
Abstract
Knowledge about pneumococcal carriage, antibacterial resistance, serotype prevalence, and prevalence of invasive pneumococcal disease (IPD) after introduction of pneumococcal conjugate vaccines (PCVs) is lacking in the Faroe Islands. PCV-7 was introduced in 2008 and PCV-13 in 2010. The aim was to obtain knowledge on serotypes and antimicrobial resistance in pneumococci from carriage in children attending day-care centers (DCCs) and invasive isolates. Nasopharyngeal swabs were collected from 607 healthy children attending DCCs in the Faroe Islands in January to March in 2009, 2010, and 2011. Pneumococci were cultured selectively, tested for antibacterial susceptibility, and serotyped. Data from IPD isolates from 1974 to 2016 from the Department of Microbiology, National Hospital of the Faroe Islands, and typed and stored at Staten Serum Institute were also analyzed. Of the 607 screened children, 45% were pneumococcal carriers, 50% in 2009, 40% in 2010, and 42% in 2011. Antibiotic resistance in pneumococci was rare both in carriers and patients. Five penicillin nonsusceptible pneumococci were found in carriers (1.8%) and one among the invasive isolates (1.7%). The most common serotypes in carriage were 6B and 6A in 2009, serotype 3 and 6C in 2010, and serotype 11 and 6C in 2011. Serotype 6B was not found in 2011. The most common serotypes among IPD were 7F and 3. Pneumococcal carriage prevalence in healthy children attending DCCs in the Faroe Islands was low and antibacterial resistance was rare, compared with Iceland. The results suggest a possible serotype shift, reduction in antibacterial use, and PCV-7/13 serotype decrease in IPD after the introduction of pneumococcal vaccinations in children.
Introduction
S
Day-care centers (DCCs) provide a favorable milieu for pneumococcal spread, where children with an immature immune system and poor hygiene practices are crowded together. 4 Therefore, children attending DCCs are more likely to be pneumococcal carriers than children not attending DCCs.5–7 Common infections such as respiratory tract infections are frequent causes for prescribing antibiotics and thus contribute to a high consumption of antibiotics in the community. 8 Several studies have shown an association between high antimicrobial use and increasing antimicrobial resistance in pneumococci.9–11 Penicillin has been the drug of choice for treatment of pneumococcal infections in Scandinavian countries for decades. In the mid-1960s, the first strain of penicillin nonsusceptible pneumococci (PNSP) was reported 12 and during the last decades, antimicrobial resistance of pneumococci has increased in many countries, including Iceland.13,14
Knowledge about carriage rates, antibacterial resistance, and serotype prevalence after introduction of pneumococcal conjugate vaccines (PCVs) is lacking in the Faroe Islands. Pneumococcal vaccination was introduced with the 7-valent vaccine in 2008 and the 13-valent vaccine in 2010. The Faroe Islands are relatively isolated small populated islands and suitable for carriage, antibacterial resistance, and pneumococcal serotype studies. Iceland is a neighboring Nordic country with cultural similarities. In Iceland, there have been several studies on pneumococcal carriage, resistance, and serotype prevalence before and after the introduction of PCVs.
The objective of this Faroe Islands study were to describe pneumococcal carriage in healthy children aged 0 to 7 years from 2009 to 2011, to describe antibacterial resistance and serotype prevalence in these carriage isolates and invasive pneumococcal disease (IPD) isolates from 1974 to 2016, and to compare the results with similar studies from Iceland.
Materials and Methods
Study population
In 2009, 2010, and 2011 (January to March), nasopharyngeal swabs were collected from healthy children attending DCCs in the Faroe Islands. The Faroe Islands is a self-governing country under the sovereignty of Denmark with a population passing 50,000 inhabitants in 2017. Children aged ≤7 years represented about 11% of the population of the Faroe Islands. 15 In January 2012, 57 DCCs were registered in the Faroe Islands 16 and 30 DCCs were selected as study sampling sites (11 in 2009, 12 in 2010, and 7 in 2009). The DCCs were selected in different geographic locations to be representative for the Faroe Islands. The target population was ∼1000 children, of which a total of 607 with an age range from 0 to 7 years were included in the study.
Questionnaire
The parents answered a questionnaire on the use of antibiotics, vaccinations, number of siblings younger than the age of 6 years, and the occurrence of otitis media in their child. The questionnaires were returned from all the participants (100%).
