
Abstract
Bioelectrical impedance spectroscopy (BIS) is a technology that is widely used for the assessment of body composition. The method is based on the measurement of the electrical resistance of the body or a body region that can be quantitatively related to the amount of water in the tissues. Lymphedema is characterized, at least in its early stages, as an accumulation of lymph, an extracellular fluid. In the late 1980s, it was recognized that it might be possible to adapt BIS protocols to measure this increase in lymph volume. Subsequently, the use of BIS for the early detection of breast cancer-related lymphedema was demonstrated in the early 1990s, with BIS reference values indicative of lymphedema published in 2001. The subsequent two decades have seen BIS become a widely accepted method for lymphedema assessment. This review traces the evolution of the BIS technique since its inception and presents the current state of the art, with particular emphasis on utility in clinical practice.
Introduction
Lymphedema is a chronic condition resulting from dysfunction of the lymphatic system characterized by accumulation of lymph in the interstitial spaces, leading to swelling of the affected body region. 1 Most commonly, a limb is affected, although lymphedema may also affect elsewhere, including the head, neck, breast, or genitals. 2 Lymphedema may be of genetic origin, primary lymphedema, or occur secondary to damage to the lymphatic system. In tropical regions, secondary lymphedema can result from lymphatic obstruction due to parasitic infection by, for example, Wuchereria bancrofti, whereas elsewhere it is primarily a result of lymphatic damage that results from treatment (surgical or radiation) for cancer. 2
Definitive diagnosis of lymphedema may be accomplished through imaging of impaired lymph flow, using techniques such as lymphoscintigraphy or indocyanine green fluoroscopy. 3 However, most patients are currently diagnosed through clinical assessment only. This is primarily completed through measurement of symptomatic swelling.4,5 Historically, swelling has been assessed by volumetric techniques, such as water displacement or geometric calculation from circumferential measurements of the affected limb. 4 Opto-electronic measurements of volume have also been developed. 6 Though easy to use, and inexpensive in the case of water displacement and geometric techniques, these methods suffer from the potential disadvantages of lacking specificity and sensitivity for lymphedema.
Change in limb volume and size may occur for multiple reasons other than accumulation of lymph. Although in postcancer-treatment patients, an increase in limb volume is a likely indication of lymphedema, swelling from other causes such as therapeutic use of taxane-based chemotherapies or simple weight gain is not precluded. 7 Further, perceptible swelling is a relatively late event in the development or progression of lymphedema. For example, in breast cancer-related lymphedema (BCRL), a whole inter-limb volume difference of 200 mL between an at-risk arm and the contralateral unaffected limb is considered indicative of lymphedema. 8 However, diagnosis at this threshold precludes the early detection of subclinical lymphedema. Ideally, an assessment technique that measures specifically lymph accumulation with high sensitivity, that is, the smallest significant volume change, is required.
Bioelectrical impedance analysis is a technique in which the opposition to the flow of an electric current through the body, or a region thereof, is measured. The measured impedance is quantitatively related to the volume of water in the body or region. 9 The technique has been widely adopted to measure body composition, as body water can be related directly to the fat-free mass of the body. 10 A derivative of bioelectrical impedance analysis, bioelectrical impedance spectroscopy (BIS), has the ability to assess not only total body water but also its constituent compartments, intra- and extracellular water. 11 Three decades ago, it was recognized that BIS might provide a method for the assessment of lymphedema since accumulation of lymph represents an increase in extracellular water. 12 Since this original observation, much research has been undertaken to develop BIS as a robust method for early detection and monitoring of lymphedema (Fig. 1).
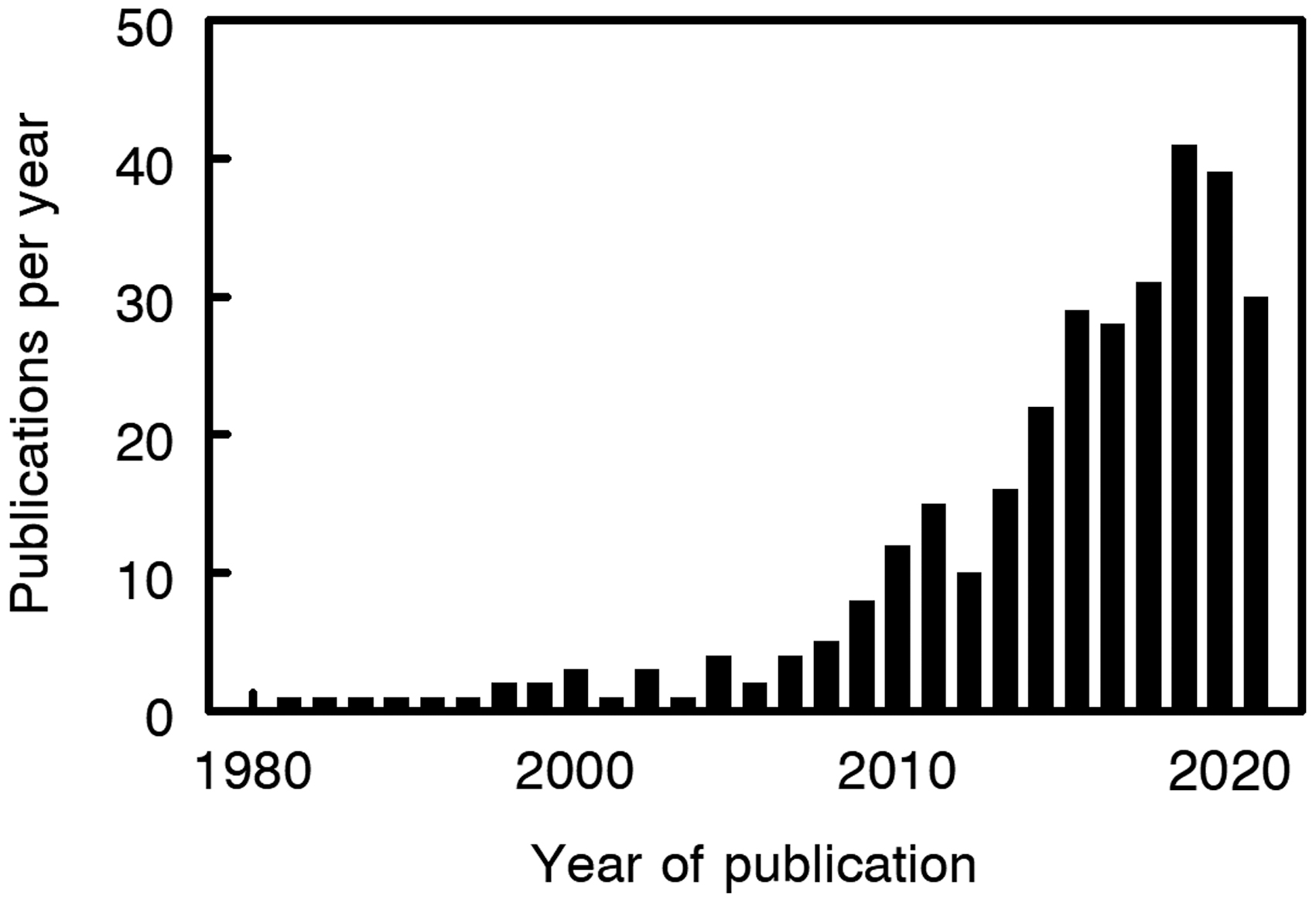
Publications per year listed on PubMed by using search terms. “Lymphedema AND (Bioimpedance spectroscopy OR Bioelectrical impedance OR Multifrequency bioelectrical impedance OR Bioimpedance)”.
