
Abstract
Background:
The natural history of venous malformation (VM) and Klippel–Trenaunay Syndrome (KTS) has not been quantitatively studied. To obtain benchmarks to guide designing clinical trials to assess safety and efficacy of novel drug candidates, the clinical course of the patients was followed for 6 months.
Methods and Results:
This is a multicenter prospective observational study evaluating the change rate in lesion volume from baseline with magnetic resonance images, as the primary endpoint. In addition, disease severities, performance status (PS), pain visual analog scale (VAS) score, quality of life (QoL), infections, and coagulation markers were also evaluated. Thirty-four patients (VM = 17, KTS = 17, 1–53 of age; median 15.9 years) with measurable lesion volume were analyzed. There was no statistically significant difference in the lesion volume between baseline and day 180, and the mean change rate (standard deviation) was 1.06 (0.28). There were no baseline characteristics that affected the change in lesion volume over 6 months. However, there were patients who showed more than 20% volume change and it was suggested that the lesion volume was largely impacted by local infection. There were no statistically significant changes in pain VAS score, severity, PS, QoL score, D-dimer, and platelet count over 6 months within all patients analyzed.
Conclusion:
The results showed the representative natural course of VM and KTS for a 6-month period with objective change of lesion volume and other factors, suggesting that it is scientifically reasonable to conduct a Phase 2 proof-of-concept study without a placebo arm, using the results of this study as the control.
Clinical Trial Registration:
NCT04285723, NCT04589650.
Introduction
Venous malformation (VM) and Klippel–Trenaunay Syndrome (KTS) are both orphan indications and their incidence is reported to be 1–2 in 10,0001 and 1 in 100,000 live births, 2 respectively. VM is a congenital lesion, which mainly consists of irregularly dilated vein, in which low-pressure and slow-flow blood goes through, with abnormal wall structure. VM can be developed in any part of the body, including the head and neck, trunk, and extremities. The diseases present across a wide range of ages from infants and schoolchildren to adulthood, and symptoms progress or deteriorate owing to growth and external stimulations.3,4 KTS is diagnosed by fulfilling two of the three major criteria: (1) having a port-wine stain due to a capillary malformation of the skin, (2) having slow-flow vascular malformations, and (3) overgrowth and hypertrophy of one or more extremities. 5 Vascular lesions and hemihypertrophy associated with KTS are observed at birth and exacerbated with age and growth in many cases. The major complaints include local pain, fever, infection, bleeding, and disfigurement.
In addition to these symptoms, dysfunction and cosmetic problems significantly reduce the patient's quality of life (QoL) throughout their lifetime. Giant lesions of VM and KTS often cause localized intravascular coagulopathy (LIC), consuming a large amount of coagulation factors in the lesion and forming thrombus. Thrombus in the lesion induces acute or chronic inflammation that causes pain and swelling, and worsens LIC gradually developing fibrosis.
The primary treatments of VM and KTS include surgical resection, sclerotherapy/embolization, and laser therapy.3,4 As most of them are invasive and there are many patients who are not applicable to any of these primary treatment options, there are significant clinical needs for pharmacotherapies. Recently, rapamycin (sirolimus) and alpelisib showed clinical efficacy in patients with VM and KTS in small cohorts.6–9
Empirically, the lesions do not resolve spontaneously and most patients with VM and KTS experience a slowly progressive disease course. 10 However, there are no prospective or retrospective studies on the natural history of VM and KTS that quantitatively evaluated the lesion volume and other clinical measures. To develop novel drug candidates for the diseases, it is important to identify the clinical measures to serve as endpoints for clinical trials and to obtain benchmarks to guide designing clinical trials to assess safety and efficacy of novel drug candidates for the diseases. Therefore, the multicenter prospective study was conducted to observe the natural course of the patients for 6 months, in which data were obtained on objective measures such as the change in lesion volume and performance status (PS) judged by physicians, as well as subjective symptoms such as pain and QoL of the patients.