Nasopharyngeal swabs
On a selected study day, two research nurses visited the DCCs after an informed consent from the parents or the legal guardians of the children had been obtained. Each child was sampled only once. The samples were obtained with a sterile medical applicator, Copan® (Transport medium swabs, Copan, Italy).
Laboratory procedures
The samples were stored for a maximum of 24 hr at 2–8°C, before they were inoculated on blood agar containing gentamicin (5 mg/L). An optochin disc (Oxoid, UK) was placed in the center and the agar plates were incubated anaerobically at 35°C for 18–24 hr. α-hemolytic colonies exhibiting morphology suggestive of S. pneumoniae were picked. Identification was obtained by susceptibility to optochin.
Antibacterial susceptibility testing
All pneumococcal isolates were tested for antimicrobial susceptibilities to erythromycin, clindamycin, tetracycline, chloramphenicol, and trimethoprim/sulfamethoxazole, using disc diffusion and the EUCAST methods and criteria (www.eucast.org). The isolates were screened for penicillin nonsusceptibility with oxacillin discs and penicillin minimum inhibitory concentration (MIC) measured for all oxacillin-resistant isolates using the E test (BioMérieux, France). Isolates with MIC ≤0.064 mg/L to penicillin were considered fully susceptible to penicillin and isolates with >0.064 mg/L were defined as PNSP.
Serotyping
Serotyping was performed by Pneumococcal Latex antisera from Statens Serum Institute, (SSI, Denmark). 17
Invasive isolates
The laboratory at the National Hospital of the Faroe Islands has a collaboration with Staten Serum Institute regarding registering and storing of bacterial isolates. Information about age, sex, susceptibility testing, serotype, and origin of the IPD isolates from 1974 to 2016 was obtained from the SSI. There were 60 pneumococcal isolates from blood and spinal fluids. Before 1978, all microbiological samples were sent to SSI for routine diagnostics. A local laboratory of clinical microbiology at the National Hospital, Faroe Islands, was established in 1978. Blood cultures were done in the Faroe Islands from 1978 to 1999 using conventional blood culture bottles, but after 1999, using the BacTec blood culturing platform. The 60 IPD isolates probably do not represent all invasive infections from 1974 until 2007, so that the exact number of IPD cases before 2007 is not known. Since 2007, all invasive pneumococci have been sent to SSI as a part of the mandatory national surveillance of pneumococcal serotypes in the Kingdom of Denmark, including the Faroe Islands.
Statistical analyses
Univariate analysis was performed using chi-square test with df = 2 < 5.991 and z-score with p value ≤0.05 considered significant. MATLAB was used to perform the statistical analyses.
Ethical approval
Ethical approval for the study was obtained from the Scientific Ethical Board of the Faroe Islands on the 7th of November in 2008, and the data collection approval was obtained from the data Protection Agency on the 6th of June in 2008.
Results
Pneumococcal carriage and results of questionnaire
Of the 607 children sampled, 45% (n = 271) carried pneumococci, 50% (133 of 265), 40% (89 of 225), and 42% (49 of 117) in the years 2009, 2010, and 2011, respectively. The difference in carriage prevalence between the years was significant (X2 = 6.03 with a critical region <5.991).
Carriage was higher in children younger than the age of 3 years (p = < 0.001). Pneumococcal carriers were significantly younger in 2009 (3.49 years) than in 2010 (4.24 years) and in 2011 (4.07 years) (p = 0.0002), and the carriage prevalence was higher in 2009 than in 2010 and 2011 (p value = 0.011) (Fig. 1).