Historical Perspective
Impedance technology was first used to measure total body water in the early 1960s, but the method languished for 25 years until a commercial impedance analyzer became available in the mid-1980s. During these intervening years, a small number of researchers continued to investigate impedance technology, including the development of the spectroscopic (BIS) technique, then called multi-frequency or swept frequency impedance analysis, in the 1970s. The first researchers to exploit this technique to specifically assess lymphedema were Watanabe et al. in Japan in 1989, 12 although in the previous year another group in Japan had reported 10 years' experience using “impedance plethysmography” to measure change in peripheral volume of edematous limbs treated with pneumatic massage therapy. 13 In both cases, few details of the impedance devices are provided but are likely to have been manufactured “in-house” by the researchers.
Despite these pioneering studies, neither group seems to have continued to research the application of impedance technology to lymphedema assessment. It was not until 3 years later, in 1992, that the now familiar BIS technique was specifically recommended for the early detection and management of lymphedema. 14 This publication precipitated an upsurge in research into the validity and usefulness of BIS for lymphedema assessment (Fig. 1). It stimulated the development of commercially available impedance devices specifically designed for this purpose. In addition, coincident with technological developments, increasing adoption of the technology in routine clinical practice and growing acceptance of the technique as a reference method emerged.
Bioelectrical Impedance Technology and Its Application in Lymphedema—Theoretical Basis
When an electric current is applied to the human body or part, current flows through the electrically conductive tissues and organs (see Refs.9,11,15 for details). Conduction is through the water compartment of these tissues. However, body fluids are not perfect conductors and the flow of the current is opposed by resistances inherent in the composition of the fluids and the capacitive nature of cell membranes, which is known as reactance (Xc). This opposition to current flow is referred to as either impedance, conventionally denoted by Z, or resistance, denoted by R; both are measured in ohm. The distinction between impedance and resistance is important. Resistance is the opposition to current flow due to the inherent resistivity of tissue fluids. Impedance is the total opposition to current flow, that is, due to both fluid resistivity and cell membrane capacitance. Impedance and resistance are directly related to the conductive volume. If we consider a simple cylinder, the impedance along the length of the cylinder to an applied electric current is inversely proportional to its cross-sectional area (Fig. 2) and is described by
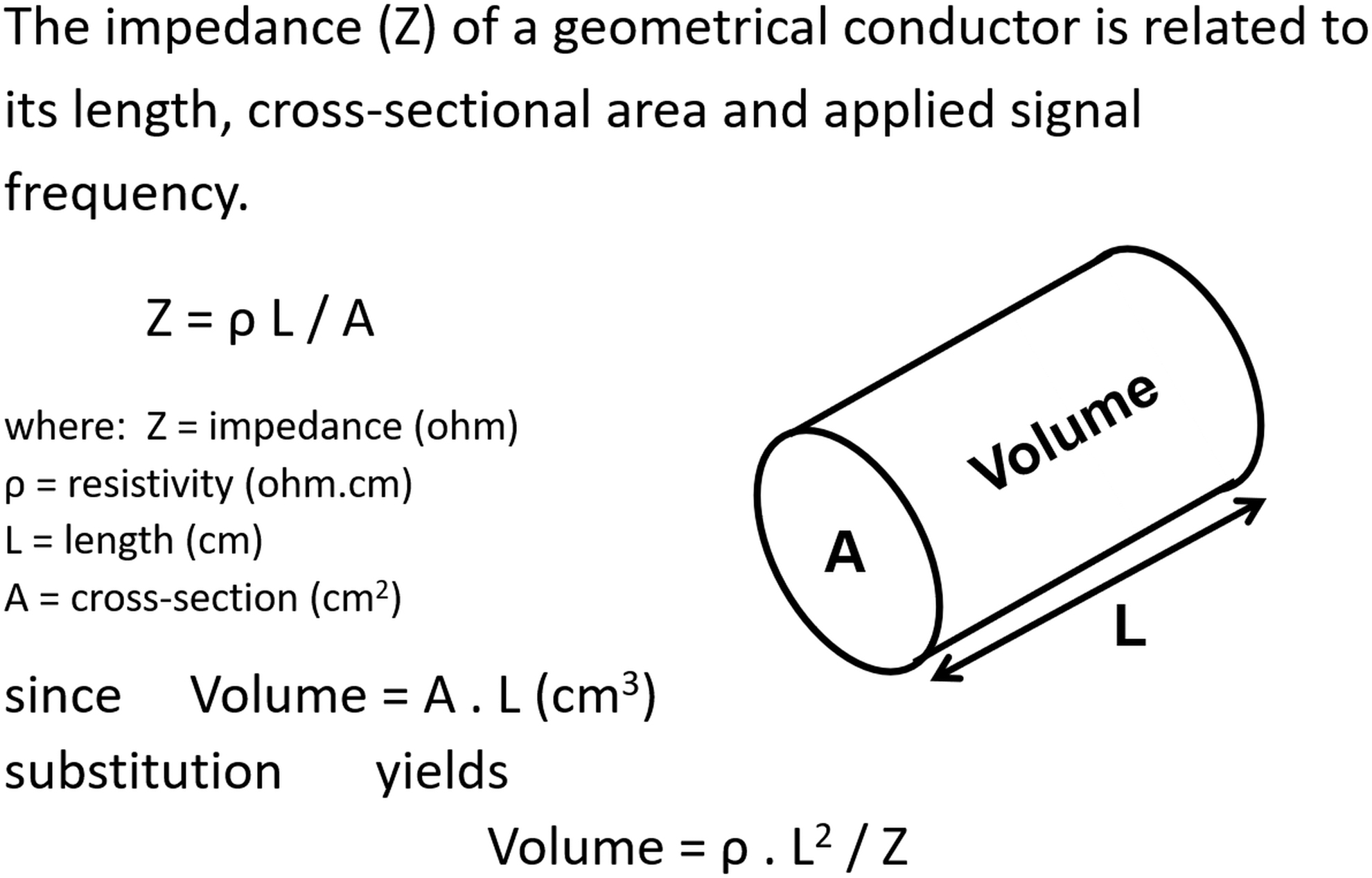
Theoretical basis of bioelectrical impedance relating measured impedance to conductor volume.
This may be rewritten as
where ρ is the resistivity. Impedance is also proportional to the length (l) of the cylinder
or
Combining Equations (2) and (4) yields
The volume of the cylinder is provided by simple geometry as
Combining and rearranging Equations (5) and (6) provides
