
Abstract
Vancomycin-resistant Enterococci (VRE) are a major public health problem worldwide, since they are commonly implicated in nosocomial infections in various regions in the world. The aim of our study was to investigate genetic features and clonal relationship of VRE in the Military hospital of Tunisia. A total of 10 VRE strains were initially detected and identified by the Viteck II compact® (BioMérieux®) automated system, then confirmed by PCR using specific primers. These VRE strains were isolated during the period extended between September 2015 and January 2017 from anal and blood samples from patients hospitalized mainly in the neonatology service and intensive care unit. All these strains were identified as Enterococcus faecium and carried the vanA gene. Other acquired resistance genes were also detected by PCR: [ermB (n = 6); tetL (n = 6); tetM (n = 2); aac(6′)-Ie-aph(2′′)-Ia (n = 10); aph(3′)-III-a (n = 9); ant(6)-Ia (n = 8)]. The insertion sequence IS16 was detected in all our tested strains. Esp virulence gene was detected in only one strain. The clonal relatedness of VRE strains screened by pulse-field gel electrophoresis and multi-locus sequence typing showed four clones: two related clones A1 (one strain) and A2 (one strain) ascribed to ST80 belonged to CC17, the other remaining two clones, named B (one strain) and C (seven strains), revealed two new sequences types assigned to ST1463 and ST1464 respectively. The emergence of novel clones of VRE in this hospital could be a warning of rapid evolution of these resistant bacteria, which calls for new surveillance strategies, strict hygiene and practices.
Introduction
Vancomycin-resistant enterococci (VRE) are a major public health problem worldwide, since they are commonly implicated in nosocomial infections in various regions in the world.1–4 This quick and uncontrolled spread of VRE is due to several factors such as horizontal transmission, antimicrobial consumption, hygiene practices, and mobile genetic elements.5–9 All these factors could complicate the situation while limiting therapeutic options and increasing hospital stay and mortality rates.10,11 The most common acquired vanA and vanB genes were mainly detected in Enterococcus faecium and E. faecalis species, which are implicated in several infections especially in compromised patients.12–14
In Tunisia, the first detection of vancomycin-resistant Enterococci has been reported since 2007 when two strains of E. faecium containing vanA gene were isolated from two elderly patients hospitalized in the south of the country. 15 Later, vanA containing E. faecium strains have been isolated in the Military Hospital of Tunis in part from patients and in the other part from the environment of the hospital.6,16 To date, three sequences types (ST80, ST18, and ST910) have been detected in Tunisia showing the spread of same clones belonging to clonal complex CC17 usually causing hospital outbreaks.14,17
The aim of our study was to investigate genetic features and clonal relationship of vancomycin-resistant E. faecium circulating in the Military hospital of Tunisia. This study will also shed light on the evolution of VRE in the hospital and determine whether the prevailing clones are related to VRE clones previously detected in this hospital.6,16
Materials and Methods
Bacterial isolates
This study was conducted on 10 VRE isolated from clinical specimens from patients attending the Military Hospital of Tunis during the period extended between September 2015 and January 2017. These VRE strains were initially detected and identified by the Viteck II compact® (BioMérieux®) automated system and then confirmed by PCR using specific primers for species identification as previously described. 18
Resistance genes
The detection of aqcuired genes conferring resistance to various antimicrobial agents: [vanA and vanB for resistance to vancomycin; tetM and tetL for resistance to tetracyclin; ermB for resistance to erythromycin; aac(6′)-Ie-aph(2′′)-Ia for resistance to gentamicin; aph(3′)-III-a for resistance to kanamycin; ant(6)-Ia for resistance to streptomycin] was performed by PCR using primers previously described. 19
Virulence genes
The two virulence genes esp (enterococcal surface protein) and hyl (encoding a hyaluronidase-like protein) usually associated with VRE clones causing hospital outbreaks, were tested in our strains by PCR using primers previously described. 20
Pulse-field gel electrophoresis
The clonal relatedness of our VRE strains was screened using pulse-field gel electrophoresis (PFGE) according to Tenover et al. 21 The genomic DNA of our isolates was digested with SmaI restriction enzyme and the dendrogram of banding patterns was prepared by FPQuest software using UPGMA algorithm.
Multi-locus sequence typing
Seven housekeeping genes (atpA, ddl, gdh, purK, gyd, pstS, and adk) of our VRE strains were amplified, sequenced, and analyzed in the PubMLST website database to assign a specific sequence type (ST) to our detected clones.
Insertion element IS16
The presence of the insertion element IS16 (marker of hospital outbreaks) in our VRE strains was tested using primers as previously described. 22
Results
A total of 10 VRE strains were isolated from clinical specimens in the Military hospital of Tunis during the period extended between September 2015 and January 2017. All of these strains were identified as E. faecium and carried the vanA gene. These VRE strains were mainly isolated from anal and blood samples from patients hospitalized in the neonatology service and in the intensive care unit (Table 1). Only one VRE strain was isolated from a pus sample from an outpatient.