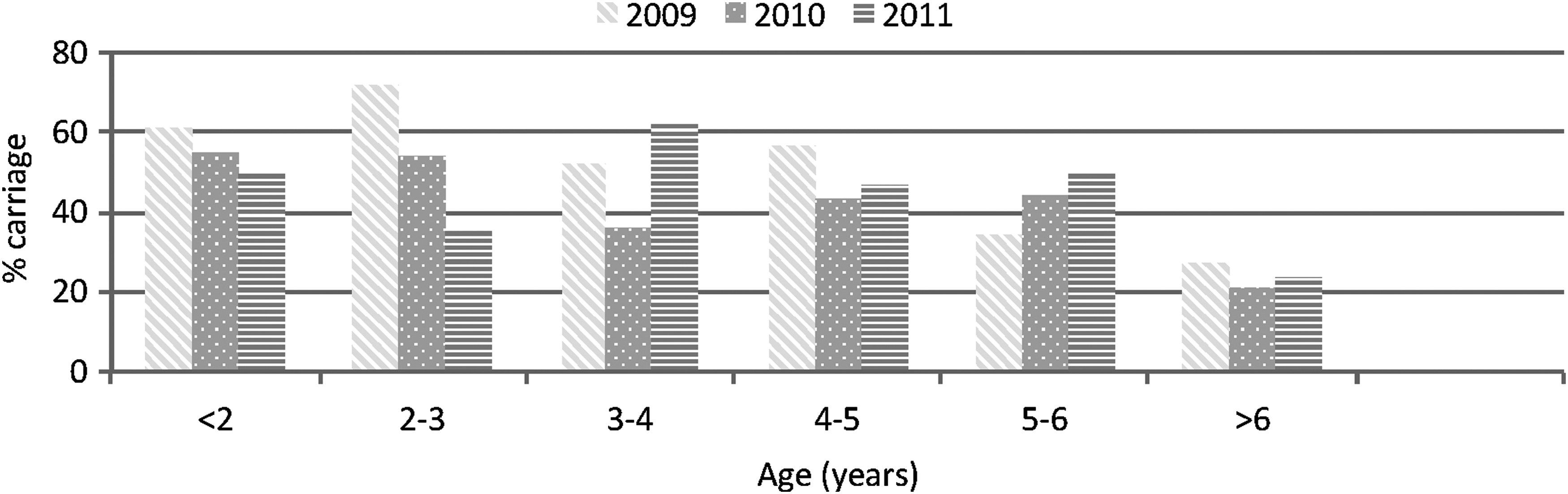
Pneumococcal carriage rate according to age in children attending DCC in the Faroe Islands in 2009, 2010, and 2011. DCC, day-care center.
Pneumococcal carriers did not use antibiotics more often than nonpneumococcal carriers. However, pneumococcal carriers used antibiotics more often in 2009 (n = 43, 32%) than pneumococcal carriers in 2010 and 2011(n = 10 and 24, 25%) (p = 0.017). The proportion of children having had otitis media and having siblings younger than the age of 6 years was the same in pneumococcal carriers and noncarriers.
Antibacterial susceptibility, vaccination, and serotype distribution
Reduced susceptibility to one or more antimicrobial was found in 15 (11.3%), 8 (9.0%), and 7 (14.3%) pneumococcal isolates in 2009, 2010, and 2011, respectively (Table 1). Erythromycin resistance was found in four isolates (Table 1). These four isolates belonged to three different serotypes (19F (n = 2) in 2009, 6C in 2010, and serogroup 11 in 2011). The erythromycin-resistant isolate of serotype 6C was also nonsusceptible to penicillin. Five PNSPs were found, three in 2009 (two serotype 19F and one nontypeable) and two in 2010 (serotype 6C and serogroup 23 [not serotype 23F]).
Antimicrobial Susceptibilities of Streptococcus pneumoniae Isolates from Children Attending Day-Care Centers in the Faroe Islands in 2009, 2010, and 2011
Resistance is listed as (R/I) and penicillin is measured in MIC.
MIC, minimum inhibitory concentrations; (R/I), resistant/intermediate.
Among the 271 isolates, 27 different serotypes were identified. The two most frequent serotypes in each year were 6B and 6A in 2009, 3 and 6C in 2010, and serogroup 11 and 6C in 2011 (Fig. 2).