Methods
The study was conducted in accordance with the study protocol and the Declaration of Helsinki. The study protocol, amendments, and subject-informed consent were approved by the Osaka National Hospital Institutional Review Boards before initiating the study. In addition, signed informed consent was obtained either from participants (age ≥20), participants and their parent/guardian (20 > age ≥16), or participants' parent/guardian (age <16). Children 7–15 years of age provided written informed assent. The study was registered under UMIN000047330.
Study design
This is a multicenter prospective observational study of patients with VM and KTS.
At the screening period, the demographics, clinical features, and medical history were collected as patient background information. As a primary endpoint, the change in lesion volume from baseline was evaluated by magnetic resonance (MR) imaging. In addition, disease severities, PS, a history of local infection, pain visual analog scale (VAS) score, QoL, and biomarkers (D-dimer, platelet count, and fibrinogen) were obtained at baseline and day 180. The disease severity and PS were examined by the physicians while VAS and QoL were scored by either patients or parents/guardians. The disease severity was assessed as Grades 1–5 for the cosmetic and functional aspects of each part of the body and other clinical aspects (bleeding, infection, skin ulcer, and coagulation abnormalities) according to “Hemangioma and Vascular Malformation Severity Classification” created by the research group supported by the Japanese Ministry of Health, Labor, and Welfare (https://mhlw-grants.niph.go.jp/system/files/2012/123151/201231160A_upload/201231160A0005.pdf).
PS was evaluated by using either Lansky play-performance scale (<17 years old) 11 or Karnofsky performance scale (17 years and older). For QoL, the following questionnaires were used: Pediatric Quality-of-Life Inventory (PedsQL) infant scale (0–24 months),12,13 PedsQL Generic core scale (2–4 years, parent proxy report; 4–24 years, patient report)14–17 and SF-36v2 (26 years and older).18–20
Subjects
Eligible patients were VM and KTS patients with symptoms, such as pain, inflammation (recurrent cellulitis), bleeding and disfigurement, and refractory disease (poor response to or recurrence after standard of care). Eligible patients also had MR images available and had not received any invasive treatment, including sclerotherapy or resection surgery and participated in any clinical trials within 12 weeks at obtaining consent. Once enrolled, MR images of the target lesion were assessed if the lesion volume was measurable. Patients with at least one measurable lesion were formally registered to this study and followed for 6 months.
MR volumetry
All MR studies were performed on a 3.0-T or 1.5-T unit. Axial T1-weighted, fat-saturated (FS) T2-weighted and coronal short tau inversion recover MR images were obtained. The entire lesion volumes were extracted slice by slice from axial FS-T2-weighted MR images by two board-certified radiologists of the Japanese College of Radiology independently using three-dimension volumetric segmentation function in OsiriX MD (Pixmeo, Inc., Switzerland). The average value of the results of them was adopted.
Statistical analyses
The data were summarized by total population and by diagnosis using descriptive statistics. Lesion volumes were log-transformed, and changes in lesion volume between baseline and day 180 were examined by total population and by diagnosis with paired t-tests. Changes in lesion volume stratified by history of infection were also examined. To explore the factors influencing the change in lesion volume, simple regression analyses were performed using the log-transformed change rate as the objective variable and demographics, disease characteristics, and other characteristics as explanatory variables. Multiple regression analysis was also performed using factors with p values smaller than 0.2. The associations between changes in lesion volume and changes in VAS score and fibrinogen were evaluated by correlation coefficients. All p values are two-sided and not adjusted for multiple testing. p-Values of <0.05 are considered to be statistically significant. Statistical analyses were conducted with the use of R software, version 4.1.1.
Results
The study was open to accrual from March 2019 through April 2021 and enrolled 44 patients (Fig. 1). Nine patients (1 VM and 8 KTS) were discontinued before formal registration. Among them, five patients had predominant vascular dilation without mass formation and the MR volumetry could not be performed. Thirty-five patients completed 6 months of follow-up without any invasive treatment. One patient was excluded since her diagnosis was determined neither as VM nor KTS after the completion of the study. All KTS patients registered fulfilled the KTS diagnosis criteria, confirming the exclusion of CLOVES syndrome. Therefore, 34 patients (17 VM and 17 KTS, 1–53 years; median age 15.9 years) were evaluated in this study. Patient demographics and baseline characteristics are listed in Supplementary Table S1 and summarized in Table 1. All KTS patients in this study had lesions in the lower extremities. Thirteen patients (38%) used analgesics, and 22 patients (65%) had a history of sclerotherapy and/or resection surgery.
