
Abstract
Background:
Approaches to screening, assessment, and treatment of breast cancer-related lymphedema (BCRL) vary widely. We evaluated overall quality of clinical practice guidelines (CPGs) for managing BCRL using the Appraisal of Guidelines for REsearch and Evaluation II (AGREE II) tool, and relevance of consensus recommendations for the Canadian health context.
Methods and Results:
We searched electronic databases, gray literature, national lymphedema frameworks, and expert opinions, to identify lymphedema CPGs, printed/published from January 2013 to October 2021. Using AGREE II, six health care professionals reviewed CPGs for consensus. Domain-specific AGREE II quality consensus scores were required (≥70% for Rigor of Development; ≥ 60% for Stakeholder Involvement and Editorial Independence; and ≥50% for Clarity of Presentation, Applicability, Scope, and Purpose). Results and overall recommendations from the CPGs were summarized and synthesized. Nine CPGs met inclusion criteria for review. Wide variability of evidence-based recommendations, and limited clinical considerations were found. Scope and Purpose, and Clarity of Presentation were adequate in six of nine CPGs; Stakeholder Involvement in seven of nine CPGs; and Editorial Independence in three of nine CPGs. Across all CPGs, Applicability was minimally reported. Only the Queensland Health CPG met quality consensus scores for Rigor and Development; however, the focus was limited to compression therapy.
Conclusions:
No CPG reviewed could be adopted for the Canadian health context. The proposed Canadian BCRL CPG will focus on stakeholder engagement, methodology, and implementation/evaluation. Using AGREE II allowed for assessment of quality of methods used to develop identified CPGs from other countries before consideration of adoption in a Canadian Context.
Introduction
Breast cancer-related lymphedema
In North America, one in five women living with breast cancer develop breast cancer related-lymphedema (BCRL), a secondary lymphedema occurring when the lymphatic system is damaged or disrupted following cancer and/or cancer treatments. 1 While BCRL is considered chronic and incurable, research points to more successful management with early diagnosis and treatment. 2 For individuals undergoing treatment for breast cancer, efforts focus on reducing risks; for those who have already developed BCRL, attention shifts to ongoing management.3–5 Considerable variation is found in clinical and rehabilitative approaches, and in the evidence bases supporting lymphedema screening, assessment, and treatment practices. 6 To improve delivery and quality of care for individuals with, and at risk of BCRL, there is a need for systematically developed recommendations using best research evidence. 7
Clinical practice guidelines
Clinical practice guidelines (CPGs) are systematically developed directives that contribute to enhancing standards of health care. 8 For more than two decades, CPGs have been developed to support health professionals' decision making for lymphedema management. Development of guideline appraisal tools and improvements in research and practice methods have resulted in increasing attention to evaluating methods in CPGs. 9 Because the quality of CPGs varies, appraising and rating the quality of content are critical. Health care professionals should be able to rely on CPGs to assist in formulating decisions for patient care, and health policy makers should be able to use CPGs to identify areas of importance. High standards of rigor in CPGs ensure that information is accurate and effectively targeted to appropriate audiences, and that recommendations and directives are rooted in the utmost quality of information. 9
Guideline appraisal
To evaluate quality, methodological approach, and transparency of recent CPGs in the area of BCRL, the Appraisal of Guidelines for Research & Evaluation II (AGREE II) Instrument was utilized. The AGREE II tool enables reviewers to appraise a CPG through consensus scoring across 23 questions, each rated from 1 to 7 (strongly disagree to strongly agree), in six key domains. 10 The six domains of CPG assessment in the AGREE II tool include the following: Scope and Purpose, Stakeholder Involvement, Rigor of Development, Clarity of Presentation, Applicability, and Editorial Independence. 10 Reviewers also provide ratings and recommendations for overall assessment and potential use of the CPG in context.