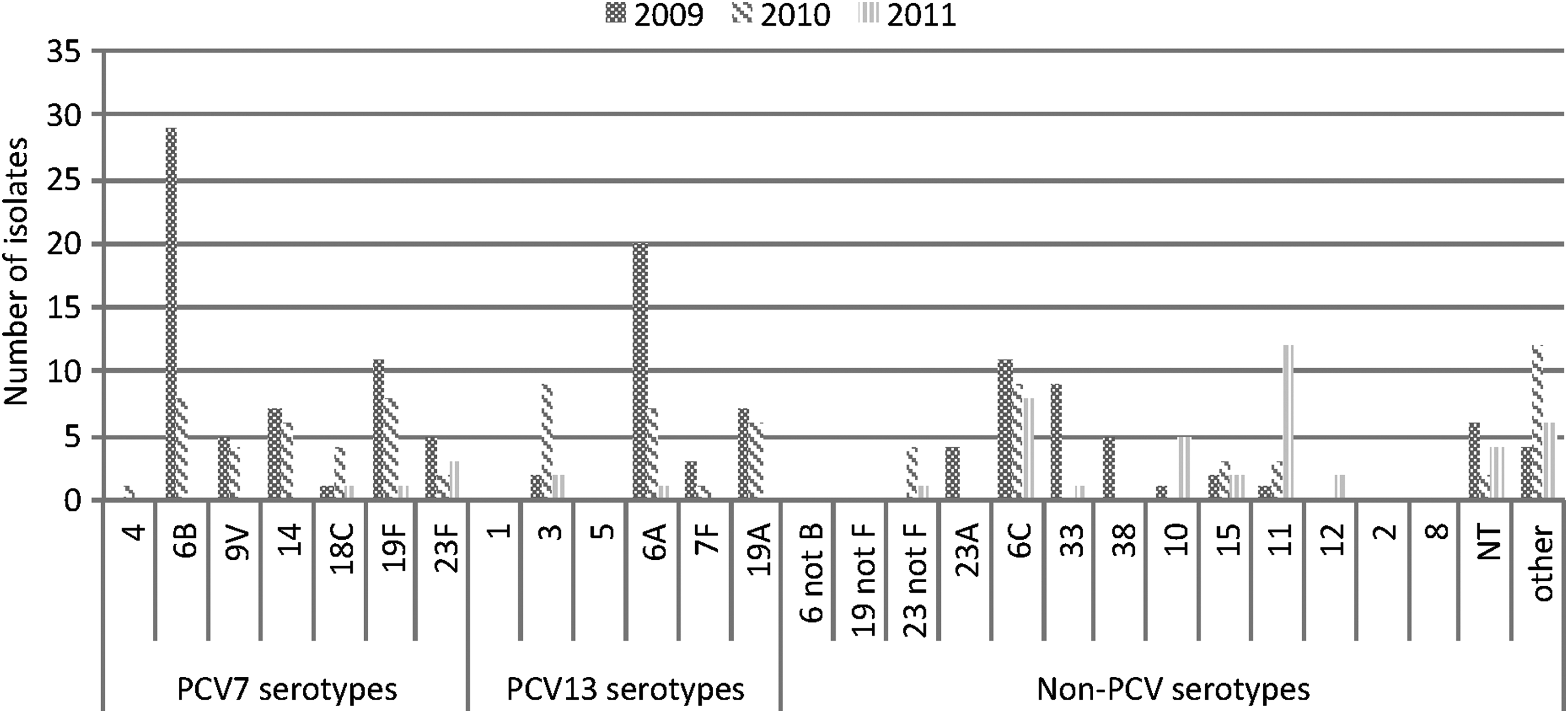
Streptococcus pneumoniae serotypes from children attending DCC in the Faroe Islands in 2009, 2010, and 2011.
In 2008, Faroese children were vaccinated with PCV-7 and in spring 2010 PCV-7 was replaced with PCV-13. In 2010, 28% children had been PCV-7/13 vaccinated, nine (10%) of which carried pneumococci. In 2011, 65% children had been vaccinated, of which 18 (37%) carried pneumococci. There was no statistical difference in vaccination status of carriers and noncarriers in 2010 and in 2011. In 2010, four fully vaccinated children carried vaccine serotypes, two with serotype 6B and two with serotype 19F, and one child vaccinated with two doses carried serotype 19A. Nine children were carriers of serotype 3 in 2010, none was vaccinated. In 2011, one child vaccinated with one dose carried serotype 23F, and one child fully vaccinated carried serotype 3. Twelve children, four of whom were fully vaccinated, were carriers of serotype 11 (Fig. 2). PCV-7 serotypes accounted for 58, 29, and 5, and additionally, PCV-13 for 32, 23, and 3 isolates in the years 2009, 2010, and 2011, respectively.