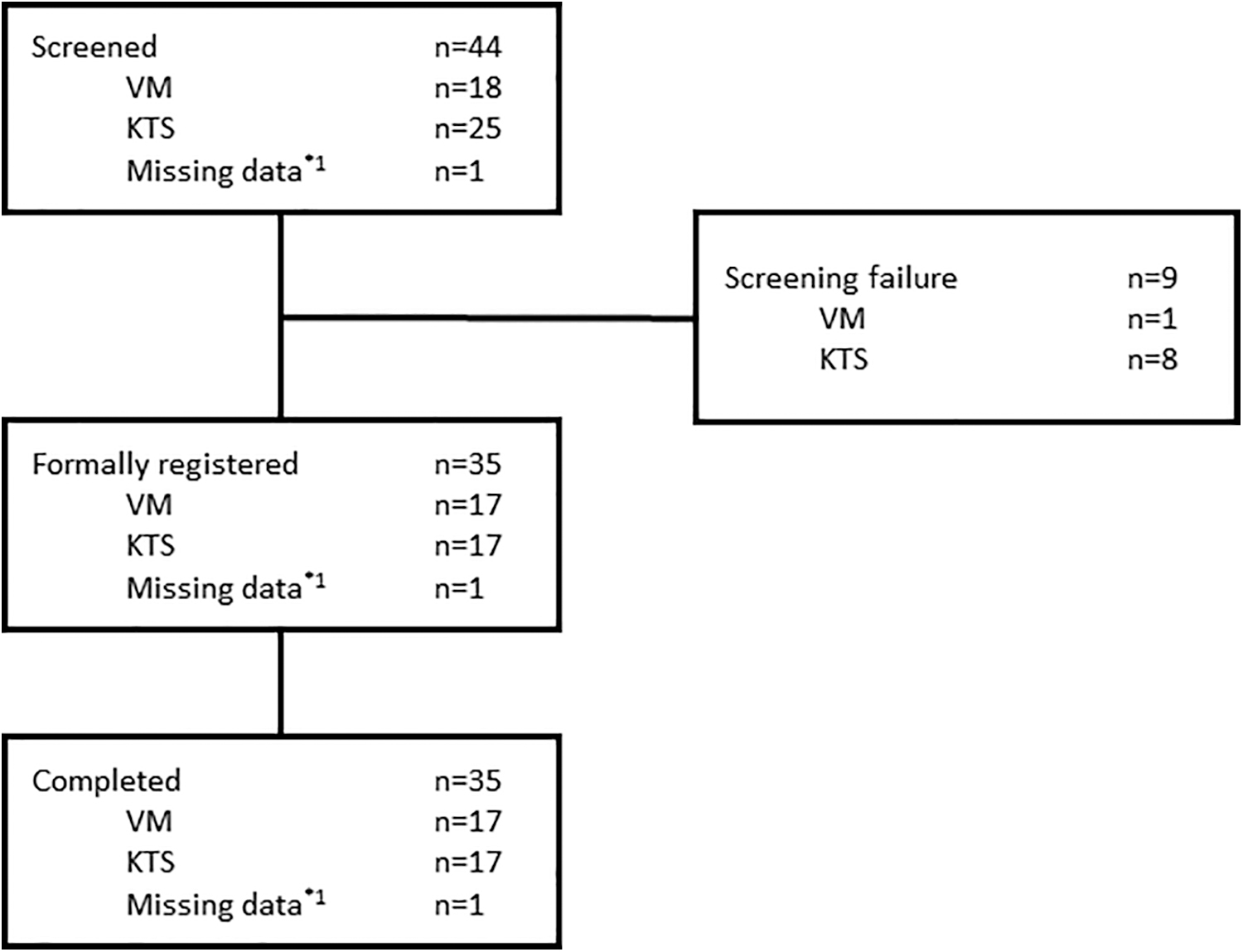
Subject disposition. The subjects who have a measurable lesion were formally registered and followed for 6 months. n is a number of subjects in each category. * 1 Missing data are the case in which VM was selected at the time of obtaining consent, but after the observation period, it was determined that the diagnosis was neither VM nor KTS. The case was removed from the full analysis set. KTS, Klippel–Trenaunay Syndrome; VM, venous malformation.
