
Abstract
Hypervirulent Klebsiella pneumoniae (hvKp) can cause severe invasive infections in healthy and immunocompromised individuals. However, there is still lack of a consensus definition of hvKp. In this study, we solely focused on the clinical isolates cultured from subcutaneous drainage of community-acquired liver abscess cases, and an hvKp strain was defined on the basis of co-harboring virulence gene regulator of mucoid phenotype A (rmpA)/rmpA2, iucA, iroB, and peg-344. A total of 47 nonrepetitive hvKp isolates were collected from January 2015 to December 2017 in a tertiary teaching hospital in Shanghai, China. All isolates were susceptible to the commonly used antibiotics. Only one strain (RJ-Kp24) had the positive detection of blaCTX-M-14 and was resistant to ceftazidime, cefotaxime, and cefepime. S1-pulsed-field gel electrophoresis (PFGE) and southern hybridization confirmed the presence of a roughly 90 kb blaCTX-M-14-carrying plasmid and a roughly 240 kb virulence plasmid. Further analysis revealed that ST23 (n = 17) sequence type and K1 (n = 20) and K2 (n = 9) serotypes were dominant in hvKp, while only 31.9% (15/47) and 46.8% (22/47) of hvKp isolates displayed hypermucoviscosity and resistance to serum killing, respectively. For further evaluation of the pathogenicity of hvKp, six representative strains were randomly selected. Three strains, RJ-Kp10, RJ-Kp28, and RJ-Kp31, displayed a remarkable resistance to serum killing and neutrophil phagocytosis. Mouse lethality assay revealed that these strains had the 50% lethal dose (LD50) of 102-103 cell forming unit (CFU), while others had the LD50 of 104–105 CFU. These results demonstrated that strain virulence differed significantly within these defined hvKp. The convergence of multidrug resistance and enhanced virulence in K. pneumoniae has presented a major infection control challenge.
Introduction
Klebsiella pneumoniae is a common opportunistic pathogen responsible for nosocomial infections, such as pneumonia and urinary tract infections. In mid-1980s, a new variant of K. pneumoniae causing invasive pyogenic liver abscess was first described in Taiwan 1 and, subsequently, found worldwide, especially in Asia. 2 Different from the classical K. pneumoniae (cKp), the new variants of K. pneumoniae often showed hypermucoviscosity when grown on agar plates, with the formation of a viscous string of greater than 5 mm in length stretched by the inoculation loop (a positive “string test”). 3 These strains were much more resistant than cKp to in vitro killing by serum or phagocytosis by neutrophils and macrophages, thus have also been referred to as hypervirulent K. pneumoniae (hvKp). 3 In addition, hvKp is able to produce liver abscess and other invasive infections at various sites, such as eye and brain.4,5 Retrospective studies showed that K. pneumoniae has been the main cause of community-acquired pyogenic liver abscess in China, as well as in other Asian countries.6,7
Since hvKp strains often form colonies with a hypermucoviscous phenotype, a positive “string test” has been widely used for identification of hvKp. 8 However, nonhypermucoviscous hvKp has also been repeatedly reported.9,10 Although most hvKp have K1 or K2 capsular serotypes, non-K1/K2 serotype hvKp strains have also been reported and some K1/K2 strains were also classified as cKp.11,12 Besides, several sequence types (STs) have been shown to be associated with hvKp. For example, ST23 is mostly associated with K1 serotype, whereas ST86 and ST65 are often associated with K2.2,13 However, hvKp strains with other STs have also been reported. 11 Overall, it is difficult to define the hvKp strain solely based on colony phenotype, serotyping, or sequence typing.
Several virulence factors have been identified to be associated with hvKp, including siderophores aerobactin (iucABCDiutA), salmochelin (iroBCDN), and the gene rmpA/A2.14–16 Siderophores are important virulence factors that scavenge ferric iron from the environment. Both siderophores and rmpA/A2 are located on a large virulence plasmid and are found almost in all reported hvKp strains. 17 Furthermore, genomic analysis also supported the presence of large virulence plasmid in hvKp and that plasmid-encoded iucABCDiutA, iroBCDN, and rmpA/A2 were tightly associated with hvKp.17,18
Although a consensus definition of hvKp does not exist, an improved working definition was recently proposed. The presence of the biomarkers rmpA/rmpA2, iucA, iroB, and peg-344 strongly correlates with the hvKp phenotype, which was validated with a murine infection model. 19 In this study, we took the clinical features into account combined with microbiological genotypes. We solely focused on the clinical isolates cultured from subcutaneous drainage of community-acquired liver abscess cases, and an hvKp strain was defined on the basis of co-harboring virulence genes rmpA/rmpA2, iucA, iroB, and peg-344. Forty seven nonrepetitive community-acquired hvKp were collected. The antimicrobial susceptibility testing was performed, and serum killing, neutrophil phagocytosis, and mouse lethality assays were used to estimate the pathogenicity of these hvKp strains.