The AGREE II tool is intended to be used with a small group (approximately four reviewers). 11 Domain- specific threshold scores, calculated to quality consensus percentages, are recommended to ensure that only high-quality CPGs are used in making recommendations for proposed CPGs. 12 The inclusion of CPG assessment tools, such as the AGREE II, results in higher standards of rigor, transparency of communication, and quality of recommendations. 13
For over 20 years, a Canadian CPG has supported medical and conservative decision making for diagnosis and management of BCRL in Canada. 14 Given advances in breast cancer medical treatment and additional scientific research in lymphedema, an update to the 2001 CPG is warranted. The proposed evidence-based update to the Canadian BCRL guideline is an initiative of the Canadian Lymphedema Framework (CLF) in partnership with the Oncology Division of the Canadian Physiotherapy Association, and Cancer Care Alberta's Guideline Resource Unit (GURU). 6
Objectives
This article presents a critical review of existing CPGs using the AGREE II to explore and evaluate the quality and transferability of these CPGs to a Canadian health care context, with the objectives of (1) evaluating overall quality of CPGs for the management of BCRL and (2) determining relevance of reviewed CPGs for adoption or use in updating the Canadian BCRL CPG.
Methods
Search strategy
A research librarian (L.D.) conducted a search for published and unpublished studies (in any language) from January 1, 2013, through October 31, 2021. The search extended across electronic databases, including MEDLINE, EMBASE, SCOPUS, CINAHL, Proquest Dissertation and Theses Global, PEDro, Cochrane Library (Cochrane Central Register of Controlled Trials, Cochrane Database of Systematic Reviews), and TRIP PRO database.
Published literature, including CPGs, systematic reviews and randomized controlled trials describing diagnosis, risk reduction, and management and measurement outcomes involving individuals with breast cancer of any age who have or are at risk of developing lymphedema, was searched. Unpublished research was also included (i.e., proceedings from lymphedema conferences, searches of websites housing clinical trial details, theses and dissertations, as well as hand-searches through the reference lists of all potentially relevant studies). Experts were contacted through email or telephone to identify relevant articles.
CPGs were shortlisted to include only those containing (i) explicit recommendations and evidence-based examples; (ii) a focus on patient care level; (iii) a nonbiased funding source; and (iv) BCRL-specific recommendations.
Exclusion of guidelines was deemed appropriate where (i) cancer-specific CPGs included lymphedema as a secondary focus; (ii) CPGs were reviews, not guidelines; (iii) CPGs were based only on expert opinion or consensus, without research-based foundation; (iv) CPGs were manuals for care or education; and (v) complete versions were unavailable.
Research team
The CPG review team (hereon referred to as the management team) included health care professionals in the fields of lymphedema rehabilitation, BCRL rehabilitation, implementation science, and rehabilitation science, from the disciplines of physical therapy (M.L.M, L.L.R., M.A.O., H.G., K.L.C., and S.R.H.), occupational therapy (N.D.D.), kinesiology (J.F.P.), library sciences (L.D.), and medicine (D.K.). H.G. provided an international perspective, while the remaining team members were based in Canada.
Data extraction, synthesis, and assessment
After preliminary screening for title relevancy by authors (M.L.M, M.A.O., and J.F.P.), CPGs were shortlisted. After further screening for topic-specific relevancy (M.L.M. and N.D.D.), CPGs not explicit to lymphedema were removed, resulting in the final list of CPGs for review and evaluation using the AGREE II tool.
Guiding clinical questions
Four key guideline categories for BCRL were determined by group consensus before review, specifically,
Diagnosis – focusing on sensitivity and specificity;
Risk reduction – focusing on strategies and practice for mitigating risk of incidence;
Effective lymphedema management – focusing on limb volume;
Measurement outcomes – focusing on valid, reliable, and sensitive methods for detecting and monitoring lymphedema, and surveillance timelines.
Through these four categories, the management team focused on key areas of importance when reviewing the CPGs using the AGREE II tool. 6 Table 1 describes the questions and their rationale.
Key Clinical Questions & Rationale
BCRL, breast cancer-related lymphedema.
Use of the AGREE II tool for consensus and review
Before meeting as a group, all reviewers completed AGREE II tool training. 10 The management team met before performing the appraisals to build competency and comfort with using the AGREE II tool. The three CPGs excluded from the initial 12 CPGs were reviewed by the management team as an opportunity to gain experience using the AGREE II tool. The nine included CPGs were then reviewed by three consistent reviewers (M.A.O., J.F.P., and N.D.), with a fourth additional reviewer (M.L.M., L.L.R., or H.G.). Guidelines were independently reviewed and scored across the six domains of the AGREE II tool. Comments were attached to specific AGREE II tool responses to allow understanding of individual reviewer's approach to scoring. Overall, scoring ranked from 1 (lowest quality) to 7 (highest quality).
