
Abstract
Background:
Secondary lymphedema is acquired and caused by obstruction or injury to a normally developed lymphatic system. Loss of mobility is a common problem in patients with secondary lower limb lymphedema (LLL) following cancer treatment. In this study, we examined the effect of complex decongestive therapy (CDT) on motor function and mobility in patients with LLL.
Methods and Results:
A quasi-experimental study was performed with 24 participants with stage 2 LLL (56.04 ± 14.23 years). Participants received 15 sessions of CDT. Motor function was assessed with a foot tapping test (FTT). Gait speed was measured in single-task (ST) and dual-task (DT) conditions, and DT cost was calculated. All assessments were performed before and after the intervention. The paired t-test and Wilcoxon signed-rank test were used to analyze the effect of CDT on FTT, gait speed, and DT cost. ST and DT gait speed (p = 0.002, p < 0.001) and DT cost (p = 0.001) decreased following the CDT, whereas bilateral FTT scores did not change.
Conclusion:
CDT improves mobility and dual-tasking in LLL, thereby promoting independence in daily life. Future prospective controlled studies are required to corroborate our results.
Introduction
Lymphedema is a chronic progressive condition characterized by protein-rich interstitial fluid retention in the interstitial spaces. 1 Secondary lymphedema develops due to injury or obstruction of the lymphatic system without any anatomical malformation. The development of secondary lymphedema commonly occurs after cancer treatment, especially following surgical procedures, chemotherapy, or radiotherapy. While most studies on cancer-related lymphedema involve breast cancer survivors, lower limb lymphedema (LLL) has been reported in ∼70% of gynecological 2 and 29% of prostate/penile cancer patients. 3 In LLL, disruption of lymphatic drainage can cause protein-rich lymph fluid to accumulate in the lower extremities, leading to swelling. Impaired limb function is one of the most severe symptoms of LLL, limiting patients’ daily life activities and independence.4,5 Patients with LLL tend to avoid physical activity to prevent disease exacerbation. In more severe cases, patients may risk developing a condition called kinesiophobia, “an excessive, irrational and debilitating fear of movement and physical activity resulting from a feeling of vulnerability to painful injuries or reinjuries.” 6 Ultimately, avoiding movement can cause changes in gait parameters and limit physical activity, negatively impacting physical health and social functioning.4,7,8
Complex decongestive therapy (CDT), which consists of manual lymphatic drainage, compression therapy, exercise, and skincare, is recommended as the gold standard in the conservative treatment of lymphedema. 1 One of the advantages of CDT is that it can be performed as an outpatient procedure depending on the patient’s needs and the affected limb’s condition. 9 A systematic review has shown that CDT can be beneficial in reducing the volume of LLL, which in turn improves quality of life. 10 However, the potential implications of CDT for lower extremity motor functioning are still unknown.
In this study, we aimed to evaluate the effect of CDT on lower extremity motor functioning. We hypothesized that 15 sessions of CDT would improve motor functioning and the ability to perform dual-task walking in patients with cancer-related LLL.
Methods
Study design and participants
We used a quasi-experimental pre-/postintervention study design to examine the effect of CDT on mobility and motor function in patients who had cancer-related LLL. Ethical approval was obtained from the Ankara City Hospital Ethics Committee (E2-23-3812). The study was conducted between April 2023 and September 2023 at the Lymphedema Clinic and Sports Rehabilitation Laboratory at the Ankara City Hospital. According to the International Lymphedema Association guideline, stage 2 lymphedema is characterized by persistent pitting edema that does not subside with elevation, and the severity of the condition is classified as moderate with a 20%–40% increase in limb volume. Thirty patients who developed stage 2 LLL after cancer-related surgery participated in the study. A physical therapy and rehabilitation physician determined the lymphedema diagnosis and stage. Participants were informed about the study and signed written informed consent before their inclusion in the study. They were allowed to withdraw from the study without reporting a reason. The inclusion criteria were: (i) having stage 2, secondary lymphedema according to the International Lymphedema Association Guideline, 11 and (ii) primary cancer therapies (e.g., surgery, chemotherapy, and radiotherapy) have been completed at least 6 months ago. The exclusion criteria were: (i) primary lymphedema, (ii) having severe systemic (e.g., diabetes mellitus, active cancer) or neurological disease, (iii) radiotherapy burn, skin infection, and ulcers in the affected limb, (iv) sensorial problems, and (v) previously received CDT treatment. The participant flowchart is presented in Figure 1.
