
Abstract
Antimicrobial resistance of Streptococcus pneumoniae in France is closely monitored by the pneumococcus surveillance network, founded in 1995, which collects data from regional observatories (Observatoire Régionaux du Pneumocoque [ORP]). In 2007, 23 ORPs analyzed the antibiotic susceptibility of 5,302 isolates of S. pneumoniae recovered in France from cerebrospinal fluid, blood, middle ear fluid, and pleural fluid, as well as from adult respiratory samples. The study showed that 38.2% of the strains were nonsusceptible to penicillin, 19.3% nonsusceptible to amoxicillin, and 10.5% nonsusceptible to cefotaxime. The percentage of pneumococcus nonsusceptible to penicillin varied according to both the sample and the age of the patient (child/adult): blood (27.8%/32.5%), cerebrospinal fluid (33.7%/34.6%), middle ear fluid (60.2%/27.5%), and pleural fluid (50.0%/31.0%). Between 2003 and 2007, the frequency of penicillin resistance in invasive pneumococcal disease gradually decreased from 46.4% to 29.0% in children and from 43.8% to 32.7% in adults. This decrease coincided with the introduction of a seven-valent pneumococcal conjugate vaccine into immunization programs and with a general reduction in levels of antibiotic consumption in France.
Introduction
Streptococcus pneumoniae is the most commonly identified bacterial cause of community-acquired pneumonia, meningitis, and otitis media. It is also a frequent cause of bacteremia, and accounts for significant morbidity and mortality. The highest incidence of pneumococcal disease is observed in children <2 and in adults >65 years of age. 20 This pathogen, which is naturally susceptible to antibiotics, developed resistance partly due to a high antibiotic consumption. 12 Since 1979, a steady increase in the percentage of pneumococcus nonsusceptible to penicillin (PNSP) strains was observed in France, reaching 55.4% in 2001 with a particularly high frequency in children (about 71%). 24 France was one of the European countries with the highest frequency of PNSP and erythromycin-resistant isolates. 8 Since then, a national campaign for reducing the use of antibiotic was launched in 2002, and the seven-valent pneumococcal conjugate vaccine (7-PCV) was introduced in January 2003 for immunization of infants under 2 years of age. 7-PCV sales increased from 0.6 to 1.6 doses per child under 2 years between 2003 and 2006. Coverage with three doses of PCV was estimated in three specific surveys at 27% in 6-month-old children in 2004, 5 at 44% in 6–12-month-old children in 2006, and at 56% in 6–12-month-old children in 2007. 11 Despite a decrease in the percentage of PNSP since 2003 (50.2%), 18 the frequency of antibiotic resistance is still very high and warrants monitoring. We analyzed the data collected in 2007 from the ongoing surveillance of pneumococcus susceptibility and analyzed recent trends in susceptibility.
Materials and Methods
French pneumococcus surveillance
The French pneumococcus surveillance network, composed of 23 regional pneumococcal observatories called “Observatoires Régionaux du Pneumocoque (ORP)” and created in 1995, includes 396 laboratories, of which 296 (74.7%) are public hospital laboratories and 100 (25.3%) are private laboratories. It has been estimated that this network covers, on average, 63% of the French population. 22 It has carried out biannual national surveys since 1995, permitting the collection of >5,000 pneumococcus strains each time.
Data and strain collection
The study was conducted from January to December 2007. Each participating laboratory sent S. pneumoniae isolates with demographic and clinical information, as well as the results of antibiotic susceptibility tests to one of the 23 regional coordination laboratories.
All pneumococcal strains isolated from cerebrospinal fluid (CSF), blood, middle ear fluid, and pleural fluid from children (<16 years of age) and adults were sent. In addition, each month, the ORPs included the two first respiratory isolates from adults recovered in their laboratory. When S. pneumoniae was recovered from different samples in the same patient, only one sample was included. The priority was as follows: CSF, blood, pleural fluid, and middle ear fluid.