Equation (7) demonstrates the relationship between impedance to volume and length. It is this relationship that is exploited in the assessment of lymphedema. In clinical practice, Equation (7) is extended to apply to the body region at-risk of or affected by lymphedema, such as an arm after treatment for breast cancer. For these purposes, it would be desirable to measure solely the impedance of the lymph compartment of a limb. Although this is not directly possible, BIS provides a surrogate measure.
When using BIS, the applied electric current is a harmless alternating current. A characteristic of biological tissues that comprise both conductive fluids and capacitive membranes is that current flow is frequency dependent (Fig. 3). At a low frequency, therefore, current will flow exclusively through the extracellular water compartment; in contrast, at high frequencies, current can cross cell membranes and it flows through total body water. Although to predict optimally the volume of the extracellular water compartment, which includes lymph, impedance measurements would occur at very low, ideally zero, frequency, this is not possible, for both technical and safety reasons. 16 The BIS devices, therefore, make measurements of resistance and reactance over a practicable range of frequencies and extrapolate these data to zero frequency by using an approach known as Cole modeling (Fig. 3). The resistance to current flow measured at zero frequency (R0) is the measure of extracellular water volume. With this consideration, Equation (7), therefore, becomes
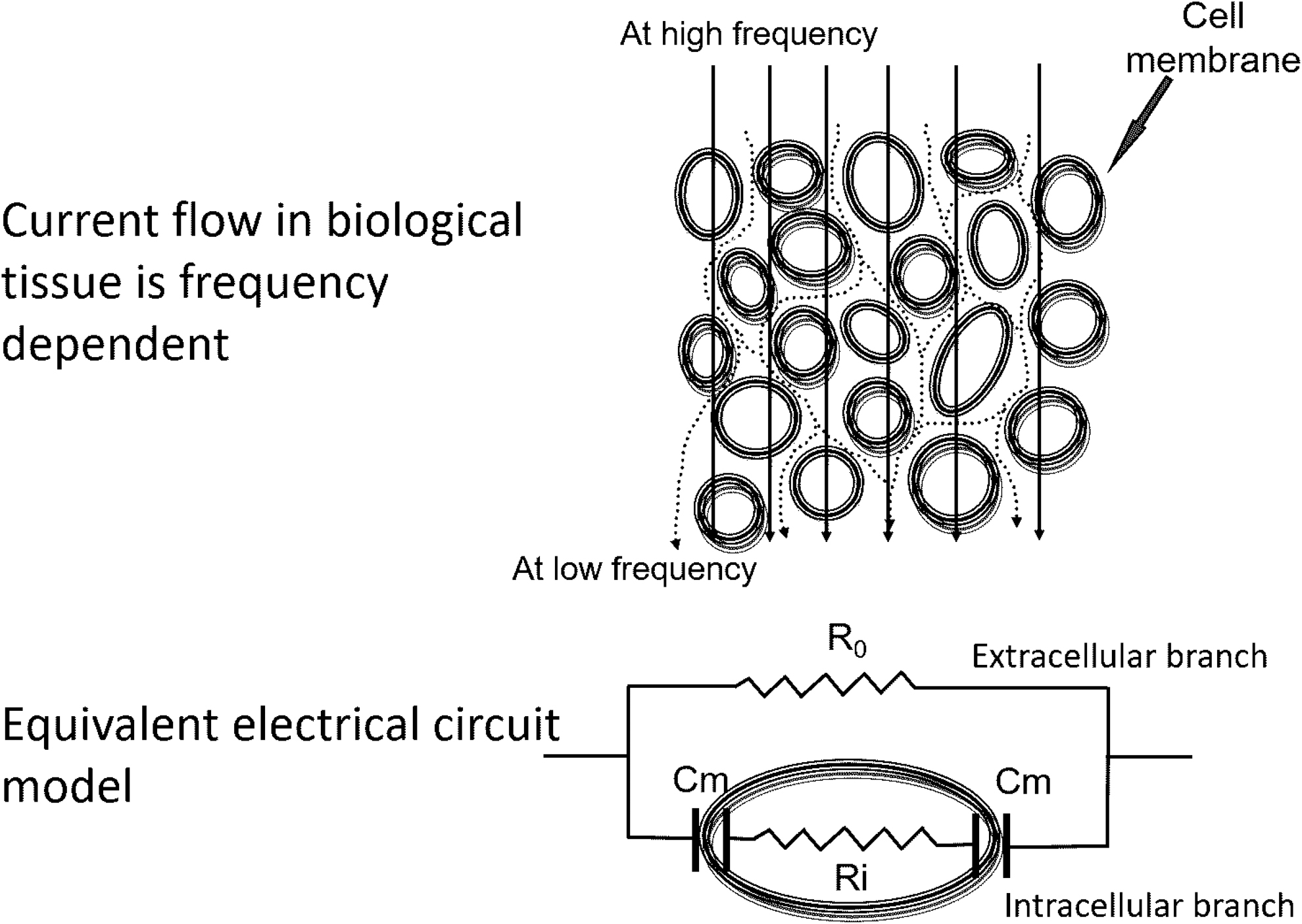
Model of current flow through biological tissue. Current flow is frequency dependent. At low frequency, current flows preferentially through extracellular water; at high frequency, current can penetrate the cell membrane and flow through both intra- (ICW) and extracellular water (ICW) and may be modeled as an electrical circuit consisting of a resistor (R0) representing ECW resistance in parallel with a capacitor (Cm) representing the cell membrane and a resistor (Ri) representing the ICW resistance. Key: (——) Current flow at low frequency; (—) Current flow at high frequency.
If length and resistivity are constant, then increases in ECW volume due to lymph accumulation are reflected by a decrease in R0. If length and ρ are known, Equation (8) can be solved to provide a volumetric measure directly (in mL). However, in reality, ρ is not known with certainty. Further, length may also be indeterminate since it is the conductive length, which is unknown and a surrogate measurement such as limb length may not be available. The volume of lymph in mL, is therefore, rarely reported or used in any practical sense.
Practical Aspects of Measurement
Impedance is measured by the impedance measurement device between electrodes placed on the skin surface. Current practice uses a tetrapolar electrode arrangement to direct and measure this impedance. The tetrapolar arrangement places a pair of impedance sense electrodes spanning the body region of interest as well as a second pair of drive electrodes located distally to the sense electrodes that injected the current into the body. Separating the current drive electrode circuit from the impedance sense electrode circuitry mitigates measurements being confounded by the large skin surface-electrode resistance. 17 A combination of tetrapolar and bipolar, where the. current drive and sense electrodes combined, has been explored as a means for measuring epidermal thickness in lymphedema.17,18 In the original protocols, electrodes were located as spanning the region of interest, for example a limb, by locating one sense electrode at the wrist and the second a set distance, typically 40 cm, proximal on the arm.14,19 The current drive electrodes were placed distally at the base of the fingers and at the acromion.