In the case of discrepancies (standard deviation [SD] >2) on any single item, the group discussed reasons for the discordance with the aim of reaching consensus. The discussion also allowed for expansion on clinical relevance related to developing updated Canadian BCRL CPG. Consensus was met when the group ranking the individual question fell within or below a difference of two SD across all reviewers.
Overall quality scores for each CPG were obtained from tallied raw scores, assessed and scaled according to instructions provided in the AGREE II tool. 10 Following evaluation of the overall quality of each CPG using the AGREE II tool, comments and recommendations were collated for the purpose of discussion in this article; CPGs were ranked comparatively for their relevancy and usefulness from a Canadian health care perspective. Overall CPG consensus was met when the average total score of each reviewer fell within or below two SD.
For transparency of decision making and to ensure confidence in recommendations adapted from existing CPGs, a quality consensus score of ≥70% in the domain of Rigor of Development on the AGREE II tool was required. Quality consensus scores were set at ≥60% in the domains of Stakeholder Involvement and Editorial Independence, and ≥50% for all other domains.15,16 Overall mean quality scores were set at >50%, or >3.5/7 overall. 15
Relevance for a Canadian context
Each CPG was then evaluated by all reviewers in terms of relevancy for informing the proposed update to the Canadian CPG, including (1) up-to-date literature, (2) use of the GRADE system to determine certainty of evidence, 16 and (3) appropriateness of recommendations for use in a Canadian public health context. Group consensus was achieved through discussion where disagreements arose.