Antibiotic susceptibility testing
Each laboratory determined the minimum inhibitory concentration (MIC) of penicillin G (PEN), amoxicillin (AMX), and cefotaxime (CTX) using E-test® strips (AES, Combourg, France), the VITEK2® system, or the ATB-Pneumo® kit (BioMérieux, Marcy l'Etoile, France). The susceptibility to erythromycin (ERY), cotrimoxazole (SXT), rifampicin (RA), pristinamycine (PRI), and norfloxacin (NOR) was also determined using a disc diffusion test and/or the VITEK2® or ATB-Pneumo® kit systems. All isolates were sent to the regional coordination center for determination of MIC for PEN, AMX, and CTX, by the agar dilution method performed in Mueller–Hinton agar supplemented with 5% horse blood. Three quality control strains (R6 [WT], ATCC49619, and CNRP32475) provided by the French National Reference Centre for Pneumococci (CNRP) were included. Susceptibility tests results were interpreted according to the 2007 French guidelines of the Comité de l'Antibiogramme de la Société Française de Microbiologie (CA-SFM). 19 The breakpoints were 0.06–1 mg/L for PEN, and 0.5–2 mg/L for AMX and CTX. PNSP were defined as strains with an MIC for PEN of over 0.06 mg/L. Data were also interpreted using CLSI criteria with new MIC breakpoints for patients without meningitis who are treated with intravenous penicillin. 4 In this case, susceptible, intermediate, and resistant MIC breakpoints for PEN were ≤2, 4, and ≥8 mg/L, respectively.
Statistical analysis
Data were monitored and validated using Capture System software. SAS (version 9.1.3., SAS Institute, Cary, NC) was used for statistical analysis using the χ2-test for trends; a p-value of <0.05 was considered significant.
Results
The 23 regional pneumococcal observatories studied 5,302 strains over the course of the study period. Of these, 1,477 (27.9%) were isolated from children and 3,825 (72.1%) from adults. These strains were recovered from various samples: 387 CSF (children [C], 95; adults [A], 292); 3,308 blood (C, 370; A, 2,938); 135 pleural fluid (C, 38; A, 97); 1,043 middle ear fluid (C, 974; A, 69); and 429 respiratory samples (A). Most of the strains were isolated from blood samples for adults (77%) and from middle ear fluid for children (66%). Strains were isolated more frequently in winter (1,193 strains [37.6%]) than in summer (559 strains [10.5%]; p < 0.01).
The frequency of reduced susceptibility [intermediate+resistant (I+R)] to PEN, AMX, and CTX based on samples isolated from children and adults is shown Table 1. We tested 5,302 strains, and 38.2% (2,027 strains) were found to be PNSP: 31.7% of these (1,677 strains) showed intermediate and 6.6% (350 strains) were resistant (MIC > 1 mg/L). The highest frequency of PNSP was observed in pediatric isolates from ear samples (60.2%). Concerning the other β-lactams tested, 19.3% of the strains (1,022 strains) were nonsusceptible to AMX and 10.5% (557 strains) were nonsusceptible to CTX. The frequency of resistance was 0.8% (42 strains) and 0.2% (10 strains), respectively, for AMX and CTX. The frequency of nonsusceptible isolates to other antibiotics was 40% for ERY, 25.8% for SXT, 6.4% for NOR, 0.9% for PRI, and 0.3% for RA.
Susceptibility of 5,302 Streptococcus pneumoniae Isolates to Penicillin G, Amoxicillin, and Cefotaxime Determined by the Agar Dilution Method
Strains were isolated from adults and children in 2007.
CSF, cerebrospinal fluid.
In children, the frequency of PNSP was 50.2% (741 strains), with a maximum frequency for children between 1 and 2 years (63%). Resistance to PEN was found in 114 of the 741 PNSP strains (7.7% of the strains isolated from the children tested). The percentage of intermediate and resistant strains was 23.3% and 0.7% for AMX, and 13.1% and 0.2% for CTX, respectively. The frequency of resistance varied depending on the sample and was often higher in middle ear fluid. Thus, PNSP represented 60.2% of middle ear fluid isolates (n = 974) of which 8.6% were resistant strains. There were 29.3% and 16.1% strains with reduced susceptibility (I+R) to AMX and CTX, respectively, but the proportion of resistant strains remained low, 0.9% for AMX and 0.2% for CTX. In addition, 59.5% of the strains were nonsusceptible (I+R) to ERY. The frequency of decreased susceptibility (I+R) to PEN, AMX, and CTX in CSF samples was 33.7%, 16.9%, and 10.5%, respectively. The frequency of penicillin resistance (MIC >1 mg/L) was 4.4%, and only one strain was resistant to AMX and none to CTX. Regarding blood samples (n = 370), 103 strains (27.8%) were PNSP. Resistance to PEN was found in 20 of these strains (5.4% of PNSP strains). The number of strains showing intermediate resistance was lower for AMX and CTX, 11.9% and 6.2%, respectively, and resistance remained rare (0.3% for both antibiotics). Finally, in pleural fluid (n = 38), the percentage of pneumococcus isolates with reduced susceptibility to PEN, AMX, and CTX was 50%, 21.1%, and 13.2%, respectively. Six of these isolates were resistant to PEN, but no isolate was resistant to AMX or CTX.