Research showed that greater precision of measurement could be obtained by adopting the principle of equipotentials, with the second sense electrode being placed on the contralateral limb, in line with the ulnar styloid for the upper limb and between the malleoli for the lower limbs. 20 This provides a “virtual” electrode location on the ipsilateral limb along the line of equipotential. Although the actual anatomical position of this virtual electrode is not known, it is consistent from person to person and application to application, reducing variability in measurement. Electrodes are electrocardiogram-style gel electrodes and may be either dual or single tab and are available from a variety of manufacturers.21,22 Attachment sites are cleaned with alcohol before electrode attachment. Measurement is time is quick, less than 1 minutes, and performed with the subject supine. A recent innovation has seen a move away from gel electrodes to the subject standing on electrode plates while placing their hands on electrode plates.23,24
Toward Clinical Utility
In the early studies of Yamazaki et al., the increase in resistance was used as an index of amelioration of swelling after pneumatic massage therapy in repeat measurements in patients with pre-existing lymphedema pre- and post-treatment. 13 There was no attempt to use impedance measurements for detection of lymphedema. Watanabe et al. compared R0 and the ratio of extracellular resistance with intracellular resistance (R0:Ri) in a small group of control (no edema) patients with the equivalent indices in a group of patients with lower limb lymphedema and suggested that these indices could be sensitive indicators of local edema. 12 In a study of women with unilateral BCRL, Ward et al. used the difference in R0 values between the affected and unaffected limbs to discriminate those with lymphedema from a comparable group of women without lymphedema. 14 This approach was used to effectively monitor response to treatment in women with BCRL and has been shown to be significantly more sensitive than circumferential measurement both in the early diagnosis of lymphedema and in monitoring change. 25
The measurement protocol was refined to adopt the equipotential measurement approach, with the impedance outcomes expressed as inter-limb ratios rather than inter-limb differences. The adoption of ratios helped minimize inter-patient variability due to the wide range of absolute R0 values seen between individual patients. 14 In 2000 and 2001, Cornish et al. successfully applied the R0 ratio method for the early detection of lymphedema.19,26 They established ratio thresholds to identify those with unilateral arm lymphedema. 26 Unlike the approach used to date for circumferential or water displacement volume methods where an arbitrary difference in circumference or volume was used as a cut-off, these authors used a statistically-based approach in which the detection threshold was set at three standard deviations (SD) above the mean ratio found in a healthy control population (Fig. 4). Thresholds were established to account for differences in R0 due to limb dominance and whether the at-risk or affected limb was dominant or non-dominant. This subsequently became the standard for early detection of lymphedema that is now in widespread use, although recent research has suggested that 3 SD may be too conservative and that 2 SD provides better sensitivity (Ref. 27 and see later).