Patients Demographics and Baseline Characteristics
KTS, Klippel–Trenaunay Syndrome; SD, standard deviation; VM, venous malformation.
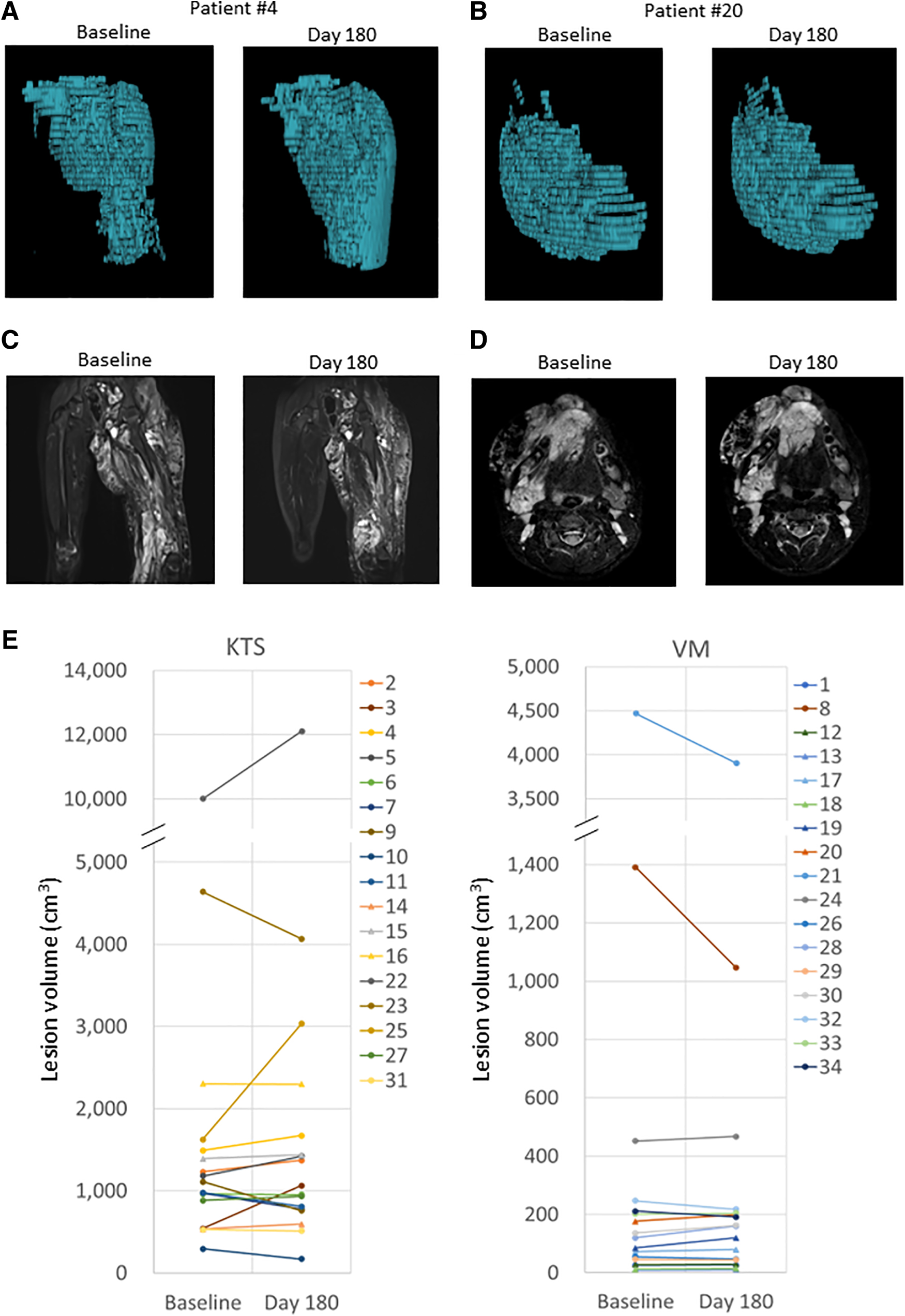
The target lesion volume was measured at baseline and day 180 in each patient (Fig. 2 and Supplementary Table S1). The mean lesion volumes at baseline were 1347.7 cm3 (range 294.8–10,009.1 cm3) and 455.7 cm3 (range, 11.2–4469.3 cm3) in patients with KTS and VM, respectively (Table 2). The mean change rates from baseline at day 180 were 1.08 (KTS), 1.04 (VM), and 1.06 (total), and there were no statistically significant changes between values at baseline and day 180. Simple regression analyses using demographic variables and disease characteristics demonstrated that there were no baseline and disease characteristics significantly affecting the change rate in lesion volume (Table 3). When patients were categorized by a history of infection, there was a statistically significant increase in lesion volume in patients who had infections within 180 days before registration and during the observation period, although the sample size was very small (n = 3) (Table 4).
MR volumetry.
Magnetic Resonance Volumetry
Factors Affecting the Change in Rate in Lesion Volume (Total)
Lesions were divided into those above the waist (right and left head, neck, chest, abdomen, upper arm, forearm, and others [above the waist]) and those below the waist (right and left pelvis, thigh, lower leg, and others [below waist]).
Univariate and multivariate regression analyses were performed with log (change rate) as the objective variable.
Lesion volumes were log-transformed.
FAS, full analysis set; SE, standard error.
Change in Rate in Lesion Volume by a History of Infection
Three patients showed changes in severity (cosmetic), two patients showed improvement by one grade (grade 5–4) and one showed worsening by one grade (grade 3–4). Only one showed a change in severity (function and others), which is worsening in the infection by 2 grades (not applicable to grade 2). The mean values of Lansky play performance scale and Karnofsky performance scale at baseline are 82.5 (range 60–100) and 83.6 (range 60–90), respectively (Table 5). Two