Results
Search outcomes
The database searches yielded 4568 references imported for screening, with 2371 duplicates removed. No further evidence was derived from gray literature, national frameworks, or expert opinion. Then 2287 studies were screened against abstract and title, with 1284 further studies excluded. Full text screening of the remaining 1003 articles yielded 656 further exclusions. After full review of the remaining 347 articles, 335 were excluded for not being or including CPGs. Twelve articles met the inclusion criterion of a CPG. Following title and abstract screening of these 12 CPGs, three were removed, with nine CPGs eligible for inclusion in the appraisal. Figure 1 depicts search strategy and article yields.
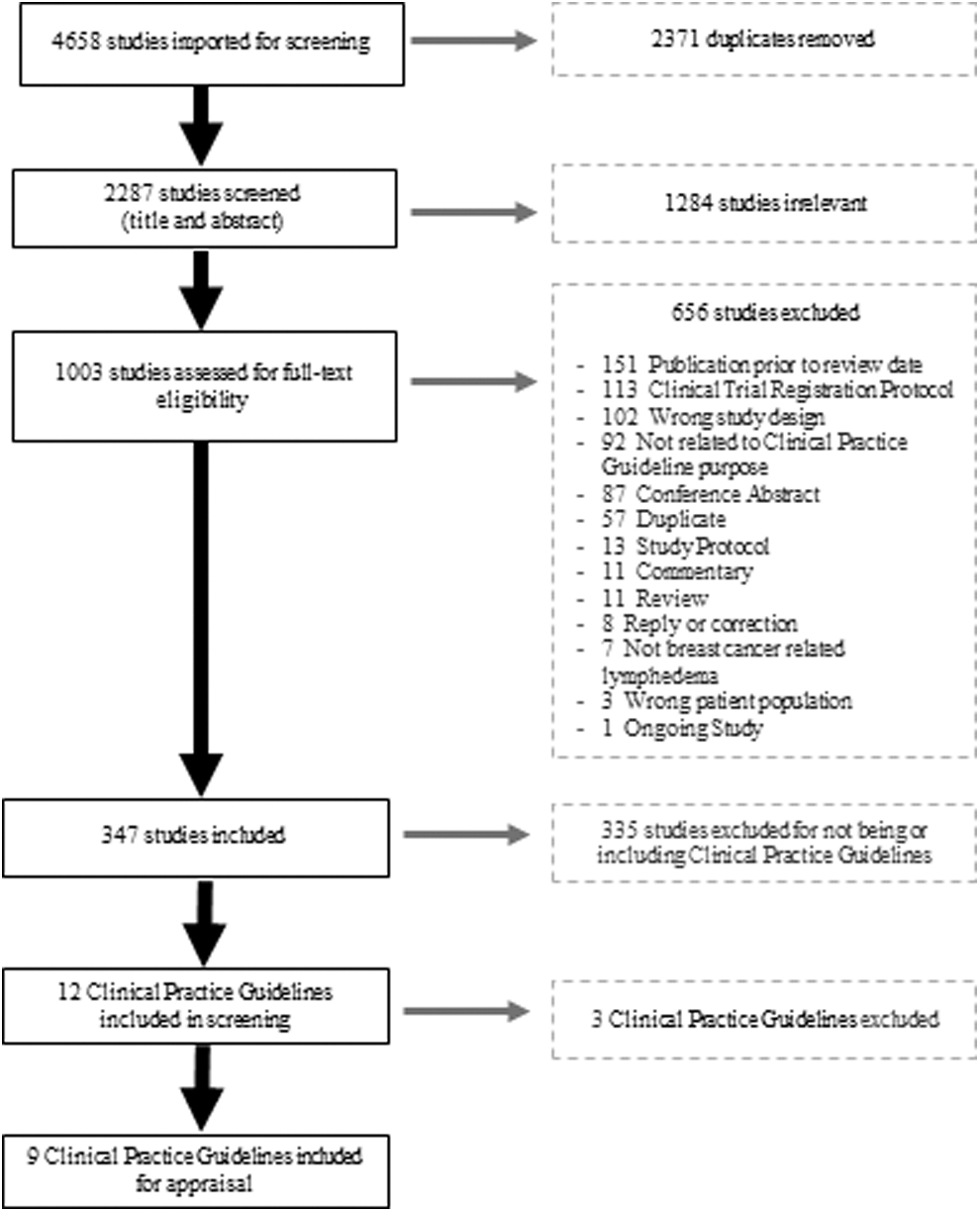
PRISMA flow diagram – search results.
These nine CPGs included a broad array of international guidelines from the following organizations: the International Society of Lymphology (ISL), an international collaboration; two from the American Physical Therapy Association (APTA), United States; the Dutch Society of Dermatology, Netherlands; the Oncology Nursing Society (ONS), United States; Association of the Scientific Medical Societies, Germany; Queensland Health, Australia; and two from the American Society of Breast Surgeons (ASBrS), United States.17–25 A summary of these CPGs appears in Table 2.
Quality Consensus Thresholds Met by Domain and Overall Recommendation
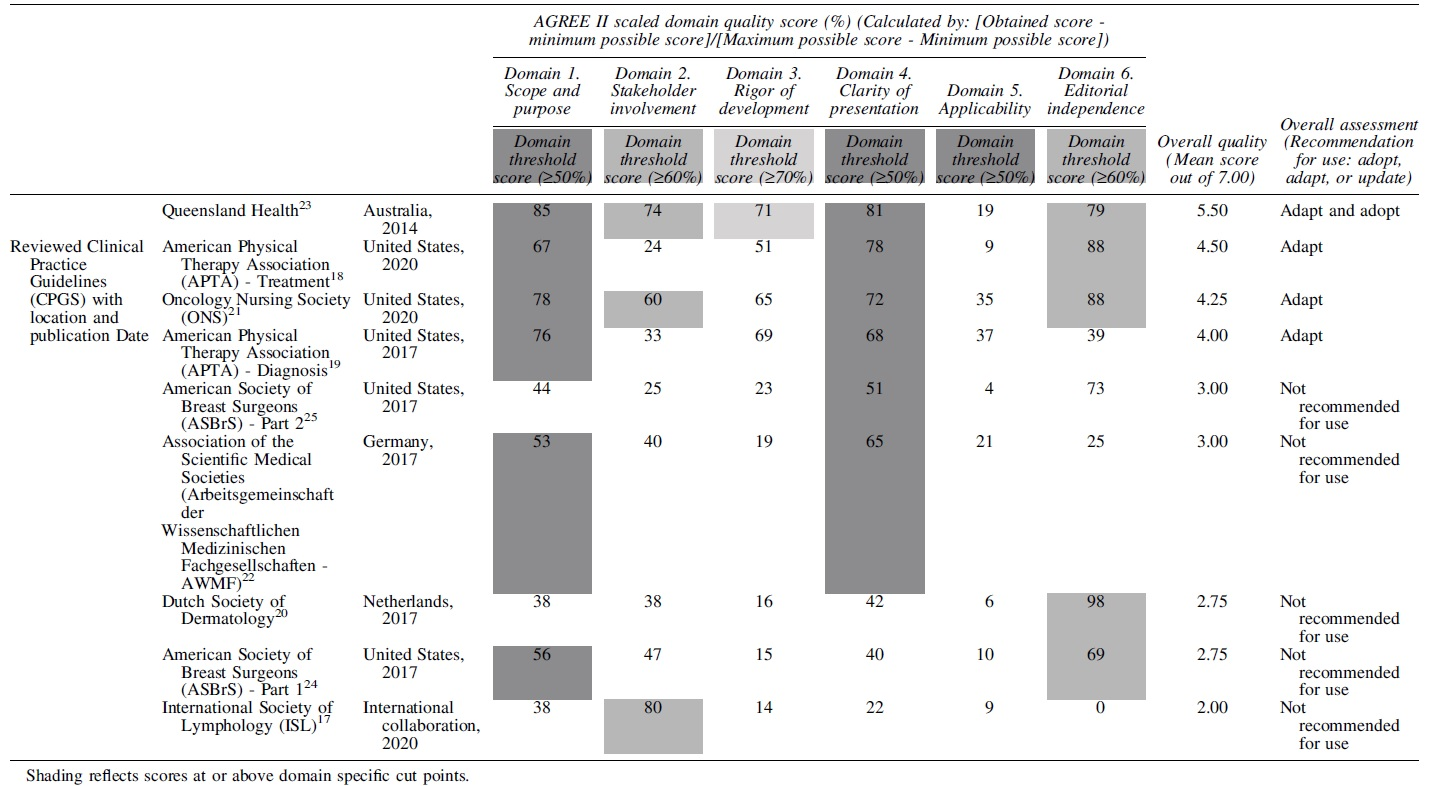