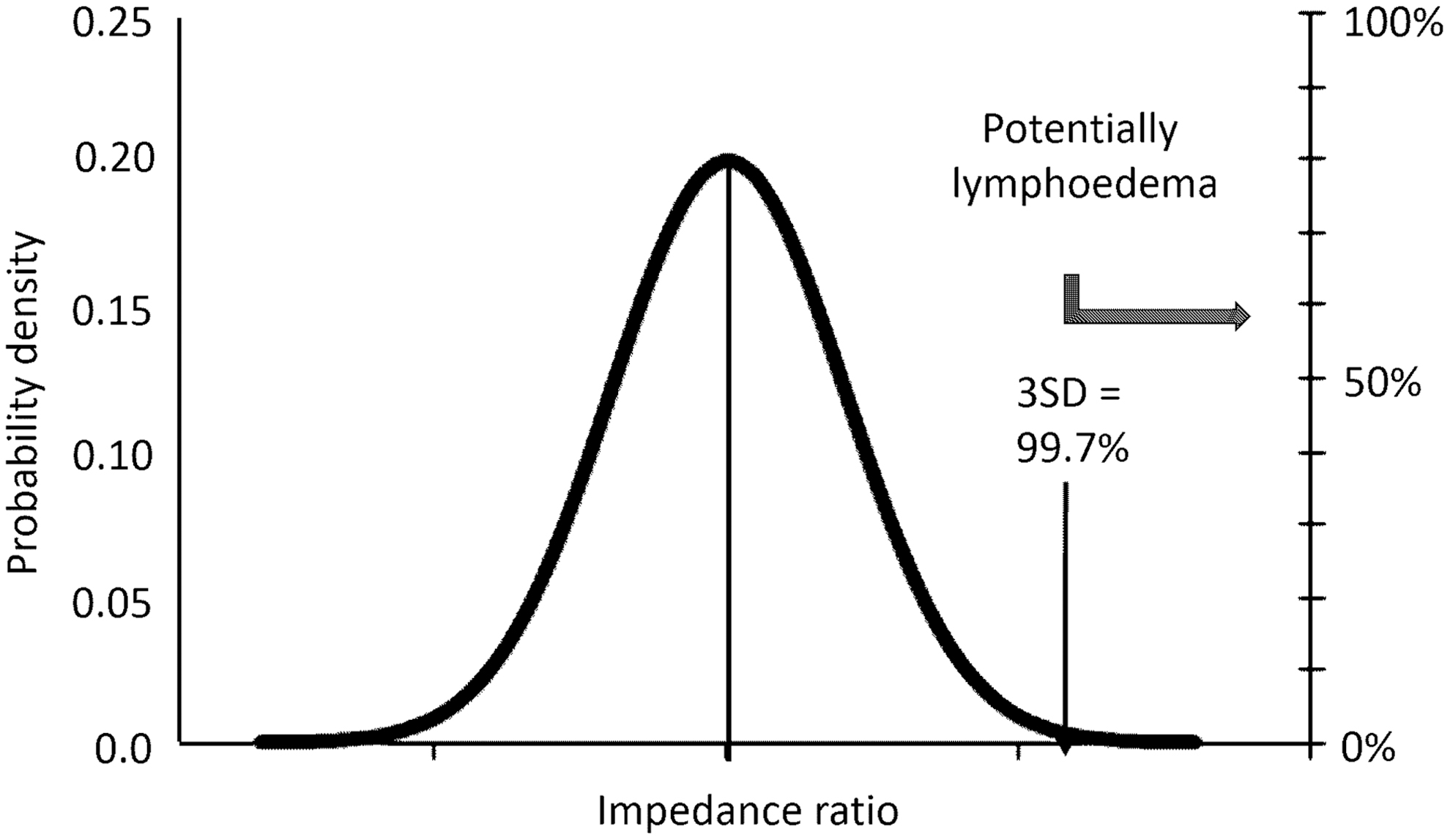
Normal distribution of inter-arm resistance ratios (R0 non-dominant: R0 dominant) observed in in a healthy control population. The presumptive presence of lymphedema is indicated by a ratio greater than a specified threshold, for example, 3 SD above the mean. SD, standard deviation.
Although the ratio of R0 values between unaffected and affected or at-risk limbs was suitable for use in cases of unilateral lymphedema, it was clearly not applicable to bilateral cases in which swelling and a change in R0 occurs in both limbs. Shortly thereafter in 2002, this same group of researchers revisited the original approach of Watanabe, using R0:Ri ratios. They were able to demonstrate that comparison of the R0:Ri ratio between an affected limb and unaffected limb but not necessarily the same limbs, for example, an affected leg with an unaffected arm, could be used to detect lymphedema in bilateral cases, for example, where both legs are affected. 28
The next major advance came in the introduction of the Lymphedema index or L-Dex score. 29 This came from commercial research and development, rather than academic research, by a leading manufacturer of BIS devices. 30 It had been recognized that the interpretation of changes in R0 ratios was not always intuitively obvious. This arises primarily due to the inverse relationship between impedance and volume, such that swelling is linked to an increase in volume but a decrease in impedance. To provide a sense of “increase” in cases of lymphedema, the R0 ratio is calculated as R0 unaffected to R0 affected. A ratio greater than 1 is produced and the ratio increases with greater limb swelling. In addition, although comparison of an individual patient's ratio to the calculated mean + 3SD threshold allows classification of lymphedema in cross-sectional studies, it does not facilitate easy monitoring of change in longitudinal studies in the same individual. Consequently, the L-Dex score was introduced. An L-Dex score is a patient's R0 ratio that has been scaled and linearized to the mean + 3SD threshold. An L-Dex score of 10 units corresponds to the ratio of the mean + 3SD threshold, indicative of the presence of lymphedema (Fig. 5). The commercial availability of BIS devices specifically for lymphedema assessment that provide simple and easily interpretable results as graphical displays of L-Dex scores has converted BIS technology from a research tool to a routine clinical assessment.