Materials and Methods
Clinical isolates
Subcutaneous drainage samples were collected from patients who had been clinically diagnosed with community-acquired liver abscess and received ultrasound-guided drainage from January 2015 to December 2017 in a tertiary teaching hospital in Shanghai, China. The percutaneous drainage was performed within 24 hr of admission. This hospital consists of three branch courts in different areas of Shanghai, thus making it possible for having the full view of primary liver abscess cases in this city. All K. pneumoniae isolates were identified by MALDI Biotyper™ (Bruker, Billerica).
Antimicrobial susceptibility testing
The minimum inhibitory concentrations (MICs) were determined for meropenem and imipenem using the Clinical and Laboratory Standards Institute (CLSI) reference broth microdilution method. 20 Comparator agents included ceftazidime, aztreonam, cefepime, piperacillin/tazobactam, ciprofloxacin, amikacin, and sulfamethoxazole/trimethoprim. Quality control strains tested concurrently included Escherichia coli ATCC 25922 and ATCC 35218, and MICs were interpreted according to CLSI breakpoints. 20 Besides, the production of extended spectrum β-lactamases (ESBLs) was also determined by Vitek 2 Compact System (BioMerieux, France).
Screening for ESBL genes
Polymerase chain reaction (PCR) detection of ESBLs (blaCTX-M, blaSHV, and blaTEM) was performed. 21 PCR was performed with the following program: Initial denaturation at 94°C for 1 min, 30 cycles of 94°C 20 sec, 54°C 20 sec, and 72°C 1 min, with final extension at 72°C for 5 min. PCR amplicons were sequenced and compared with sequences available in the GenBank database using BLAST searches. S1-PFGE and southern hybridization were performed for localization of the resistance plasmid, with DIG High Prime DNA Labeling and Detection Starter Kit II (Roche, Switzerland). Conjugation assay of the resistance plasmid was performed by filter mating as previously described. 22
Multilocus sequence typing analysis
Multilocus sequence typing (MLST) with seven housekeeping genes (gapA, infB, mdh, pgi, phoE, rpoB, and tonB) was performed for all clinical isolates. 23 Multiple sequence alignment analysis was conducted according to the online MLST database of the Institute Pasteur.
String test
String test was used to identify the hypermucoviscosity phenotype of clinical isolates. A positive string test was defined as the formation of a viscous string >5 mm in length when a colony grown overnight on a blood agar plate at 37°C was stretched by the inoculation loop. 8
Detection of virulence factors
Capsular type was determined through wzi gene sequencing. 24 This gene was conserved in all capsular types of K. pneumoniae that codes for an outer membrane protein involved in capsule attachment to the cell surface. The iucA, rmpA, rmpA2, iroB, peg-344, and kfu genes were detected by PCR as described previously.18,19 PCR was performed with the following program: Initial denaturation at 94°C for 1 min, 30 cycles of 94°C 20 sec, 54°C 20 sec, and 72°C 1 min, with final extension at 72°C for 5 min. S1-PFGE and southern hybridization were performed for localization of the virulence plasmid as previously described, 25 with DIG High Prime DNA Labeling and Detection Starter Kit II.
Serum killing assay
Human blood was obtained from healthy individuals, and serum killing assay was performed as previously described. 2 An inoculum of 25 μL of bacterial suspension prepared from the mid-log phase was mixed with 75 μL of serum. Viable counts were checked at 0, 1, 2, and 3 hr of incubation at 37°C. Each strain was tested at 3 times, and the mean results were expressed as percent inoculums. The responses in terms of viable counts were graded from 1 to 6, as previously described. 2 A strain was defined as serum sensitive at grades of 1–2, intermediately sensitive at 3–4, and resistant at 5–6.
