
Abstract
Background:
Lymphedema measurement is vital to select appropriate treatment and monitor its progress. Quantifying lymphedema in the head and neck area is challenging. The use of tissue dielectric constant (TDC) measurements has shown promising results in other body areas. This study aims to determine the test-retest reliability of a TDC measurement protocol developed for the head and neck area.
Methods and Results:
A detailed measurement protocol, including eight measurement points per side, was developed. Subsequently, the reliability of the protocol was tested in a sample of healthy participants (n = 50, 28 males). Using the LymphScanner (Delfin, Finland), participants were subjected to two measurement sessions. Each measurement point was measured three times per session. Test-retest reliability for each point was evaluated using intraclass correlation coefficients (ICCs) and standard errors of measurement (SEMs). Using the average of three measurements, reliability was good to excellent for all points (ICCs 0.81–0.95), with small measurement errors (SEMs 1.51–2.86). The reliability of a single measurement was moderate to excellent for all measurement points (ICCs 0.58–0.87), with larger, but still small, measurement errors (SEMs 1.65–3.39). When using single measurements, the lowest ICCs were found for the temporal (left 0.73 and right 0.67) and submandibular (left 0.58 and right 0.77) locations.
Conclusion:
Measurements with the LymphScanner, taken according to the developed protocol, are reliable in healthy participants. We recommend using the average of three measurements to optimize reliability. The protocol is fit for further testing in patient populations and for determining normal values in a larger scale study with healthy subjects.
Introduction
Head and neck lymphedema (HNL) affects between 35% and 75% of people treated for head and neck cancer.1–3 Patients suffering from HNL can experience pain; feeling of heaviness, tightness, or numbness; and reduced mobility. In addition, they have increased infection risk due to their lymphedema.2,4–6 Often, external lymphedema is accompanied by internal mucosal lymphedema, characterized by hoarseness and swallowing problems, sometimes leading to laryngeal dysfunction. Prolonged lymphedema is associated with structural changes such as adipogenesis, fibrosis, and chronic inflammation. 7
Despite the high prevalence, the subject has received relatively little attention in the scientific literature compared with breast cancer-related lymphedema. At the same time, serious challenges for managing HNL exist. One of these challenges is how to reliably quantify HNL for diagnosis and evaluation of treatment and for prospective surveillance in high-risk patients.
Currently, there is no generally accepted gold standard for measuring lymphedema. For the extremities, bioimpedance, spectroscopy, water volumetry, tape measurement, and perometry have shown good reliability and validity. 4 Measurement of HNL, however, is more complex. This is due to the anatomical shape, external structures (eyes, nose, and mouth), and internal structures (vessels, nerves, glands, and bone structures) that sit close together.
Research into the reliability, validity, and clinical applicability of measurement methods for the head and neck area is scarce.4–6 A few studies have studied measurement instruments for quantifying HNL, including clinician-administered assessment criteria and the use of computed tomography, ultrasound, tape measurement, or tissue dielectric constant (TDC).8–14 TDC has shown promising results for measurement of lymphedema in the breast region. 15
Mayrovitz et al. conducted several studies examining the reliability of TDC at various measurement points, including the face and neck.16–18 However, a structured and reliable protocol for HNL assessment using TDC measurement is still lacking. Therefore, we developed a detailed assessment protocol. The measurement protocol consists of eight measurement points per side of the head and neck. Each measurement point is measured in triplicate.
In this study, we studied the test-retest reliability of the protocol in healthy participants. As a secondary objective, we assessed the impact of taking single measurements, instead of triplicate measurements, on the reliability of the protocol.
Methods
Participants
In this cross-sectional test-retest study, we recruited a convenience sample of healthy participants. Eligible subjects were older than 45 years. For the purpose of this study, we considered participants to be “healthy” if they had never been diagnosed with and treated for head and neck cancer, had no other acute active disease, and did not have lymphedema in the head and neck area.
Exclusion criteria were active inflammatory skin condition in the face and/or neck, the presence of facial hair (as this hinders adequate contact of the LymphScanner with the skin), and use of medication that might affect local TDC values (i.e., systemic corticosteroids). A sample size of 50 participants was considered feasible and would yield adequate precision (i.e., sufficiently narrow confidence intervals [CIs]) under the expectation that reliability parameters would exceed 0.70. 19
The Dutch Central Committee on Research Involving Human Subjects (CCMO) confirmed that this study did not fall within the scope of the Dutch legislation on medical research with human subjects and that formal medical ethical approval was not required. Nonetheless, we adhered to medical ethical research principles. All participants were informed about the study and measurement methods and they provided written informed consent before participation in the study.