Invasive isolates—antimicrobial susceptibility and serotypes
Of the 60 invasive isolates, only one was PNSP, serotype 23B (penicillin MIC = 0.25) found in 2016. Three isolates were erythromycin resistant, one of serotype 15A in 2002, also multiresistant, and two isolates of serotype 14 in 2005 and 2006. The most frequent serotypes among invasive isolates were serotypes 3 (n = 8) and 7F (n = 7) (Table 2). Serotypes 7F and 3 were the most frequent serotypes in patients older than 7 years of age. Nine isolates of serotype 3 were recorded (in 2005, 2010, 2011, 2013, 2014, and 2016). Seven invasive isolates were from children. One 2-year-old child had the PCV-13 serotype 7F in 2010. The isolate was recovered from spinal fluid (Table 2). There was a possible decrease in PCV-7/13 serotypes among IPD from the period 2002 to 2016. From 2002 to 2006, there were 11 PCV-7/13 serotypes and 5 non-vaccine types (NVT). From 2007 to 2011, there were 21 PCV-7/13 and 1 NVT, and from 2012 to 2016, there were 6 PCV-7/13 and 9 NVT (Fig. 3).
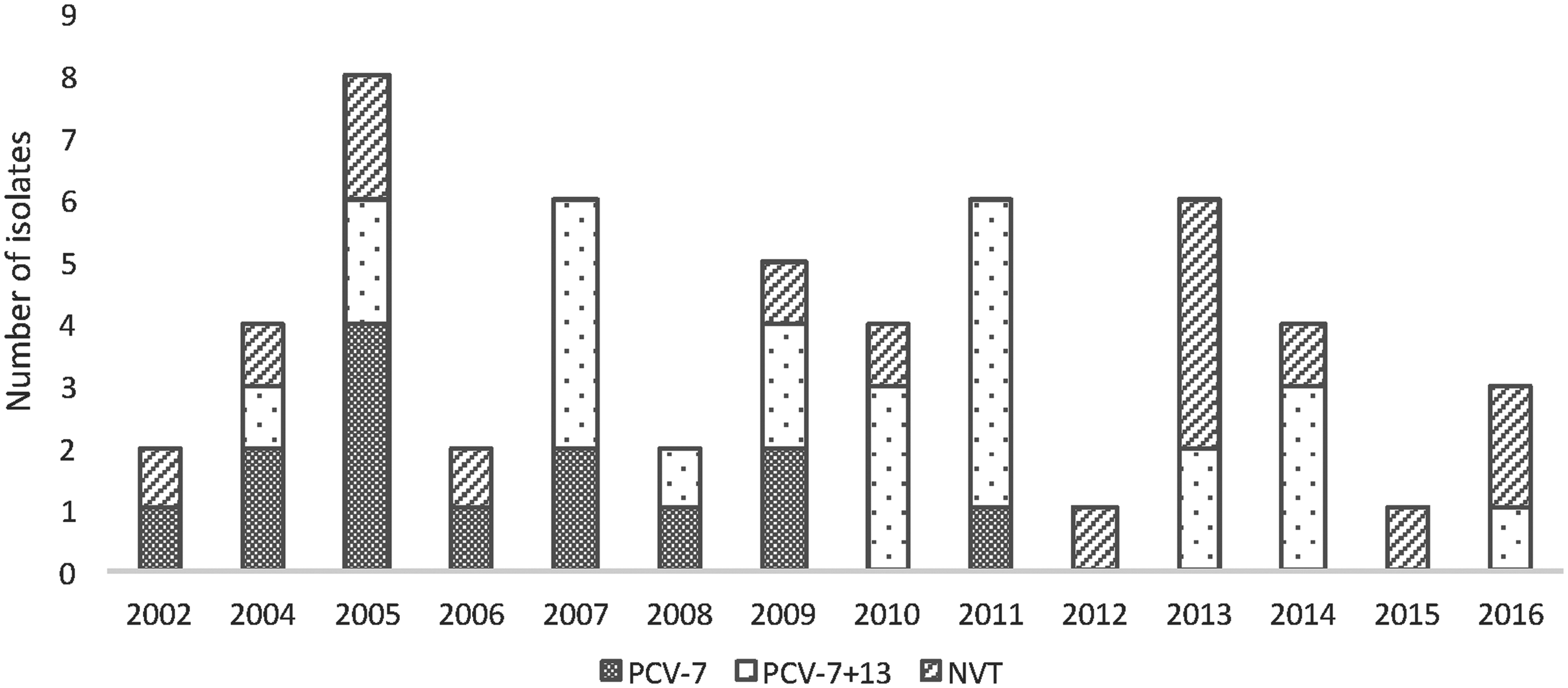
Serotype distribution in invasive isolates in the Faroese community, 2002–2016. PCV-7; serotypes 4, 6B, 9V, 14, 18C, 19F, 23F, PCV-13 serotypes in PCV-7 plus serotypes 1, 3, 5, 6A, 7F, 19A, and NVT; other than in PCV-10 and PCV-13. NVT, non-vaccine types; PCV, pneumococcal conjugate vaccine.