Characterization of Vancomycin-Resistant Enterococcus faecium Isolated from the Military Hospital of Tunis
MIC, minimal inhibitory concentration; PFGE, pulse-field gel electrophoresis
All VRE strains showed high minimal inhibitory concentration (MIC) for vancomycin (MIC VAN ≥256 μg/mL) and teicoplanin (32–64 μg/mL). Moreover, in addition to vancomycin and teicoplanin, all our VRE strains were resistant to the majority of antibiotics tested: erythromycin, tetracyclin, gentamicin, and kanamycin.
Acquired resistance genes detected by PCR in our VRE strains were as follows: ermB gene conferring resistance to erythromycin was detected in six strains; tetL and tetM genes conferring resistance to tetracycline were detected in six and two strains respectively; aac(6′)-Ie-aph(2′′)-Ia gene conferring high level resistance to gentamicin was detected in all of our VRE strains; aph(3′)-III-a gene conferring resistance to kanamycin was detected in nine strains and ant(6)-Ia gene conferring resistance to streptomycin was detected in eight strains (Table 1). The virulence gene esp encoding enterococcal surface protein was detected in only one strain isolated from a blood sample of a patient hospitalized in the intensive care unit, however, the virulence hyl gene was not noted. The insertion element IS16, which is a marker of hospital outbreaks, was detected in all of our strains.
The clonal relatedness of VRE strains screened by PFGE and multi-locus sequence typing (MLST) showed four clones (Fig. 1). Two related clones A1 (one strain) and A2 (one strain) ascribed to ST80 belonged to CC17. These two strains were isolated during January 2017 from the blood of one patient in the Intensive Care Unit and from the pus of one outpatient. The other remaining two clones named B (one strain) and C (seven strains) isolated during 2015 showed two new sequences types with the following allele combination: [Pulsotype B: atpA (9), ddl (1), gdh (1), purK (1), gyd (4), pstS (14), and adk (1); Pulsotype C: atpA (70), ddl (1), gdh (38), purK (29), gyd (12), pstS (14), and adk (1)] (Table 2). These two new sequences types were submitted to the MLST website and were assigned to ST1463 and ST1464 respectively. Only one strain showed pulsotype B, it has been isolated from the blood of one patient hospitalized in the intensive care unit. However, the remaining other strains of the pulsotype C were isolated from anal samples of seven patients hospitalized in the neonatology service during the same period.
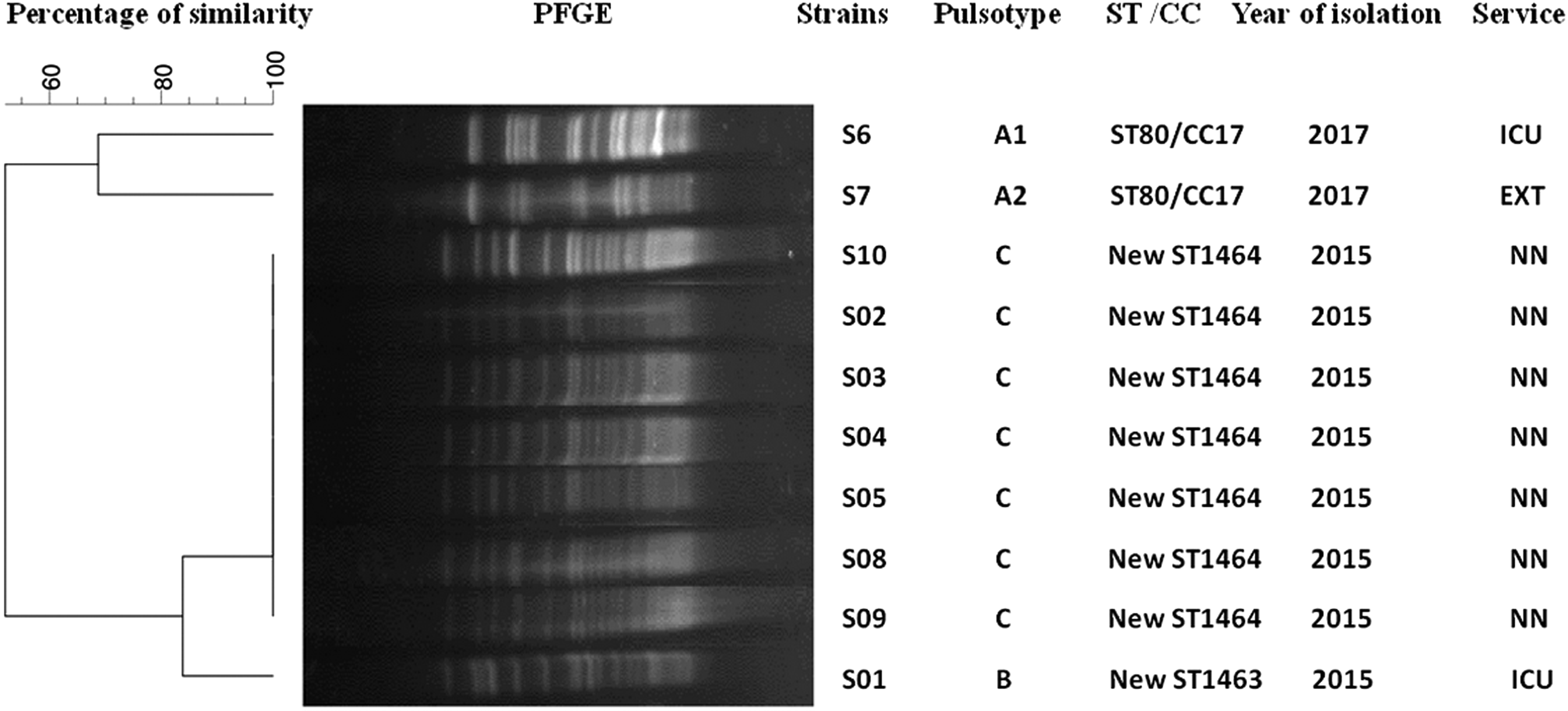
Dendrogram prepared by FPQuest software (version 5) using UPGMA algorithm of PFGE patterns of SmaI digested DNA of 10 vancomycin-resistant Enterococci strains. PFGE, pulse-field gel electrophoresis; ICU, intensive care unit; NN, neonatology; EXT, externe.
Results of Multi-Locus Sequence Typing
Discussion
To date, few studies have reported the presence of VRE in hospital settings in Tunisia: only three published articles have described the emergence of this resistant pathogen that remains uncommon.6,15,16 Further studies are needed to assess the epidemiological situation of these pathogens in our hospital and to establish adequate measures for control of VRE infections. In this study, a total of 10 VRE strains were isolated from clinical specimens from September 2015 until January 2017.