Measurements
We collected data on the following characteristics of the included participants: sex, age, body–mass index (BMI), skin type, alcohol use, smoking, and medication use. BMI was calculated (kg/m2) using weight measurements obtained using a digital scale with an accuracy of ±1% and the body length, as reported by each participant. Skin type was divided into six categories, according to the Fitzpatrick classification. 20
Habitual alcohol consumption was registered dichotomously (any vs. never) and in the average number of units per week. The smoking behavior of participants was classified as yes, no, or stopped. For those who smoked or had stopped, we calculated packyears (the average number of packs of cigarettes (or equivalent) smoked multiplied by the years during which the participant had smoked) based on self-report. Medication use included only medication that could potentially affect the amount of interstitial fluid (e.g., corticosteroids).
Local tissue water levels by TDC values were measured using the LymphScanner. This device generates electromagnetic waves at a frequency of 265 MHz and transmits them, through a coaxial probe, to the skin to a depth of 2.5 mm. The LymphScanner measures the TDC, which is then converted to a percentage water content value that can be read from the display on the device (Delfin, Finland).
All measurements were done by two skin therapy students and by the first author (C.R.A.), an experienced skin therapist. The researchers had been trained in the use of the LymphScanner and determination of measurement points according to the protocol. The measurements took place at the participants' homes. The temperature and humidity of the environment were registered. Participants were not allowed to wear a face cream or foundation and they were also not allowed to smoke, exercise, or drink a hot beverage an hour beforehand.
Measurement protocol
The measurement protocol includes eight measurement points per side. These points are located at the temporal, cheek, jawline (above and below the mandibular bone), submental, and neck regions. All points are related to easily distinguishable anatomic landmarks (Table 1; Fig. 1). Measurements are taken on both sides of the face, except for the submental measurement point (5c).
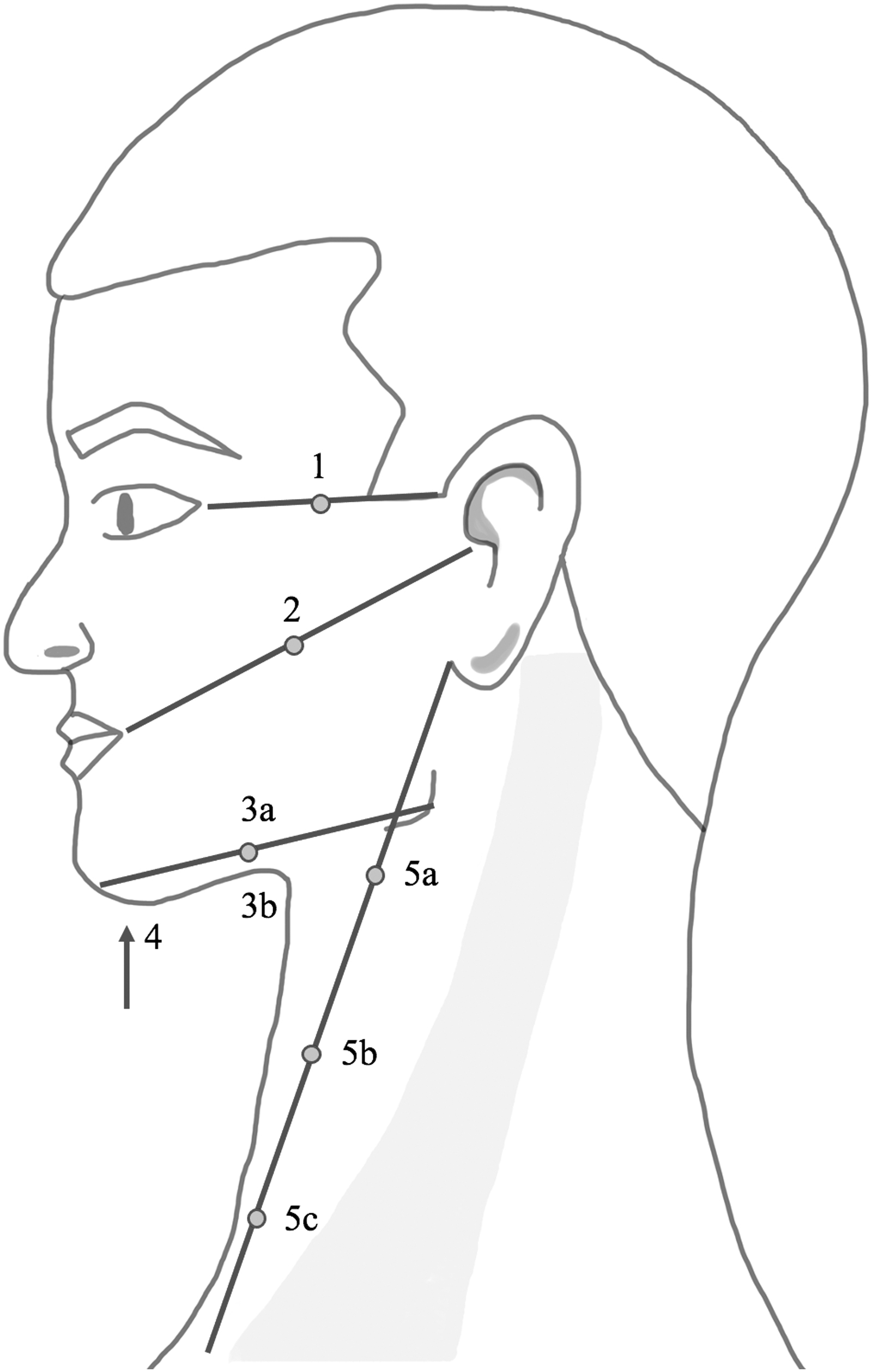
Visual reproduction of the measuring protocol. Dot, measurement point; line, determination of points.
Summary of Measurement Point Locations
SC joint, sternoclavicular joint.
Participants lie supine on a folding treatment bench for the measurements, with the head and cervical spine in neutral position. Each measuring point is determined using a tape measure and marked with a skin pencil. LymphScanner measurements are taken after 10 minutes of resting in the supine position to avoid influence on the measurement of skin reactions to palpation or marking.