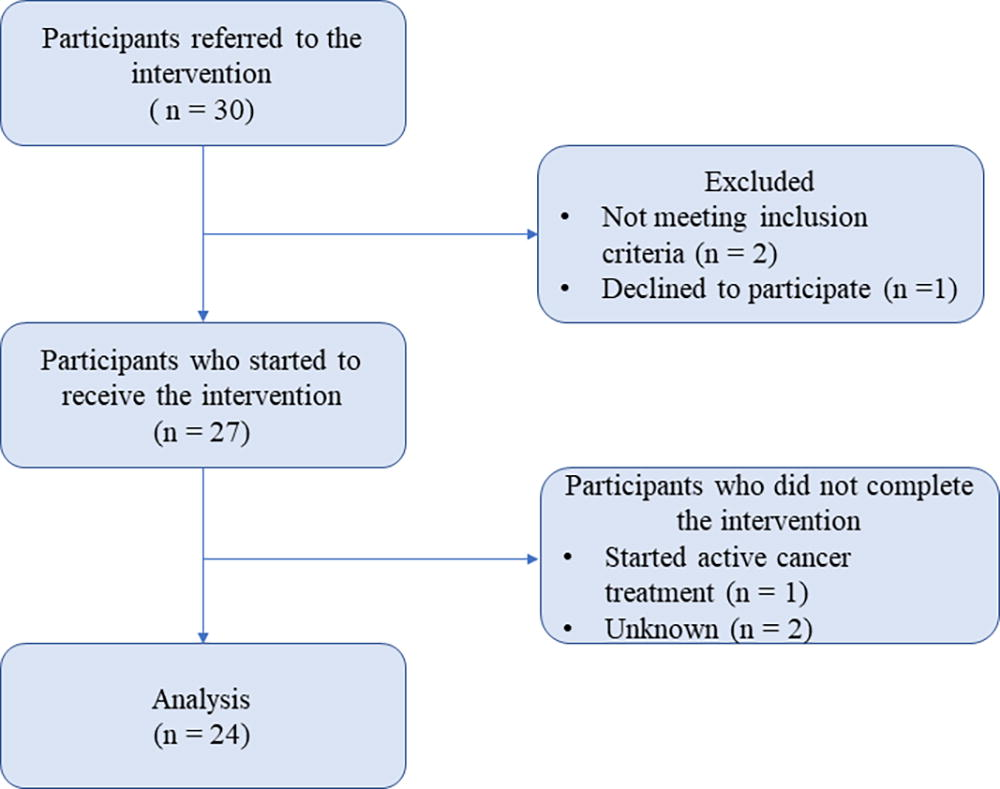
Participant flowchart.
Intervention protocol
After the initial evaluation of the patients, CDT was performed by a certified physiotherapist trained in this field. The CDT consisted of manual lymphatic drainage, compression bandage, exercises, and skincare. Patients received treatment 5 days a week for 3 weeks (15 sessions). In each session, the patients underwent multilayered bandaging and kept the bandages on for 21–24 hours a day. Therapeutic exercises, such as ankle pumps, foot circles, leg slides, knee lifts, and side leg raises, were performed with the bandages for two sets of 10 repetitions each to improve lymphatic drainage through muscle contractions and relaxations. Patients were also encouraged to engage in gentle daily walking. Additionally, the rehabilitation program included abdominal breathing exercises, with 5–10 repetitions per session, administered two to five times daily based on the patient’s tolerance. Patients were informed about skincare, hygiene, and protection of their lymphedematous extremities from cold/heat and trauma. Skincare involved applying vitamin E cream to the affected lower limb both before and after the bandage was removed.
Measurements
Participants filled out a demographic questionnaire recording their age, sex, body weight (in kg), length (in cm), and educational status. Before the intervention, we conducted a comprehensive assessment encompassing various aspects of the patient’s health information, such as hypertension, diabetes, cardiac problems, circulatory problems, and thyroid dysfunction. We further collected information regarding previous treatments related to cancer, including chemotherapy, radiotherapy, and hormone therapy. We recorded the lymphedema history, including the date of onset, cause of onset, where edema first started, and whether they had received any previous treatment for lymphedema. Foot preference and physical activity level were assessed by the Foot Preference Test and International Physical Activity Questionnaire–short form, respectively. We evaluated lower limb motor function using the foot tapping test and assessed the gait speed with the 3-m Timed Up and Go Test in single- and dual-task conditions.