AGREE II domain outcomes
Table 2 depicts the specifics of each CPG within the AGREE II domains, which are reviewed in detail in the sections below. Figure 2 shows the interquartile ranges of domain scores, demonstrating how the nine CPGs varied across the overall AGREE II domains, with some domains showing more variability in scores than others.
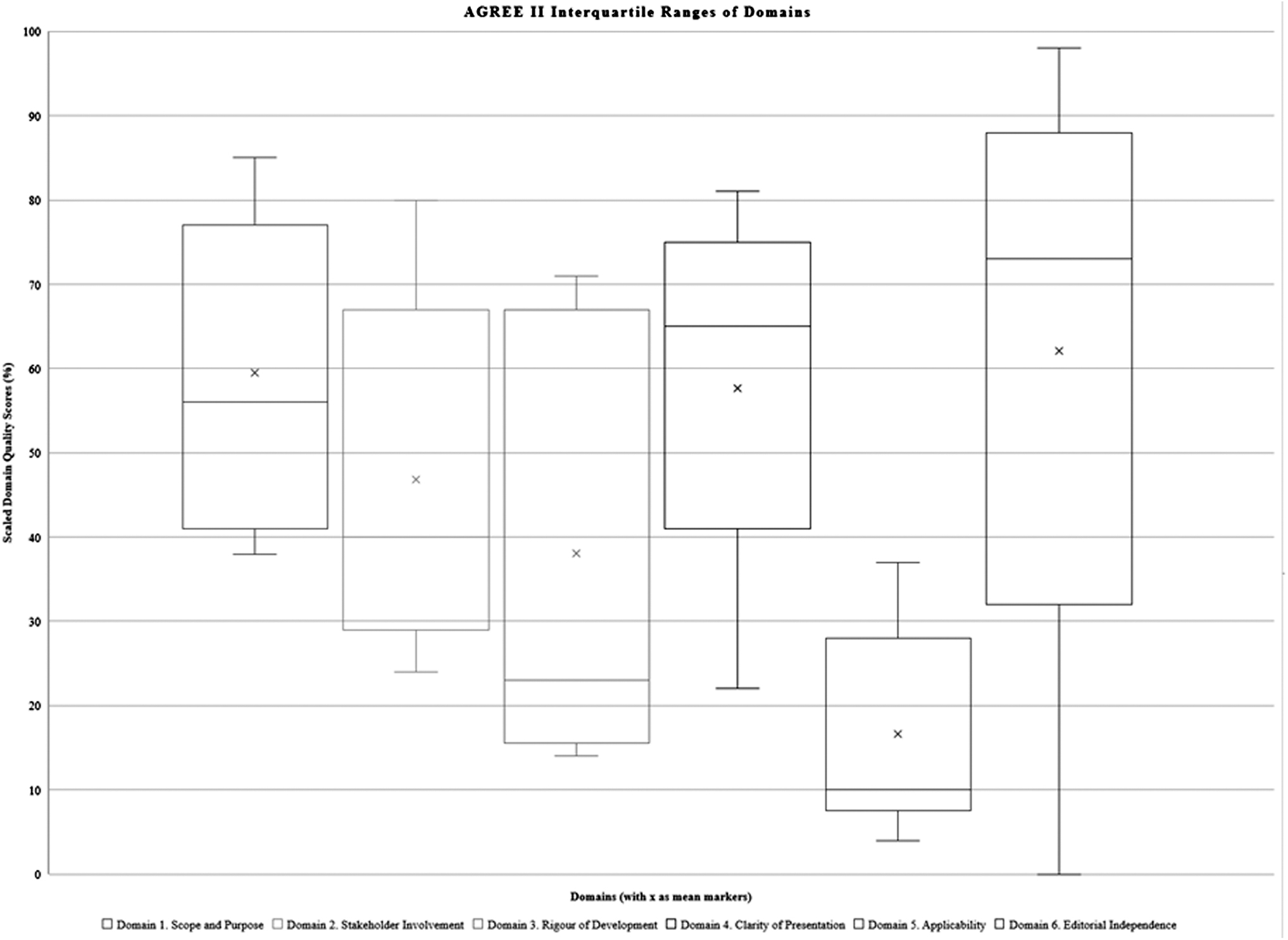
Interquartile range of domains.
Scope and purpose
Six CPGs met the threshold criterion of a quality consensus score of ≥50%.18,19,21–24 Using the AGREE II tool, all the CPGs identified the focus as being lymphedema, and the scope of these guidelines was consistently described. However, management team consensus found that there was no consistent explanation of the purpose; only four of nine CPGs described their clinical questions and population.18,19,21,23 In the remaining reviewed CPGs, our management team consensus found that scope and purpose were broadly defined at the start, but then not specifically addressed in the recommendations.17,20,22,24,25
Stakeholder involvement
Three CPGs met the threshold criterion of a quality consensus score of ≥60%.17,21,23 While all the CPGs targeted lymphedema populations, it was not consistently clear how the stakeholders, or target population, were actually involved in the process, making it difficult to explain stakeholder engagement. Furthermore, most CPGs reviewed did not clearly define their expected users, or how their guideline was intended for use.18–20,22,24,25 Some CPGs that offered a wider audience as the guideline target had limited follow-through with recommendations that targeted all of these intended audience groups; for example, the ONS guideline targeted a broader range of health care professionals, while the actual recommendations were primarily focused on nursing. 21
Rigor of development
Only one CPG met the threshold consensus quality score of ≥70%. This was the Queensland CPG, which provided strong rationale and recommendations based on rigor. 23 Most reviewed CPGs did not clearly describe the systematic methods used to search for evidence, nor how evidence was selected for use.17,20,22,24,25 While the ONS CPG used systematic reviews, an indication of rigor, their search strategy for obtaining the reviews was unclear. 21 In most CPGs, it was unclear how recommendations were determined; there was a need to infer that clinical expertise and experience were utilized, although these methods were not explicit.17–22,24,25 Stemming back to limitations in explaining scope and purpose, the information regarding health outcomes was often unclear.17–22,24,25 Most CPGs did not include clear external review or plans for ongoing updates to remain current.17–22,24,25
Clarity of presentation
Six CPGs met the threshold consensus quality score of ≥50/%, with the Queensland CPG having the highest-rated presentation and format.18,19,21–23,25 The recommendations were most difficult to follow in the ISL CPG, and easiest to follow in the Queensland CPG.17,23 Overall, there was great variability in how management and key recommendations were presented, with some CPGs having much more user-friendly readability than others.18,19,21–23,25 Formatting and text arrangement played a large role in the quality rating.