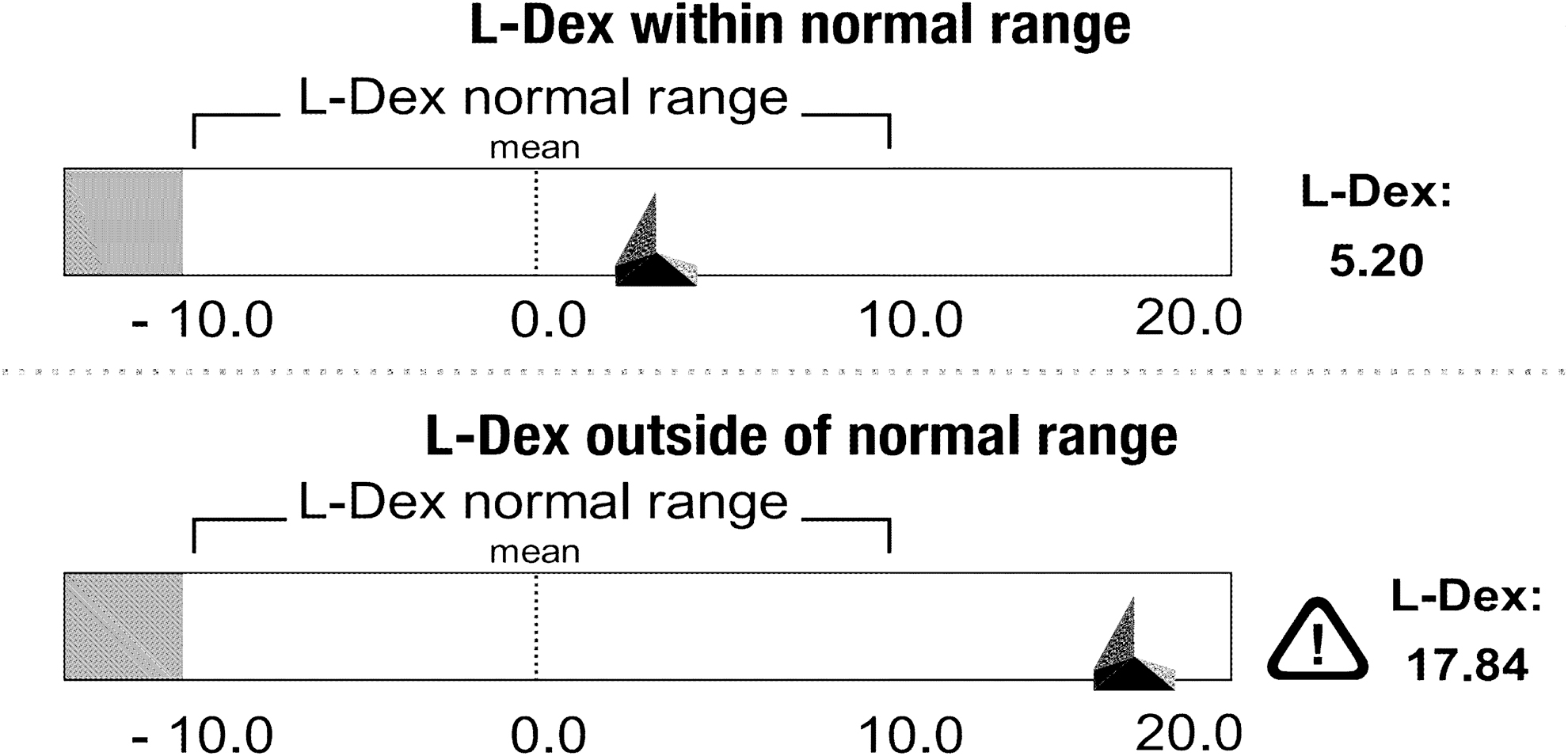
Interpretation of L-Dex scores. An L-Dex is a patient's inter-arm R0 ratio (unaffected: affected) linearized against the normal distribution of ratios observed in a healthy population. A score greater than 10 (or a change in score greater than 10) is equivalent to exceeding the 3 SD ratio threshold indicative of the presence of potential lymphedema and is used to trigger further investigation (Figure copyright Impedimed Ltd. adapted and used with permission.)
Clinical Utility of BIS Assessment
Numerous studies on the agreement between populations and reliability of assessment of the upper limb using BIS have been undertaken. Strong agreement for the normative inter-limb mean and SD between differing healthy populations, particularly for the dominant limb, have been shown, including those in Australia, 31 the United States,32,33 and China, 34 suggesting their universal utility. Further, for the upper limb, both inter-and intra-rater reliability has been found to be excellent.27,35,36 Similarly, high reliability was found when BIS was used to assess the hand [ICC (2,1) = 0.842, 95% confidence interval; CI 0.900–0.967] 37 and the lower limb (concordance correlation coefficient = 0.88, 95% CI 0.82–0.92). 38
Assessment of the validity, sensitivity, specificity, and predictive performance of BIS is more complicated than assessment of reliability due to a lack of consensus on a gold standard for the diagnosis and assessment of lymphedema for comparison. Suggested gold standard reference assessments include: previous diagnosis of lymphedema, 39 lymphoscintigraphy,40,41 and opto-electronic volumetry (perometery).42,43 To perform a true validity, sensitivity, or specificity analysis, the test method needs to be compared with a definitive reference method.44,45 Unfortunately, there is no consensus as to what constitutes the “gold standard” for lymphedema detection or diagnosis. The performance of BIS, therefore, has been compared against numerous reference standards, including functional measures, such as imaging,40,41,46 measures of swelling, for example, volume increase assessed by perometry29,43 or water displacement 47 or changes in limb circumferences,48–50 subjective assessment of symptoms, 51 and clinical diagnosis. 39 For many of these assessment tools, definitive criteria for the presence or absence of lymphedema are not available or agreed on. This has led to a variety of sensitivity and specificity findings for BIS.