Neutrophil phagocytosis assay
Neutrophils were isolated from venous blood of healthy volunteers with Ficoll-Hypaque gradient density centrifugation. To measure neutrophil bactericidal activity, neutrophils were combined with bacteria in 1.5 mL Eppendorf tubes, with 106 neutrophils plus 107 cell forming unit (CFU) K. pneumoniae in 500 μL final volume. The mixture was incubated at 37°C for 1 hr with gentle rotation. Viable counts were checked at 0, 15, 30, and 60 min of incubation. 26 Before CFU counts, saponin (0.1% final concentration) was added to each tube, and the tubes were chilled on ice for 15 min before diluting and plating on Luria-Bertani (LB). Each strain was tested at three times, and the mean results were expressed as percent inoculums.
Mouse lethality assay
To determine the 50% lethal dose (LD50), pathogen-free, 6–8-week-old, female BALB/c mice were used. Ten-fold serial dilution of CFU of K. pneumoniae was made from a starting concentration of 106 to 103 CFU/mL, and BALB/c mice were infected intraperitoneally with 0.1 mL of each concentration. A number of six mice were used as a sample population for each bacterial concentration. Symptoms and mortality rates were observed for 7 days. The exact inoculation dose was confirmed on LB agar, and the LD50 was calculated using the SigmaPlot (version 11.0) program.
Statistical analysis
Categorical variables were summarized as numbers (percentages). Pearson's two-sided chi-square test or, if the expected count in any cell was less than five, Fisher's exact test was used to compare these data. For the continuous variables generated from neutrophil phagocytosis assay, one-way analysis of variance (ANOVA) was used for comparison among the six strains. Data analysis was carried out with Intercooled Stata v.12; p < 0.05 was considered to be statistically significant.
Results
Clinical characteristics of patients with hvKp infection
A total of 103 patients diagnosed with community-acquired liver abscess were enrolled from January 2015 to December 2017. Among them, 88 (85.4%) patients received percutaneous drainage therapy. Drainage samples were collected, and the overall positive bacterial culture was 69.3% (61/88), of which 86.9% (53/61) were identified as K. pneumoniae. A total of 47 isolates were co-harboring virulence genes rmpA/rmpA2, iucA, iroB, and peg-344 and were defined as hvKp.
As shown in Table 1, 22 (46.8%) of all 47 patients with hvKp infection were with diabetes mellitus, and 32 (68.1%) community-acquired liver abscess cases occurred in the right lobe. Metastatic infections of endophthalmitis were also observed in two patients. Most of the patients received cephalosporin based antimicrobial therapy, while only one patient died largely due to the serious underlying conditions.
Clinical Characteristics of Klebsiella pneumoniae Associated Community-Acquired Liver Abscess
IQR, interquartile range.
Microbiological characteristics of hvKp
All hvKp isolates were susceptible to aztreonam, imipenem, meropenem, piperacillin–tazobactam, and amikacin (Table 2). MLST analysis revealed a total of 24 STs, and ST23 (n = 17) was the dominant ST, followed by ST412 (n = 4), ST29 (n = 4), ST65 (n = 3), and ST86 (n = 2) (Table 3). K1 serotype (20/47) was dominant in hvKp, followed by K2 (9/47), and the majority of K1 strains (17/20) belonged to ST23. Although all hvKp strains carried the virulence genes rmpA/rmpA2, only 31.9% (15/47) of them displayed a positive string test, whereas 46.8% (22/47) were proved to be resistant to serum killing (Table 3).
Antimicrobial Susceptibility Testing of Community-Acquired Hypervirulent Klebsiella pneumoniae
MIC, minimum inhibitory concentration; S, susceptible; SMZ-TMP, sulfamethoxazole/trimethoprim.
Microbiological Characteristics of Community-Acquired Hypervirulent Klebsiella pneumoniae
A strain was defined as serum sensitive at grades of 1–2, intermediately sensitive at 3–4, and resistant at 5–6.
ESBLs, extended spectrum β-lactamases; hvKp, hypervirulent K. pneumoniae; MLST, multilocus sequence typing; rmpA, regulator of mucoid phenotype A; STs, sequence types.
As shown in Table 4, ST23, ST65, and ST86 were confined to K1/K2 serotype strains. No significant differences on the detection rates of hypermucoviscosity phenotype and the plasmid mediated virulence determinants rmpA and rmpA2 were observed between the two groups (p > 0.05). Interestingly, K1/K2 serotype strains displayed higher resistance to serum killing than those of other serotype strains (p < 0.05).