KTS patients showed improvement from 70 to 90 and from 60 to 80 and one KTS patient showed worsening from 100 to 90. However, there were no VM patients with any changes in PS over 6 months in this study. Regarding a history of infection, 11 KTS patients (64.7% of KTS) had local infection 180 days before the registration and/or during the observation period. There were no VM patients who had a history of infection in the study. There were no significant changes in the pain VAS score observed between the baseline and day 180. Overall, there were no significant changes in severity, PS, and a history of infection and pain VAS score at day 180 from baseline.
Performance Status, a History of Infection, Pain Visual Analog Scale Score, and Biomarkers
and ** indicate p-values (baseline vs. day 180); *p < 0.05; **p < 0.01.
PS, performance status; VAS, visual analog scale.
On the other hand, when analyzed by diagnosis, patients with VM showed statistically significant improvement in pain VAS score (p = 0.043) and the mean change was −9.2 ± 18 mm. However, there was no correlation between the changes in pain VAS score and the change in rate in lesion volume (Supplementary Table S2).
D-dimer, platelet count, and fibrinogen were also examined as biomarkers (Table 5). Seventeen patients (8 VM and 9 KTS) showed D-dimer with ≧1.0 μg/mL, 17 patients (5 VM and 12 KTS) showed platelet count with <120 × 103, and 5 patients (2 VM and 3 KTS) showed fibrinogen with <150 mg/dL at baseline. KTS patients showed higher D-dimer levels compared with VM patients. There were no statistically significant changes in D-dimer, and platelet count over 6 months within all patients analyzed. Fibrinogen levels exhibited a statistically significant increase in patients with KTS, but not in patients with VM. The mean fibrinogen levels of patients with KTS increased 1.2-fold (p = 0.007) compared with baseline. However, the changes in most cases are within the normal range and there was only one patient whose fibrinogen level showed clinically meaningful improvement. The baseline as well as the change rate in the lesion volume did not exhibit any correlation with those in fibrinogen (Supplementary Table S2).
