and were desperate for an effective treatment. Complications after hydrocelectomies performed by less trained and sometimes unqualified practitioners were also reported. Anecdotal tales of expenditure incurred ranged up to about Rs 1.5 lakh ( = 2300 USD) in one instance for lymphedema and about 0.5 lakh ( = 700 USD) for a complicated surgery for hydrocele.
A limitation of this study is that it depends on self-reporting, which could be erroneous. The use of mixed-gender teams and specific training on NVBDCP were attempts to overcome this. However, conditions such as hernia can mimic hydrocele, whereas joint disease or limb swelling due to other conditions can mimic lymphedema. These can be a reason for inflation of incidence. In the earlier line listing, 8 about 10% of those cases were subsequently diagnosed as resulting from nonfilarial problems. Assuming a similar situation, these data result in a lower figure of 9944 ± 970 patients in Pisawan block. With continuing population growth, which was 23.9% from 2001 to 2011 in Sitapur district, one can expect a higher case load.
NVBDCP figures state that India has a total of 0.8 million long-term sufferers of LF. However, this is at variance with WHO figures that state that India has 40% of the global load, that is, 16 million. This survey suggests a total closer or even higher than WHO estimates. According to NVBDCP, hydrocele is less common than lymphedema, but the comparative figures from this study show a relative incidence matching that of WHO, which is around 52% for hydrocele. This could be due to (1) low awareness of the links between LF and hydrocele and (2) a reluctance by hydrocele patients to report their disease, which, however, the current survey addressed by constituting teams of men as well as women.
In conclusion, LF and its complications are a significant problem in Pisawan block and indicate a larger population at risk. Both the MDA and morbidity management components of the National Programme to Eliminate LF must be strengthened to halt the spread of the disease and provide much-needed care for patients.
Statement Regarding Experiments on Human Subjects Helsinki Declaration
This was a house-to-house survey done after full explanation and consent thereof of the subjects participating in the survey.
Footnotes
Acknowledgments
The authors acknowledge the contributions of the survey team consisting of Jagannath, Bitoli, Maya, Ramasre, Manohar, Sunita, Rajrani, Surender, Kishori, Anita, Srikishan, and Anuradha, who tirelessly collected data from households in the scorching June heat, and the important role of the Sangtin admin team in data entry.
Authors' Contributions
Team SANGTIN (all three): Planning and execution of survey. S.B.G. (SATHI): Emphasizing the need and document writing.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding obtained from external sources.