In adults, the overall percentage of PNSP was 33.7% (1,286 strains). Resistance to PEN was found in 236 of these strains (6.2% of all strains isolated from adults tested). A maximum frequency of PNSP was observed in elderly patients (90 years and over; 46.4%). The percentage of intermediate and resistant strains was 16.6% and 0.8% for AMX and 9.3% and 0.2% for CTX, respectively. Among the strains isolated from CSF (n = 292), 34.6% were PNSP and nearly 4.8% of all strains were resistant to PEN. A decrease in susceptibility to AMX and CTX was observed in 14.7% and 7.9% of strains, respectively. Three strains were resistant to AMX and one strain was resistant to CTX (MIC = 4 mg/L). Concerning blood samples (n = 2,938), the percentage of PNSP was 32.5%, and 5.9% were resistant. Regarding AMX and CTX, 16.7% and 9.1% of strains, respectively, were categorized as intermediary, but the proportion of resistant strains remained low, 0.7% and 0.2%, respectively. Finally, of the 429 respiratory samples, the percentage with reduced susceptibility to PEN, AMX, and CTX was 42.2%, 21.7%, and 11.1%, respectively. Thirty-seven strains were resistant to PEN, 7 to AMX, and 1 strain to CTX (Table 1).
No resistance marker was present in 2,421 (45.7%) of the strains studied, whereas 1,801 strains (34%) had one or two resistance markers. The most common resistance phenotypes are presented in Table 2. The loss of activity of AMX, CTX, ERY, and SXT was similar to that observed for penicillin. No pneumococcus susceptible to penicillin (PSP) strain had reduced susceptibility to AMX or CTX, whereas 1,021 of the 2,027 (50.4%) strains not susceptible to PEN had reduced AMX susceptibility and 558 (27.5%) of these strains also had reduced CTX susceptibility. The most frequent nonsusceptibility (I+R) encountered in PNSP was that to ERY (742 strains). ERY resistance was more common in PNSP strains (84.2%) than in PSP strains (12.7%). Moreover, 48.9% of PNSP and only 11.5% of PSP were not susceptible to SXT. Multidrug resistance, defined for S. pneumoniae as resistance to at least three families of antibiotics, 7 was observed in almost 11% of all strains tested. The majority of multiresistant strains had both decreased susceptibility to β-lactams and macrolide resistance.
Multiresistance and Most Common Resistance Phenotypes of 5,302 Streptococcus pneumoniae Strains for Six Antibiotics
The strains were isolated from children and adults in France in 2007.
P, penicillin G; ERY, erythromycin; SXT, cotrimoxazole; PRI, pristinamycin; RA, rifampicin; NOR, norfloxacin.
Compared frequencies of reduced antibiotic susceptibility of S. pneumoniae strains isolated from patients with invasive pneumococcal disease (CSF and blood culture) in France in 2003, 2005, and 2007 are shown in Fig. 1. The frequency of PNSP decreased from 44.1% in 2003 to 32.2% in 2007 (p < 0.001)3,16,18 and that of penicillin-resistant pneumococci (MIC >1 mg/L) decreased from 12.3% in 2003 to 6.6% in 2007 (p < 0.001). Changes in the susceptibility of strains recovered from children (<16 years old) accounted for most of this decrease. Indeed, the frequency of PNSP isolated from CSF fell from 47.5% (2003) to 33.7% (2007) (p < 0.02) and those isolated from blood from 46.1% (2003) to 27.8% (2007) (p < 0.001). 16 The frequency of PNSP in adults also fell from 43.8% to 32.7% (p < 0.001). Further, a gradual decrease in resistance (I+R) to the other antibiotics tested was observed from 2003 to 2007: AMX, 27.3% to 16.6%; CTX, 15.8% to 8.9%; ERY, 47.4% to 34.5%; SXT, 33% to 23.7% (p < 0.01). In addition, a decrease in the frequency of PNSP isolated from middle ear fluid was observed in children between 2003 (69.2%) and 2007 (60.2%) (p < 0.02).