Twenty-five patients reported with PedsQL Generic Core Scale and eight patients reported with SF-36v2 (Table 6). Because there is only one patient who reported with PedsQL infant scale, the statistical analyses was not conducted with the data. There were no statistically significant changes in total score and subscales of patient report outcome with PedsQL Generic core scales and in each item of SF-36v2 over 6 months. In addition, analysis on the relationships between patients' self-reported QoL scores at baseline and either patients' background or study endpoints at baseline demonstrated that patient-reported QoL total scores were negatively associated to the lesion site at pelvis, the presence of concomitant therapy, the lesion volume, disease severity (cosmetic [trunk/reproductive organ and thigh], function and others [lower leg and foot, thigh, bleeding, infection, and intractable skin ulcer], pain VAS score, and Lansky PS (Supplementary Table S3).
Quality of Life
For PedsQL Generic Core Scale, patients 2–4 years of age used parent proxy-reports, and patients 5–25 years of age used patient self-reports.
Sample size of the total score, physical functioning, emotional functioning, and social functioning.
PedsQL, Pediatric Quality-of-Life Inventory.
Discussion
This study was a multicenter prospective observational study designed to obtain the natural history of intractable VM and KTS, and ultimately to guide clinical study design for novel drug candidates in patients with VM and KTS. Median subject age was 15.9 years, which ranged from 1.1 to 53.2 years, which is comparable with subjects' age of previously reported clinical trials that recruited patients with similar diseases. 6 All measures were collected as scheduled without significant technical challenges, except a few cases outside the allowance.
There were no statistically significant changes between lesion volume at baseline and day 180 (Table 2), and there were no baseline and disease characteristics significantly affecting the change rate in lesion volume (Supplementary Table S1), suggesting that, at least within the 6-month period, significant disease deterioration did not occur regardless of baseline characteristics.
However, there was a significant increase in lesion volume in patients who had infections both within 180 days before formal registration and during the observation period (Table 4). One patient (patient #3) showed 1.96-fold increase in the target lesion. The patient had an infection during 180 days before the registration but did not show a sign of infection during the observation period besides an acute swelling of the hip in the same side as the target lesion. The hip swelling might be caused by intralesional hemorrhage, which potentially affected the target lesion volume. In addition, a resection surgery was performed 9 months before the registration and the observation period overlapped with the time when the postoperative compression was released. This also explains the increase of the target lesion volume in this patient.
On the other hand, there were four patients (11.8%, three KTS and one VM) who showed >20% lesion volume reduction in 6 months' observation period. Among them, two KTS patients (patient #9 and #10) with 31.9% or 41.9% reduction had the episode of cellulitis within a week before taking MR images at the baseline. The other KTS patients (patient #7) who showed 20.3% reduction had cellulitis 2 months before taking MR images at baseline. The VM patients (patient #8) with 24.8% reduction had large lesions (1390.75 cm3 at baseline) and had been using compression stocking, which might affect the lesion volume. In the previous clinical trials for vascular anomalies6,21 and for PROS, >20% lesion volume reduction was used as the efficacy criteria. Therefore, it is important to remove potential causes unrelated to an intervention with the investigational drug candidate, which largely affect the lesion volume such as infection episodes and swelling when designing a clinical trial. For example, if an infection occurs in a patient before the magnetic resonance image scan, the scan should be postponed.
There were no significant changes in severity, PS, a history of infections, and pain VAS score between baseline and day 180, suggesting at least within 6 months that the measures are stable and do not exhibit a significant improvement or worsening. For the pain VAS score, there were seven patients (five VM and two KTS) whose pain VAS score were <5 mm at baseline and six of them maintained the score <5 mm at day 180. Among them, three patients reported no pain (0 mm) both at baseline and day 180, suggesting that not all the patients have pain. When analyzed by diagnosis, there was a statistically significant improvement only in VM patients (−9.2 ± 18.2 mm, mean ± standard deviation), but not in KTS patients. It was reported that ∼13 mm difference on VAS represented the minimum clinically significant change in pain in adults 22 and that 10 mm difference in VAS represented that in children. 23 Therefore, −9.2 mm mean change in pain VAS observed in this study might be marginal. There was no correlation between changes in VAS and change in rate in lesion volume.