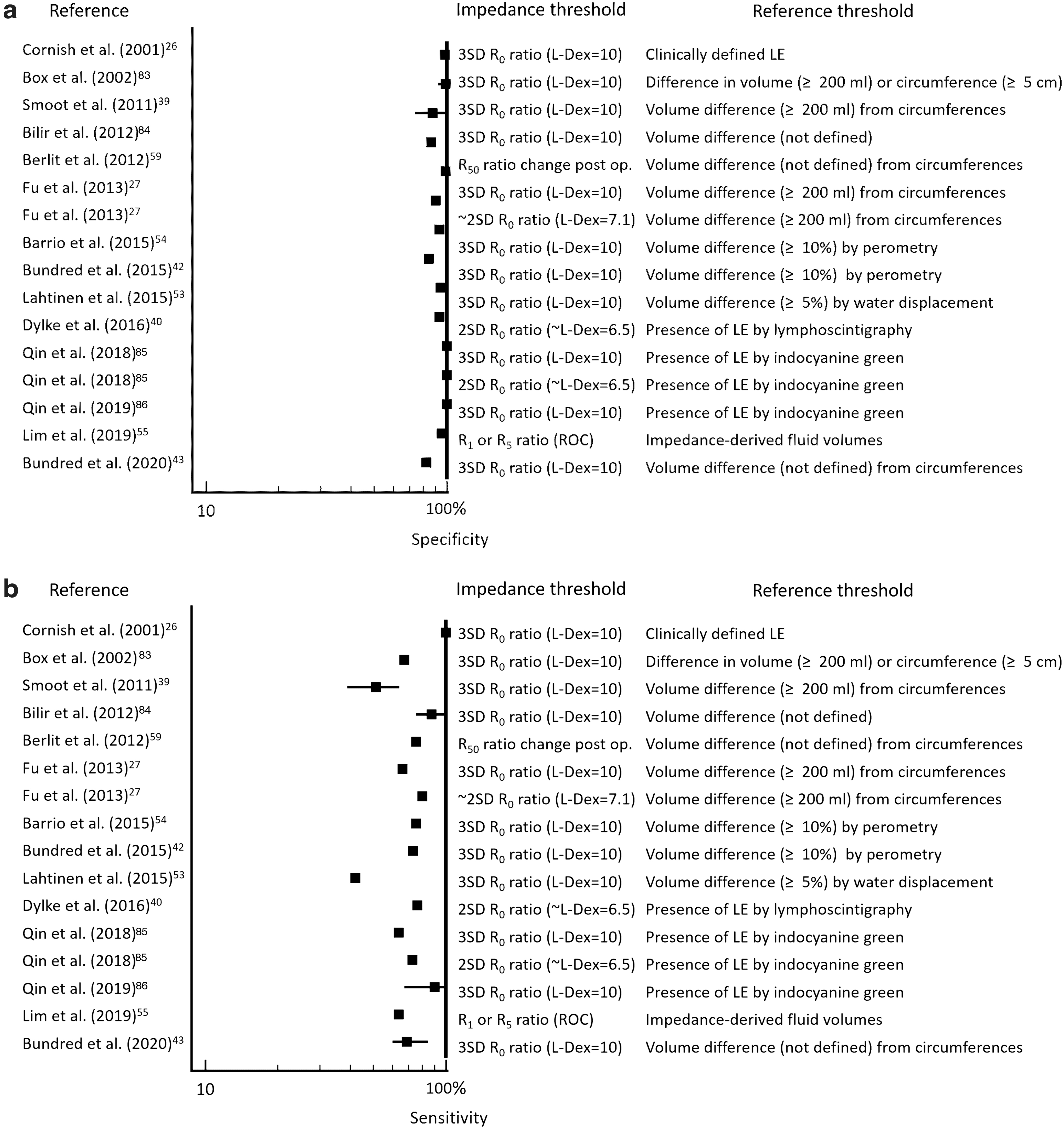
Statistical sensitivity and specificity for the assessment of upper limb lymphedema by BIS were first determined by Cornish et al., 26 who found 100% sensitivity with 98% specificity by using a normative mean + 3 SD threshold when compared with sequential circumference measurements. Since then, further studies have found generally high specificity, ranging from 64% to 100%, with somewhat lower sensitivity lower, ranging from 42% to 100% (Fig. 6). Notably, no recent analysis has achieved 100% sensitivity, as found by Cornish et al. 26 This may relate to differences in measurement protocol. Cornish et al. determined that lymphedema was present only after two consecutive 1-week apart positive BIS measurements, whereas more recent studies have relied on a single measurement, despite it being recognized that lymphedema may wax and wane. 52
Sensitivity
The wide range of sensitivity and specificity findings are also likely due to different thresholds for both BIS and the comparison measurements being chosen across the literature. For example, a volume difference between arms of 5% 53 has been adopted by some, whereas others adopt a relative inter-limb volume change cut-off of 10%42,54; however, Lim et al. adopted a reference standard of circumferences taken above and below the elbow. 55 Equally, different BIS criteria for the presence of lymphedema may be used, that is, L-dex scores of 10, 56 7.5, 43 7.1, 27 or 6.5, 57 with the latter three approximating an inter-limb ratio of mean + 2 SD. The impact of differing threshold is highlighted by the data of Fu et al., 27 who determined a sensitivity of BIS of 66% when adopting an L-dex cut-off of 10, which increased to 80% when using a criterion of 7.1 L-dex units. 27 Similarly, Hayes et al. 58 set BIS as the reference method, finding that the sum of arm circumferences method had only a 65% sensitivity; whereas Berlit et al. 59 observed a 75% sensitivity compared with circumferential measurements.