One measurement session takes about 20 minutes. We performed two measurement sessions, measuring each point in triplicate in each session, using the “spot mode” of the LymphScanner. Specific attention was given to the pressure applied when placing the LymphScanner on the skin. The intention was to apply as little pressure as possible, by gently increasing pressure from an initial indication of “low pressure” on the device up to the point where a TDC value could be obtained.
The test-retest sessions were performed on a single day, with a minimum of 30 minutes and maximum of 60 minutes between sessions. Between the two sessions, participants remained at the measurement location. They did not drink hot beverages and were not physically active during that time. Between the two measurement sessions, the marked points were erased. Similar to the first measurement, the second measurement started with 10 minutes of resting in the supine position. Data were collected using Castor electronic data capture.
Statistical analyses
Data were analyzed using R software for Mac, version 4.0.2. Descriptive statistics were calculated to characterize the sample, using means and standard deviations (SDs) for numerical variables following a (near) normal distribution, medians and quartiles for non-normal numerical or ordinal variables, and numbers and percentages for categorical variables.
Test-retest reliability for each point was evaluated using intraclass correlation coefficients (ICCs) and standard errors of measurement (SEMs). To assess the decrease in reliability of the measurement protocol by taking single measurements instead of triplicate measurements, we calculated two ICCs for each point: one using the average of the three measurements, using a two-way, mixed, absolute agreement, average measure definition, and one based on only the first of the three measurements taken, using a two-way, mixed, absolute agreement single measurement definition. 21
An ICC smaller than 0.50, between 0.50 and 0.75, between 0.75 and 0.90, and greater than 0.90 indicates poor, moderate, good, and excellent reliability, respectively. 22 For measuring a group of patients, an ICC value of 0.70 is acceptable. For individual measurements that underlie clinical decision making, an ICC value of 0.90 is recommended. 19 Because TDC values may differ systematically based on sex, we performed a sex-stratified post hoc analysis of ICCs and SEMs and additionally calculated the mean absolute differences of each point for the sample as a whole as well as stratified by sex.