Foot preference
We used the Foot Preference Test to ascertain foot preference. 12 The task requires standing on a single foot while performing nine specific movements using the other foot. These movements include stepping from a starting point toward the researcher, hitting a tennis ball without looking for a target, stepping on a tennis ball, drawing a large letter “A” on the floor, stepping on a stool, climbing stairs, climbing stairs backward, hitting a tennis ball toward a target, and erasing the letter “A” from the floor. The test is conducted twice in the same order. Foot preference is determined by assigning “0” points for each right foot use and “1” points for each left foot use, with a possible score range of 0–18 points.
Physical activity level
Physical activity level was assessed using the International Physical Activity Questionnaire–short form. 13 The 7-item scale is used to determine the time spent by the individual on sitting, walking, moderate, and vigorous physical activity. The time and day values obtained from the scale are multiplied by the metabolic equivalent (MET) value determined for each item and added to the total physical activity time. Physical activity level is classified as physically inactive (<600 MET-min/week), low physical activity level (600–3000 MET-min/week), and adequate physical activity level (>3000 MET-min/week).
Foot tapping test
Foot tapping score was recorded by a computerized test. 14 Participants sat on a comfortable chair and found the most comfortable foot position. They were asked to press a pedal as fast as possible for a duration of 10 seconds. The test was conducted three times on both the right and left foot. An average score was calculated separately for each foot.
Gait speed
Gait speed was assessed by the Timed Up and Go Test 15 in single- and dual-task conditions. Participants were asked to perform two tasks while walking along a 3-m walkway that is marked with a 30.48 cm width, wearing their standard footwear. The first task was to stand up and walk along the 3-m walkway, turn around, walk back at a self-selected speed, and sit down on the chair (single task [ST]). The second task was to count backward by five, starting with a randomly selected number between 70 and 100 while walking the same walkway at a self-selected speed (motor + cognitive task). During the dual-tasking session, participants were instructed not to prioritize one task over the other. Gait speed for each task was recorded using a mobile phone (Apple iPhone 11—iOS 16.1.1) and a built-in stopwatch application that is accurate up to 0.01 seconds. Dual-task cost (DTC) was calculated to measure dual-task interference using the following equation: DTC (%) = 100*(DT − ST)/ST. A higher DTC score indicates lower multitasking ability. 16
Statistical analysis
Before the experiment, the sample size was estimated using G*Power (version 3.1.9.7). 17 With a medium effect size, a significance level of ≤0.05, and an 80% power confidence interval, the total sample size required was 27. A paired sample t-test and Wilcoxon signed-rank test were conducted to compare the outcome scores before and after the intervention. All statistical analyses were performed using SPSS for Macintosh (version 25.0, Chicago, IL, USA). The significance level was set at p < 0.05.
Results/Findings
Of the 30 initially included patients, 27 met the eligibility criteria. Twenty-four patients completed the intervention, while three of them dropped out due to irregular attendance. Patient characteristics are summarized in Table 1.
Demographic and Clinical Characteristics of Patients
Descriptive statistics are presented as the number of people (%) and mean ± SD.
BMI, body mass index; MET, metabolic equivalent; SD, standard deviation.
After 15 sessions of CDT, there was no significant change in the foot tapping score (right foot, p = 0.74; left foot, p = 0.48). However, DTC decreased (Z = −3.200, p = 0.001), and gait speed improved significantly for both ST (Z = −3.029, p = 0.002) and DT (Z = −4.086, p < 0.001). Table 2 summarizes the statistical results.
Baseline and Postintervention Outcomes
Normally distributed data are presented as mean (SD), non-normally distributed data are presented as median (interquartile range). ST and DT are presented as gait speed in seconds. FTT is presented as the number of tapping per second.
Non-normally distributed data.
p < 0.05.
CDT, complex decongestive therapy; DT, dual-task; FTT, finger tapping test; n, number; ST, single task.
Discussion
The present study provided evidence that CDT improves gait speed and dual-tasking in patients with cancer-related LLL.