Applicability
No guideline met the threshold consensus quality score of ≥50%. None of the CPGs reviewed adequately described facilitators and barriers to application. Limited details were offered on translation into practice and ongoing auditing. The exception was the Queensland CPG, which used compression garment funding algorithms to explain how the CPG would be used to change health care practice, however, this was not sufficiently described for the readers. 23
Editorial independence
Five CPGs met the threshold consensus quality score of ≥60%.18,20,21,23,24 The disclosures for funding and influence were typically well described, although two CPGs were very limited in explaining affiliations.17,22 The approach to consensus and collaborative approach by the CPG team members were overall well described in most of the reviewed CPGs. In particular, the Dutch CPG very clearly explained the group members and influences, with a threshold consensus score of 98%. 20
Overall assessment
There are two aspects of this section, the overall quality rating of the CPG and whether it was recommended for use or not. The mean scores of overall quality varied across the CPGs, with lower quality scores of 2/7 for the ISL, 2.75/7 for the Dutch guideline, and 2.75/7 for the ASBRS Part 1.17,20,24 Although moderate in overall quality rating (3/7), the ASBRS Part 2 and the AWMF were not recommended for use.22,25 Higher-quality rated CPGs included 4/7 for the APTA Diagnosis, 4.25/7 for the ONS, and 4.5/7 for the APTA Treatment; these CPGs were recommended for use with modifications.18,19,21 The highest quality ranking was 5.5/7 for the Queensland CPG, which was also recommended for use with modifications. 23
Alignment to planned updated Canadian CPG
The four highest rated guidelines—the Queensland CPG, APTA Treatment, ONS, and APTA Diagnosis—were then evaluated in terms of relevance for use in a Canadian public health context18,19,21,23; Table 3 depicts the alignment of the CPGs. No CPG met the criterion for adoption. All four CPGs were deemed to be up-to-date (within 1 year) in terms of literature to publication date. In terms of their use of GRADE recommendations, only the Queensland CPG reported evidence-based recommendations. 23
Alignment to a Canadian Context Across High Quality-Rated Clinical Practice Guidelines
The relevancy for use in a Canadian public health context was only clearly met by the Queensland CPG. 23 Overall, the recommendations for use—as measured through consensus to adopt, adapt, or update the reviewed CPG—were to: adopt and adapt compression therapy aspects of the Queensland CPG 23 ; adapt the treatment and management approach sections of the APTA Treatment CPG 18 ; adapt the treatment section of the ONS CPG 21 ; and adapt the diagnostics information from the APTA Diagnosis CPG. 19
Discussion
Main findings
An important finding derived from using AGREE II was that the majority of CPGs did not meet established quality standard in terms of sufficient rigor to adopt for use in a Canadian context. We found variability in quality of CPGs across the AGREE II domains, with the majority of CPGs rated as low quality, and the most frequent response for adoption recommendation as “no.” Similar results have been reported in appraising quality from other CPGs in the clinical rehabilitation and lymphedema fields.8,26
There is opportunity for improvement of quality of CPG development. Specifically, attention on the domains of Applicability and Rigor of Development would improve the overall application of CPGs. Use of standard approaches and/or tools in the development stage of CPGs would ensure consistent approaches to CPG protocols and presentation. For example, while the ISL was originally written before the development of the AGREE II tool, and includes valuable information on the grading and staging for lymphedema, the current update for this CPG is lacking transparency, making it impossible to evaluate rigor, and decision making around recent modifications to recommendations. 17
Engagement and applicability in BCRL CPG development
Including experts from clinical or patient populations in CPG development is considered key to quality and intended use. 27 Defining the intended context for use is also crucial to ensuring CPGs align to practice. Definitions related to the target audience, required training, and intended use of reviewed CPGs were often vague or too broad, leading to challenges in assessing the quality of recommendations and clinical application. The Queensland CPG was the most explicit in describing clinical applicability. 23 We recommend having a clear and transparent stakeholder focus (of both the health care population and the target user group), combined with clinically relevant measurable endpoints, to ensure that a CPG functions to serve the population, condition, and goals it was developed to address.