Serotypes of Invasive Streptococcus pneumoniae from the Faroe Islands from 1974 to 2016
Serotypes marked with bold are resistant to antimicrobials and serotypes underlined belong to PCV-7/13. PCV, pneumococcal conjugate vaccine.
Discussion
The prevalence of PNSP was low in the Faroe Islands compared with Iceland and Denmark,7,10,18–20 and this may be because of conservative use of antibiotics in the Faroese community. Our results suggest reduced antibacterial use after vaccine introduction. Antibacterial susceptibility among pneumococci in the Faroese community is similar as in Denmark, Sweden, and Norway.21–24 Another possible explanation may be that the macrolide of choice in the Faroe Islands is a short-acting erythromycin, whereas the long-acting azithromycin is mainly used in Iceland. 25 Azithromycin may have been a contributing factor to the circulation and increase of 19F clone in Iceland, which is often associated with PNSP among pneumococcal carriers. 19 The pneumococcal carriage rate in the Faroe Islands may also be a factor, for its prevalence is lower in the Faroe Islands than in Iceland and Denmark.20,26 Furthermore, the PNSP pneumococcal clones may not have the same opportunity to circulate in the Faroe Island because of its small and rural population.
A significant difference in pneumococcal carriage in the Faroe Islands was observed between the years 2009, 2010, and 2011, with the highest pneumococcal carriage in 2009. The most likely reason for the difference could be that the children were significantly younger in 2009 than in 2010 and 2011, and in our study, children younger than the age of 3 years were significantly more often pneumococcal carriers than older children, this is consistent with other studies.20,22
The most common serotypes among children attending DCCs were 6B and 6A in 2009, serotype 3 and 6C in 2010, and serotype 11 and 6C in 2011. Serotype 6B was not found in 2011. There appeared to be a serotype shift with a reduction in PCV-13 serotype carriage from 2010 to 2011, since 9 vaccinated children carried five PCV-13 serotypes in 2010, and 18 vaccinated children carried three PCV-13 serotypes in 2011.
Nine healthy children carried serotype 3 in 2010, none of them had been vaccinated, and the most common serotypes in patients were 3 and 7F, however, no children had an invasive pneumococcal infection caused by serotype 3. PCV-13 vaccination program in Denmark has not lead to a reduction of the incidence of IPD caused by serotype 3. 27 Our results suggest that this could also be the case in the Faroe Islands. Serotype 7F is considered to have high invasive potential, 28 and therefore its frequency among IPD in the Faroese community was not unexpected.
The results of the historical IPD isolates serotyped at SSI should be interpreted cautiously because of the limited information about sample processing and laboratory methods used. The Faroe Islands did not have an IPD surveillance before 2007, and therefore, there could have been more IPD cases than the 60 recorded. Iceland and Denmark reported higher number of invasive pneumococci than the Faroe Islands, 29 and the small numbers of isolates from the Faroe Islands may therefore not give a true representation of the Faroese situation.
In conclusion, pneumococcal carriage rates in children attending DCCs were lower than in the neighboring countries, and antimicrobial resistance in pneumococci was extremely rare in the Faroe Islands. Pneumococcal vaccination has probably reduced the incidence of PCV-7/13 serotypes among IPD cases, and there is indication of serotype shift in pneumococcal carriage in DCCs. Further monitoring is important to detect new serotypes in invasive disease and changes in disease prevalence.
Footnotes
Acknowledgments
The authors thank Elna Krosstein, and Sunneva Petersen, Tórshavn, Faroe Islands, for sampling pneumococcal isolates from children attending DCCs. We acknowledge the Statens Serum Insitut (SSI) for the data of the invasive pneumococcal isolates and Hjálmar Hátún, Tórshavn, Faroe Islands, for the planning and helping with the statistical analysis. This work was supported by a grant from the Faroese Research Council, BP Amoco, Chevron Texaco, Eik vísindagrunninum, and SSAC foundation.
Disclosure Statement
No competing financial interests exist.