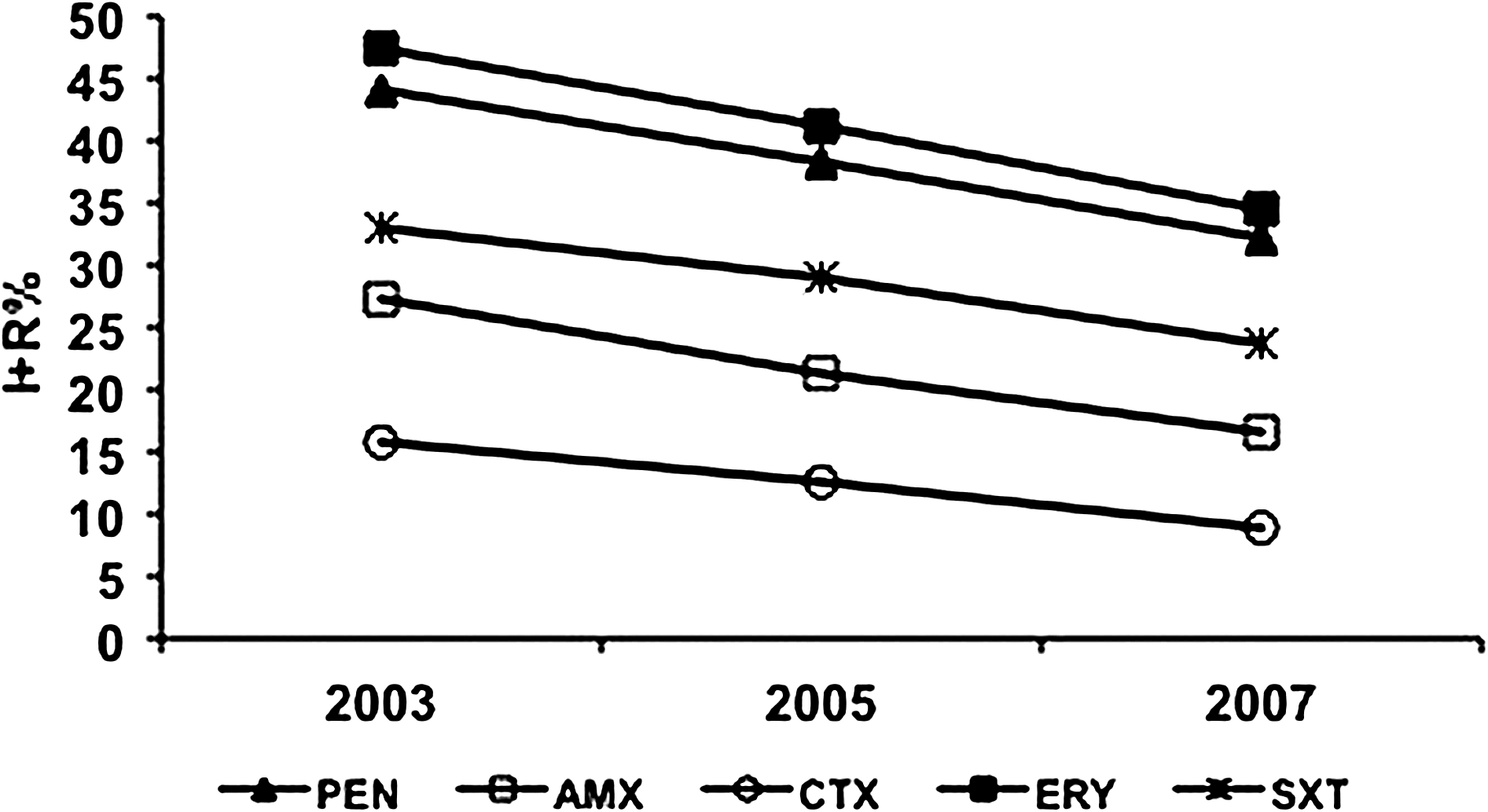
Trends in susceptibility to five antibiotics of invasive pneumococcal isolates (cerebrospinal fluids and blood cultures) in France from 2003 to 2007. PEN, penicillin G; AMX, amoxicillin; CTX, cefotaxime; ERY, erythromycin; SXT, cotrimoxazole.
Nevertheless, some regional discrepancies in PNSP frequency were observed. Thus, the percentage of PNSP varied depending on the region, ranging from 29% in Alsace to 50% in the west of the Paris Region of Ile de France. A frequency of PNSP higher than 40% was observed in only six ORP in 2007, whereas it was 17 in 2005. This decrease was observed in both children and adults.