Results
Fifty participants (28 males and 22 females) were included. Their mean age was 60 years (SD 7; range 46–85) and mean BMI was 27.9 (SD 4.6; range 18.4–40.2) and 90% had skin type II or type III. Participant characteristics are shown in Table 2. Sixteen of the participants were medication free. Thirty-four participants were using medication (Table 2). None of the participants used topical corticosteroids in the head and neck area. During measurements, the mean room temperature was 20.3°C (SD 0.9; range 18.5–22), with mean humidity of 40.16% (SD 5.5; range 25–51).
Participant Characteristics
median [interquartile range].
BMI, body–mass index; SD, standard deviation.
For single measures, ICCs of the test-retest ranged from 0.58 (95% CI 0.358–0.734) to 0.87 (95% CI 0.782–0.926). The SEM varied between 1.65 and 3.39 (Table 3). The lowest ICCs, single measures, were found for the temporal spot (left 0.73 and right 0.67), submandibular spot (left 0.58 and right 0.77), and the highest point in the neck (left 0.772 and right 0.713). The average of three measurements resulted in good to excellent reliability for all points, with ICCs between 0.81 (95% CI 0.633–0.893) and 0.95 (95% CI 0.898–0.976). The SEM varied between 1.51 and 2.86 (Table 4).
Single Measurement of Percentage Local Tissue Water (Percentage Water Content)
95% CI, 95% confidence interval; ICC, intraclass correlation; L, left; R, right; SEM, standard error of measurement.
Average Measurements of Percentage Local Tissue Water (Percentage Water Content)
The post hoc sex-stratified analysis showed that in our research population, male participants have a higher mean value than female participants. Furthermore, in general, ICCs were somewhat lower and SEMs were slightly higher. The mean absolute differences between measurements in the full sample were mostly comparable to those in the subsamples (Table 5).
Post Hoc Analysis, Average Measurements of Percentage Local Tissue Water (Percentage Water Content) Stratified by Sex and Absolute Mean Differences
Discussion
This study aimed to determine the test-retest reliability of a TDC measurement protocol developed for the head and neck area in healthy participants. The reliability was good to excellent, indicating that the protocol could be used for repeated measurements on the individual level. The study also showed that reducing the number of measurements per point decreases the reliability for some points below a clinically acceptable level and should therefore not be recommended.
Insufficient reliability when taking single measurements was observed for some, but not all, measurement locations. The locations with lower reliability included the temporal region (location 1) and below the mandible (location 3b). Both measuring points are close to the bone, which may increase the influence of probe placement. In addition, earlier research mentioned that TDC points close to bones and tendons showed lower reliability and higher measurement errors and should therefore be used with caution. 23
The additional time needed to take the measurement in triplicate is ∼5 seconds per measurement, resulting in a total of 3 extra minutes. Considering the limited increase in time and the substantial increase in reliability, we believe this is worth the effort. However, we conducted our study in a healthy population. One might argue that the pressure applied during measurement could disperse some of the lymph fluid when lymphedema is present. This could then impact the validity and possibly the reliability in triplicate measurements. To investigate whether this is the case, further research should be carried out in a patient population with lymphedema after head and neck cancer.
Given the lack of previous reliability studies on TDC measurement in the head and neck area, we cannot directly compare our results with others. However, in patients with upper extremity lymphedema or lower extremity lymphedema, measurement of local tissue water has been described as a reliable technique.15,23–26 In addition, Jonsson et al. measured TDC values in the lower limbs in healthy women and men. The range of ICCs and SEMs in that study was similar to ours. 23
Recently, Mayrovitz et al. related head and neck TDC values to those measured in the extremities, in a nonlymphedema sample, in an attempt to provide normal within-patient reference values and diagnostic cutoffs based on TDC ratios. 27 The authors made no mention of the reliability of their protocol, and the protocol had not been published previously.
However, although not exactly the same, the measurement locations used in that study were very similar to those used in our protocol. We did not take measurements at the extremities, so we cannot compare TDC ratios of our sample with those found by Mayrovitz et al. Although the use of TDC ratios is an attractive approach because of its easy applicability, such ratios may be influenced by characteristics such as gender, skin type, and BMI.16,17
Indeed, in the post hoc analysis, male participants seemed to have higher TDC values than female participants. Although this did not clearly translate to systematic differences in reliability between male and female participants, for four of the measurement points, reliability was lower in male participants. A possible explanation could be that in men, the bone structures are more prominent at those locations, for example, the mandibular region.