This range of reference tools and thresholds has led to misinterpretation or over-interpretation of the accuracy, or lack thereof, for BIS. 60 The lack of a single universal reference criterion is not unique to lymphedema assessment. Where no definitive reference method is available, alternative methods of analysis, such as maximum likelihood estimation, are recommended. 44 To date, these approaches have not been applied to assessing the predictive performance of BIS. Further, only a handful of studies have gone beyond calculating the sensitivity and specificity of BIS to determine its clinical utility for use in an individual patient. When the absolute accuracy of the reference to which BIS is compared is not known, it is not possible to state with certainty that BIS is more or less accurate than an assumed gold standard.
Sensitivity and specificity can be mathematically combined to determine positive and negative likelihood ratios (LRs). The LRs are a strong method for assessing the diagnostic accuracy and they allow the combining of diagnostic assessments in meaningful ways by using a diagnostic nomogram. 61 Dylke et al., 40 and others, 39 have found strong, clinically useful positive LR (9–13) and negative LR (0.3–0.6) for the use of BIS in determining the presence of lymphedema. This can elevate certainty in the diagnosis, such that if a patient has a low chance of developing BCRL, for example, 5% for patients who undergo a sentinel node biopsy, a single elevated inter-limb circumference difference provides a probability of BCRL of 50%. This increased to a predictive probability of 90% when combined with a positive BIS inter-arm ratio.
Although the terms “sensitivity” and “specificity” are most commonly used with respect to statistical analysis, they may also be applied to biological considerations. Measurement tools must be technically sensitive and specific to what they purport to measure. They should exhibit a low limit of detection and measure only the parameter of interest. A criticism of commonly used volume-based measures of lymphedema is that they may be detecting a simple change in tissue volume, rather than a change in fluid volume due to lymphedema. A virtue of impedance measurements made at a low frequency is that they are measuring the extracellular water. When impedance measurements are obtained along a limb, as for example the arm when assessing BCRL, the impedance measurements reflect mostly interstitial fluid, of which lymph is a primary constituent. Thus, though not measuring lymph directly, impedance measurements are very closely related to lymph volume and are, therefore, more sensitive to changes in fluid levels than volume-based measures of lymphedema. It has been calculated that in BCRL, whole arm impedance measurements are capable of detecting a change of as little as 35 mL in this volume. 62 This corresponds to a minimal detectable change of ∼0.04 units in inter-arm impedance ratio in patients with BCRL. 63
BIS in Clinical Practice
Over the past 20 years, BIS has moved from being a validated technology to a valuable tool in the screening, detection, and monitoring of lymphedema, particularly in the upper limb. The BIS has been used repeatedly in prospective screening programs to initiate early treatment, with the aim of reducing the incidence of established lymphedema.33,57,64 For example, Koelmeyer et al. found that patients prospectively assessed, from a pre-surgery point, by using BIS were less likely to develop lymphedema requiring treatment, and for those who did, the lymphedema was less severe.64,65 Growing evidence suggests that immediate intervention with simple, short-term conservative treatments once a change occurs in the BIS of 10 L-Dex points can lead to lower establishment rates for lymphedema.33,66–69 At this time, however, the utility of prospective BIS monitoring for developing lymphedema in other regions, including the lower limbs, has not been studied. 70
The use of BIS to assess lymphedema beyond whole arm measurements is constantly expanding. Protocols of measurements and normative data, and therefore diagnostic thresholds, for smaller segments of the upper limb, including the hand, are now available.37,71,72 Recently, a protocol for the assessment of breast edema was developed. 73 In this study, R0 was determined by using a polynomial curve fitting, rather than the standard Cole modeling, which was found to be less reliable to determine R0 in the breast. Further, the use of BIS for bilateral lower limb lymphedema is gaining further attention, with leg to arm R0 ratios, determined by receiver operating curve analysis, demonstrating strong sensitivity (0.65–0.89) and specificity (0.6–0.74).74,75
Conclusions
From the earliest theoretical suggested uses, impedance technology has matured to become an invaluable tool for assessing human physiological parameters such as body composition in nutritional studies. The past three decades have seen its use expand to the early detection and ongoing monitoring of lymphedema to the point where its use is recommended by national lymphedema organizations such as the National Lymphedema Network in the United States 76 and the Australasian Lymphology Association in Australia. 77 Early lymphedema surveillance using effective assessment tools such as BIS, in combination with other tools such as imaging modalities, such as ICG lymphography and lymphoscintigraphy, can be effective in reducing the incidence of lymphedema and provide more opportunities for therapeutic intervention, leading to improved quality of life for those with lymphedema. 78
The BIS was originally introduced as an aid to the early detection of breast cancer-related lymphedema; a purpose for which it is still extensively used. Over the past three decades, its application has extended to the assessment of lower limb lymphedema, typically following gynecological cancer 75 and most recently to the hand 37 and breast. 73 These latter uses have followed the original concept of using BIS to assess fluid accumulation but lymphedema is more than that, particularly in the later stages, where protein infiltration in tissue, fibrosis, and fatty accumulation may occur. A typical BIS scan accumulates 256 raw data points, each consisting of a value for impedance, resistance, reactance, and phase angle from which at least another five parameters, including characteristic frequency (fc), characteristic frequency impedance (Zc), phase angle at 50 kHz (PhA50), membrane capacitance (Cm), and alpha (the exponential parameter in the Cole equation that accounts for cell membranes being imperfect capacitors), may be derived; a wealth of this potential information has been largely unexplored. This is not the case in other conditions where PhA50, 79 alpha, 80 and Cm 81 have found prognostic utility. Preliminary studies have suggested that Cm, an index of cell membrane function, may have value in late-stage lymphedema assessment. 82 It is to be hoped that research in the next three decades may be as productive as the first, expanding the utility of BIS in lymphedema treatment.
Footnotes
Authors' Contributions
E.S.D. and L.C.W. equally contributed to the study conception and design, literature review, and article preparation.
Author Disclosure Statement
L.C.W. consults to ImpediMed Ltd. ImpediMed had no involvement in the design, undertaking, or article preparation of this study.
Funding Information
No funding was received for this review.