Moreover, new MIC breakpoints were proposed by CLSI in 2008 for patients without meningitis who are treated with intravenous penicillin. 4 On the basis of these criteria for bacteremia in our study, the proportion of PNSP was 0.8% with 0.05% penicillin resistant and 0.75% intermediate isolates.
Discussion
Although the incidence of pneumococcal resistance to antibiotics is decreasing, France remains one of the European countries with the highest levels of PNSP in 2007. Twenty-nine countries reported results for surveillance of invasive pneumococcal infections (blood and CSF: n = 11,585) in 2007. 8 In Norway and The Netherlands, the frequency of PNSP remained low, close to 2%. In other countries, however, the rate of PNSP was increasing, for example, in Finland (2005, 6.9%; 2007, 13.2%), Italy (2005, 9.1%; 2007, 14.8%), Slovenia (2005, 10.6%; 2007, 16.9%), and Ireland (2005, 11.1%; 2007, 17.5%). As in France, the percentage of PNSP decreased in Luxembourg (2005, 11.6%; 2007, 6.5%) and Germany (2005, 4.2%; 2007, 2.8%). Similar trends were observed in the United States, where a national study showed a decrease from 26.3% in 2001 to 16.5% in 2004. 15 In Spain, a significant decrease in PNSP was observed between the periods 1993 and 1997, 2001 and 2003, and 2004 and 2007 with, respectively, 38.8%, 32.3%, and 24.7% of PNSP. 10
No emergence of AMX-resistant strains (2003, 1.8%; 2005, 1.8%; 2007, 0.8%) and CTX (2003, 0.2%; 2005, 0.2%; 2007, 0.2%) was observed in France unlike in the United States.3,25 Regarding other antibiotics, we noted a decrease in frequency of resistance (I+R) to ERY (2005, 46%; 2007, 40%) and SXT (2005, 30.5%; 2007, 25.8%). These results appeared to be related to the decrease in PNSP.
These evolutions occurred following national programs developed by the French public health authorities. Indeed, in 2002, the French National Insurance Fund for Salaried Workers (CNAMTS) initiated an extensive program to avoid inappropriate antibiotic use by outpatients. The “Antibiotics are not automatic!” campaign aimed at increasing awareness of the French to good antibiotic practice. 13 A previous study conducted in 2000 in three regions of France demonstrated that intensive educational strategies aimed at optimizing antibiotic use could significantly reduce the frequency of PNSP colonization.14,23 Moreover, since 2002, the CNAMTS has promoted the use of a rapid antigen detection test for streptococcal pharyngitis, and distributed it to physicians free of charge to decrease unnecessary antibiotic prescription. The overall community antimicrobial consumption in France has decreased from 33.0 defined daily doses per 1,000 inhabitants per day in 2001 to 27.9 in 2006, that is, a reduction of 15%; the consumption of broad-spectrum penicillins has decreased by 20% and the consumption of macrolides by 39%.2,9 Studies performed in other European countries described a similar reduction in penicillin resistance levels due to reduced general antibiotic use in the community.1,21 In addition to reduced consumption of antibiotics, the introduction of the 7-PCV in March 2002 was associated with a 71% decrease in vaccine-type invasive pneumococcal disease incidence between 2001/2002 and 2006 in children under 2 years of age, 17 which may have contributed to large decrease in PNSP frequency in children under the age of 2 years of age.5,6,17 Nevertheless, it is premature to assess the real impact of vaccination on the decrease in resistance in France.
In conclusion, the frequency of PNSP has decreased in France since the implementation of the new antibiotic policy launched in 2002 as well as the introduction of the 7-PCV. This gradual decrease was observed both in children and adults. The frequency of penicillin resistance for invasive pneumococcal disease fell from 46.4% to 29.0% in children and from 43.8% to 32.7% in adults, between 2003 and 2007. Despite a decrease in the frequency of PNSP, continued surveillance of antimicrobial activity is essential to track changing resistance at the regional and national level.
Footnotes
Acknowledgments
The authors thank the French regional pneumococcal observatories and the participating laboratories for their assistance. This study was funded by an educational grant from GlaxoSmithKline (Dr. Ammar Zerrar).
Disclosure Statement
The authors received an educational grant from GlaxoSmithKline. There was no conflict of interest regarding the content of this article.
This work was presented in part at the ICAAC congress in 2008 (poster no. C2-258).