In addition, there was also no correlation between pain VAS score and the lesion volume at baseline, suggesting that pain and lesion volume are independent indicators for the diseases.
Since lesions of VM and KTS could cause LIC, the levels of D-dimer, platelet count, and fibrinogen were investigated. Twenty-five patients (74%, 11 VM and 14 KTS) showed at least one abnormal value either with D-dimer, platelet count, or fibrinogen, suggesting indeed many patients showed coagulopathy. There was a statistically significant increase in fibrinogen level between baseline and day 180, but in most cases, the changes are within the normal range and were suggested not to be clinically meaningful. In addition, there was no correlation between those changes and the change in rate in lesion volume (Supplementary Table S2).
Analysis on the relationships between QoL scores and either patients' background or study endpoints suggested the close relationships between QoL and the measures, such as the size of lesion, PS, severity, and pain. The mean total QoL score and scores of all subscales of PedsQL at baselines in this study were higher than those in the Japanese general population. 14 QoL was assessed in a clinical trial evaluating efficacy and safety of sirolimus in patients with complicated vascular anomalies. 6 In the study, improvement of self-report PedsQL by >4.4 or proxy-report PedsQL by >4.5 compared with baseline was defined as partial remission (PR). According to the criteria, 8 patients out of 24 patients (33.3%) who had PedsQL were judged as PR in this natural history study (data not shown). Regular visit to the physicians and assessment of their diseases may itself have positive impact on patients' QoL.
Conclusions
Our results showed the representative natural history of VM and KTS for a 6-month period, in which there was no clinically meaningful improvement or deterioration of the disease status, by evaluation of objective change of lesion volume and other factors. The lesion volume, which was consistently quantified in the study, was largely impacted by local infection of the lesions. The results suggest that evaluation of change in lesion volume can be used as an objective endpoint for a clinical trial and that it is scientifically reasonable to conduct a clinical trial such as Phase 2 proof-of-concept study without a placebo arm, using the results of this study as the control. The future phase 2 study can be designed, having the inclusion and exclusion criteria, and efficacy endpoints that are guided by this study.
Footnotes
Acknowledgments
The authors would like to thank all the patients, their families, radiologists, and other staffs from all the study sites who participated in the study. The authors are grateful to Dr. Shunsuke Yuzuriha from Shinshu University and Dr. Satoru Sasaki from Tonan Hospital for their advice and suggestions.
Authors' Contributions
Conceptualization and methodology: A.F., Kan.K., Tai.N., M.O., T.O., I.S., Kiy.K., A.T., N.U., Kaz.K., F.K., and H.N. Statistical analysis: T.O. and I.S. Investigation: A.F., Tai.N., M.O., S.S., Tad.N., A.H., M.N., A.K., N.A.-H., Kot.I., Kos.I., J.O., and S.H. Writing—original draft: A.F., Kan.K., and H.N. Writing—review and editing: all authors. Supervision: H.N. Project administration: Kan.K., K.N., and F.K. Funding acquisition: Kan.K. and H.N.
Author Disclosure Statement
Kan.K. and A.T. are employees of ARTham Therapeutics, Inc., and H.N. is CEO of ARTham Therapeutics, Inc. Kaz.K. and K.N. are former and current employees of CTD, Inc., and F.K. is CEO of CTD, Inc. A.F., Tai.N., M.O., T.O., N.U., Tad.N., J.O., and S.H. served as paid advisers to ARTham Therapeutics, Inc. A.F. has received honoraria from Nobelpharma Co. Ltd. Kiy.K. is compensated as an officer of Kaken Pharmaceutical Co., Ltd. All other authors declare that no competing financial interests exist.
Funding Information
This research was supported by the Japan Agency for Medical Research and Development (AMED) under grant no. JP18nk0101215 and ARTham Therapetucis Inc.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.