It has been reported that antalgic gait is a common problem in patients with LLL due to the unequal size of the limbs. 18 To compensate for the center of gravity, patients shorten the swing phase and demonstrate excessive leg adduction, ankle plantar flexion, and external hip rotation, 6 which may lead to degenerative joint changes. Forner-Cordero et al. 19 reported that gait speed was slower in patients with severe bilateral LLL than in those with unilateral LLL. Although it is clearly seen that gait is impaired in LLL, yet there appears to be a need for more literature examining its effect on gait parameters. To date, no study has investigated the effect of CDT on gait speed in patients with LLL. This study assessed the gait speed in ST and DT conditions in patients with stage 2 LLL. We demonstrated that CDT improved gait speed in both ST and DT conditions. Gait speed is a critical index of physical function in midlife. 20 Previous research has established a significant correlation between slower gait speed and diminished capacity to carry out daily activities, with walking speed emerging as the foremost physical performance metric in predicting the initiation of functional dependence.21,22 Relatedly, the American Cancer Society recommends that patients avoid inactivity and participate in regular physical activity as soon as possible after diagnosis and treatment. 23 Moreover, it has been reported that cancer survivors with slower gait speed have a higher risk of death. 24 Considering that walking as a simple form of exercise may be more easily accepted by patients, improving the gait speed of cancer survivors with LLL is crucial to help them achieve better mobility and an overall improved quality of life. Relatedly, as either single- or dual-task gait speed is a crucial predictor of fall risk,25,26 the use of CDT interventions represents a promising approach to fall prevention in cancer survivors with LLL. Future studies utilizing more precise methods analyzing other gait parameters, such as step length/width and cadence, may provide more inclusive data regarding the effects of CDT on gait in patients with LLL.
Dual-task walking, such as talking while walking or carrying a shopping bag, is a necessary part of daily life. During dual-tasking, cognitive-motor interference can impair either or both cognitive and motor task performance due to limited cognitive resources. 27 As we presented in this study, the effects of cognitive-motor interference on walking performance are frequently quantified by the DT cost. In this study, we demonstrated that CDT decreased cognitive-motor interference in patients with LLL. Considering the importance of dual-task in daily life activities, it is fair to state that CDT holds significant potential for improving patients’ ability to carry out independent daily living by reducing DTCs.
Cancer survivors have been reported to experience a decline in working memory. 28 During our study, we used a counting backward task as an additional cognitive task while walking but did not test it separately. Since counting backward is a working memory task, 29 one possible explanation for the decreased DTC may be an improvement in this working memory function. Further, it is reasonable to assume that CDT may have improved the overall mood and cognitive ability of patients by reducing lymphedema and increasing social interaction during the treatment period. Future research analyzing cognitive function separately would provide evidence of whether cognitive enhancement improves dual-task performance.
We did not find a significant change in foot tapping score following CDT. During the foot tapping task, patients are required to perform repetitive dorsiflexion of the ankle. However, the patients who participated in our study had a long history of lymphedema, which could have led to a limitation of movement in the ankle joint. This ankle range of limitation could be a possible explanation for the lack of improvement in tapping score after CDT. Future studies can consider analyzing ankle mobility before and after the intervention while controlling for this factor.
There are several limitations of this study that should be noted. First, we were unable to form a control group as our patients needed immediate treatment. Second, our sample size was below the number indicated by the power analysis. Third, we did not include limb volume measurement in our analysis. Last, we did not conduct a follow-up to evaluate the long-term effects of CDT on foot tapping score and dual-task walking. Future research needs to be conducted with a control group to validate our results, including limb volume measurement and follow-up outcomes in a larger sample size.
Implications on Physiotherapy Practice
CDT improves gait speed in both single- and dual-task conditions.
Given the crucial role of gait speed in daily activities, the use of CDT can significantly improve the quality of life and mobility of patients with LLL.
Therefore, it is important to adopt a conservative therapeutic approach for managing lymphedema that emphasizes the importance of CDT.
Footnotes
Acknowledgment
The authors thank Fikret Arı for designing the foot-tapping device.
Authors’ Contributions
E.G. designed the study. Ü.D.Ö. performed the intervention. E.G. and N.G. carried out the analysis, interpreted results, and wrote the first draft of the article. All authors read and approved the final article.
Author Disclosure Statement
The authors have no conflicts of interest to declare.
Funding Information
The authors did not receive support from any organization for this study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.