Adoption considerations
Examples of recommendations missing from the reviewed CPGs, but highly relevant to adoption, would be inclusion of more functional details in assessment, practice, and guidance; specifically, consideration of hand dominance (in relation to the affected upper extremity), use of standardized clinical examination tools for diagnosis, and inclusion of a broader location of swelling beyond just the arm and hand (e.g., chest wall, trunk, and back). In addition, technology advances should be considered for current and future CPGs; use of knowledge translation and clinical practice tools—to improve access as well as standards for surveillance—such as e-health platforms, e-assessments, and virtual health care options, should be explored as part of establishing context for adoption of a CPG.
A more standardized national approach to the delivery of needed services and the provision of compression garments would help to improve access and equity across regions. Finally, formatting and layout are important factors that should be developed with the support of stakeholder and end-user (health care professional) engagement, to ensure that recommendations are presented in a format that meets the needs of the intended audience.
Utility and limitations of the AGREE II tool
While the AGREE II tool provides opportunities to objectively appraise CPGs with a standard of quality, the tool has limitations.
Quality
In terms of quality, the ratings and categories do not translate well for older CPGs, such as the ISL. The AGREE II tool does not offer a method of bridging or transitioning older CPGs into the current standard of quality. The AGREE II tool is limited in rating the quality of sources of recommendations, requiring use of additional tools after overall consensus has been reached.
Applicability
As to applicability, there is an issue in AGREE II scores of those CPGs that are more specific and directed in their objectives versus a CPG with broader aims. CPGs with more specific audience and goals will likely score higher than CPGs that have broader audiences and less specific goals (i.e., a goal to broaden awareness will score lower because it is less objectively measurable, despite being a reasonable intent of a CPG). For example, despite addressing fewer categories of recommendation than many other reviewed CPGs, a positive consequence of the Queensland CPG was its focus on compression therapy alone; thus, it scored higher in quality as it met its objectives. 23
Adoption
After appraising the quality of a CPG, challenges exist in aligning recommendations to the context of its intended use in practice. The AGREE II tool is not meant to be used to guide the tailoring, modification or adoption of a CPG, but must be used in conjunction with other tools, such as the Appraisal of Guidelines for Research and Evaluation–Recommendations Excellence (AGREE-REX) and/or ADAPTE.28–30 Tools such as the AGREE-REX instrument can be used as a next step, to ensure recommendations are utilized in the CPG adaptation process.28,29 After determining quality of recommendations, the process of tailoring a CPG requires methodologically informed practice, with the use of a tool such as the ADAPTE methodology 30 ; ADAPTE facilitates adoption of components from appropriate CPGs. 30
Strengths and limitations
The strength of our work appraising guidelines included our interdisciplinary research team, including a team member (S.H.) with previous involvement in developing the initial Canadian CPG. Limitations of our work included the relatively low number of published CPGs meeting our inclusion criteria, only one CPG meeting the standard for rigor, and no CPG found to be directly adoptable for use in a Canadian health care context.
Conclusion
Development of a high-quality CPG to provide recommendations on diagnosis, risk reduction, and management for individuals with BCRL is warranted. The quality of current BCRL CPGs varies greatly, being generally of lower quality. Using the AGREE II tool for appraisal of the nine included CPGs offered opportunity to explore quality, applicability, and potential for adoption. While no reviewed CPG could be adopted into the Canadian context, some aspects of the included CPGs could be recommended for use with updates and adaptation.
Footnotes
Authors' Contributions
All authors contributed substantially to conception and design and drafted the article or revised it critically for important intellectual content. All authors gave final approval of the version to be published and agreed to act as guarantor of the work.
Author Disclosure Statement
Lori Radke and David Keast are members of the editorial board for the Pathways Magazine of the CLF.
Funding Information
Naomi Dolgoy was supported by a Mitacs Accelerate postdoctoral fellowship.