Another explanation could be that despite shaving, a short stubble still influenced reliability of the LymphScanner measurement in men. The overall lower ICCs in the subgroups mostly reflect reduced variation, which is probably related to variation explained by sex as well as reduced sample size in the subgroups. With few exceptions, mean absolute differences were largely comparable for males and females, which suggests comparable reproducibility of the measurements.
However, these findings should be interpreted with caution since the stratified analysis was unplanned and therefore had a smaller sample size. In addition, other variables such as age and skin type may also influence TDC values. To fully appreciate the importance of such factors, a large study with sufficient variation is needed. Such a study could also provide reference values for healthy people.
Purcell et al. 10 studied the validity of MoistureMeter D, the earlier version of LymphScanner, for lymphedema assessment in the head and neck area. Using a single reference point, the submental location (our location 4), they showed that the outcomes were significantly different in an HNL group compared with a control group without lymphedema. In their study, they also presented the mean TDC scores for each level of the MD Anderson Lymphedema rating scale to assess the distinctiveness of lymphedema severity. A higher TDC score was associated with more severe lymphedema. 10 Although these findings support the construct validity of a single TDC measurement for evaluating HNL, we believe that a protocol including multiple locations should be preferred. In particular, when using the TDC measurements for prospective surveillance, early lymphedema may be missed if the measurement is restricted to a single location. In addition, even chronic lymphedema can manifest in one place and not in another.
The measurement protocol used in this study was developed based on clinical expertise and earlier reported landmarks in the face.8,10 The eight measuring points per side are intended to cover all the different parts of the face and neck. A recently published study, which was conducted during the same time as our study, used only four measurement points in the head and neck area.
These points correspond closely, although not exactly, to four of the measurement points used in our protocol. 28 The reliability estimates in that study were somewhat lower and with wider confident intervals compared with our findings, which might be due to sample variation, longer time between the two measurements, and differences in standard operating procedures (e.g., positioning of patients).
Obviously, including more measurement points provides a more comprehensive picture, but it comes at the cost of a longer measurement time. Which measurement points are most relevant in clinical practice, that is, in terms of sensitivity to change or correlation with other outcomes such as body image or function, could be a topic for further investigation, preferably in prospective longitudinal studies.
Limitations and strengths
Although we used a convenience sample of healthy participants, we kept an eye on gender balance and invited participants within an age range similar to that which could be expected for a head and neck cancer population.
While none of the participants had acute active disease, some of them did use medication for chronic conditions. This is as expected given the prevalence of chronic disease in a relatively older population. In addition, the use of medication that would likely affect TDC values was an exclusion criterion. Still, we would not recommend clinicians or researchers to consider the TDC values obtained in our study as reference values for future use.
The measurements for this study were carried out during the COVID-19 pandemic. This introduced logistical issues that led us to take measurements at participants' homes, which introduced differences in temperature and humidity across participants. However, we compared measurements within individuals, and all measurements were taken within 4 months of each other.
In addition, post hoc analyses of our data did not show correlations between the TDC values and the temperature or humidity. Therefore, we do not expect that these circumstances biased the reliability estimates. Nevertheless, when applying the protocol for longitudinal analyses in clinical practice, we would recommend performing measurements under comparable conditions.
Over longer measurement intervals, when temperature and humidity show larger variation, a correlation of these variables with TDC values may still exist, which would then affect the comparability of repeated measurements. To ensure generalizability to clinical practice, we used a folding treatment bench, which ensured that every participant had the same starting position, similar to what would be used in a clinical setting.
Conclusion
This study shows that the described assessment protocol is reliable in a nonlymphedema population. Using triplicate measurements is worth the additional effort. The protocol is fit for further testing in an HNL population. In addition, further research is recommended to obtain normal values in a large and heterogeneous population and explore which participant characteristics influence TDC values.
Footnotes
Acknowledgments
The authors are very grateful to Mandy van Schuppen and Diba Snijder for participating in the measurements. The authors thank the Verwelius Foundation for the financial support.
Authors' Contributions
C.R.A. was involved in methodology (lead), formal analysis, investigation, and writing—original draft. L.v.d.M. and M.W.M.v.d.B were involved in supervision, writing—original draft (supporting), and writing—review and editing (equal). M.M.S. was involved in supervision, methodology (supporting), writing—original draft (supporting), and writing—review and editing (equal).
Author Disclosure Statement
The authors have no conflicts of interest to declare.
Funding Information
This study received financial support from the Verwelius Foundation.