With respect to the number of detected VRE strains during the study period, it is notable that the rate of these emerging resistant pathogens is low compared with other countries with very high VRE frequencies.23–28 In our country, acquired vancomycin resistance has only been detected in E. faecium with vanA gene. Nevertheless, in other countries this acquired resistance has been detected in both E. faecium and E. faecalis and conferred either by the vanA gene or vanB gene and in some cases by both of them.29–32
Our VRE strains were mainly isolated from patients hospitalized in the intensive care and neonatology service, this could be explained by both the vulnerability of patients in these services and an endemic situation in the hospital, especially that those resistant bacteria are always associated with outbreaks.33–36 Resistance to vancomycin in our strains was associated with resistance to other antibiotics such as erythromycin, tetracyclin, kanamycin, gentamicin, and streptomycin. This multiresistance in VRE strains has been reported by other investigators all over the world and was explained by the fact that the vanA gene could be mobilized with other antibiotic resistance genes by the same mobile genetic element.9,31,37
All strains contained the insertion element IS16 usually known as the marker of hospital outbreaks especially of the clonal complex CC17. 22 It has also been reported that the insertion element IS16 provides genomic flexibility, thus facilitating the acquisition of virulence factors or drug resistance mechanisms. 38
The virulence esp gene encoding the enterococcal surface protein was detected in only one strain, this gene is commonly detected in VRE strains belonging to the clonal complex CC17 39 and it has been reported that it could play a role in the biofilm formation. 40 The molecular typing of our VRE strains by PFGE and MLST showed that there is a clonal spread in this hospital. In fact, it has been noted that two strains isolated during 2017 were ascribed to ST80/CC17, and the remaining other strains, isolated during 2015 showed two unrelated pulsotypes and were ascribed to two new sequences types (ST1463 and ST1464) indicating an endemic situation in this hospital.
Most of our VRE isolates were recovered from anal swabs from patients hospitalized in the neonatology service. These strains belonged to the same clone and were recovered in the same period (2015), showing the cross-transmission of VRE which succeeds to colonize patients in the same service. This colonization could progress into infections depending on patients' health status. 41 In fact, patients received in the neonatology service may carry several risk factors, including long hospital stay, low birth weight, weakened host immune system, promoting VRE colonization and infection. 42
Our study showed the persistent circulation of VRE in hospitals in Tunisia, this calls for setting up a new surveillance program to restrict the spread of these resistant bacteria.
Footnotes
Acknowledgments
This work was supported by the Tunisian Ministry of Higher Education and Scientific Research and by the Military hospital of Tunisia.
Disclosure Statement
No competing financial interests exist.