Comparison of Microbiological Characteristics Between K1/K2 and Other Serotypes of hypervirulent Klebsiella pneumoniae Strains
The values in bold are statistically significant.
Pearson's two-sided chi-square test or, if the expected count in any cell was less than five, Fisher's exact test was used. Data analysis was carried out with Intercooled Stata v.12; p < 0.05 was considered to be statistically significant.
A strain was defined as serum sensitive at grades of 1–2, intermediately sensitive at 3–4, and resistant at 5–6.
Only one strain (RJ-Kp24), with ST of ST1333, was proved to be ESBL positive and was resistant to ceftazidime, cefotaxime, and cefepime. PCR screening revealed the positive detection of blaCTX-M-14 and blaSHV-11. S1-PFGE demonstrated that there were two plasmids in strain RJ-Kp24, and southern hybridization confirmed the presence of a roughly 90 kb blaCTX-M-14-carrying plasmid and a roughly 240 kb virulence plasmid (Fig. 1). The blaCTX-M-14-carrying plasmid could be transferred to E. coli strain J53 through conjugation assay, at frequencies of 10−4 transconjugants per donor cell.
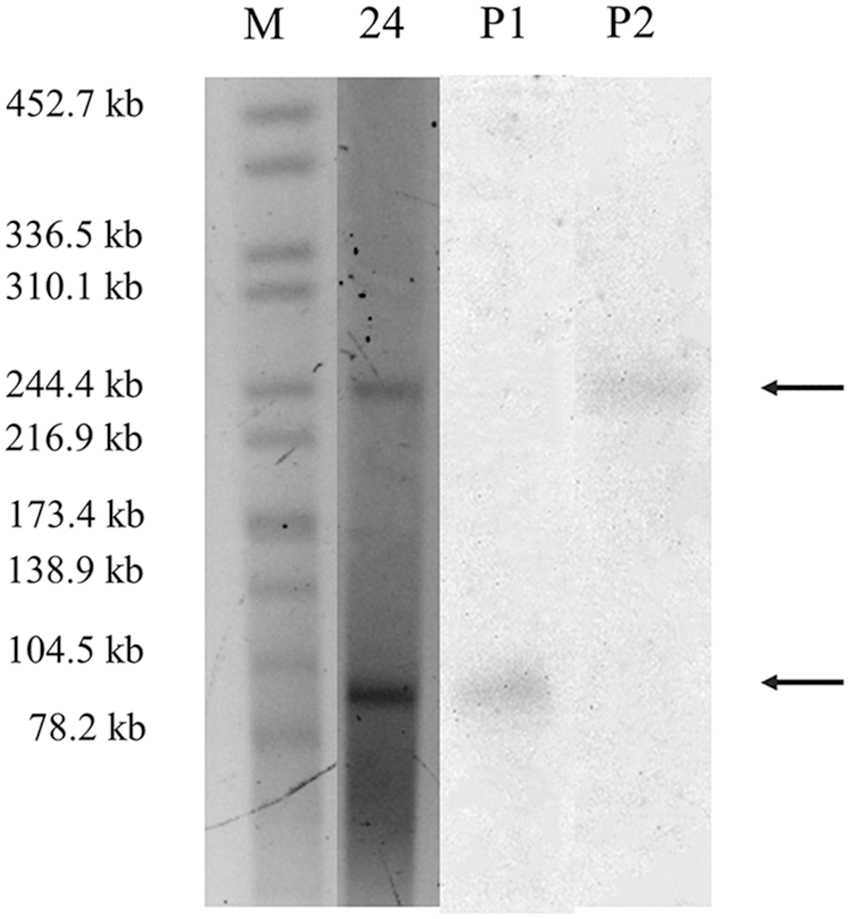
S1-PFGE and southern hybridization of the ESBL-producing strain RJ-Kp24. Numbers represented the strains' codes. M: DNA marker. P1, southern hybridization of the blaCTX-M-14-harboring plasmid with marker gene blaCTX-M-14, which was hybridized to a roughly 90 kb resistance plasmid. P2, southern hybridization of the virulence plasmid with marker gene rmpA2, which was hybridized to a roughly 240 kb resistance plasmid. ESBLs, extended spectrum β-lactamases; rmpA, regulator of mucoid phenotype A.
In vitro and in vivo virulence estimation of hvKp
For further evaluation of the pathogenicity of hvKp, six representative strains were randomly selected. Three strains, RJ-Kp10, RJ-Kp28, and RJ-Kp31, displayed a remarkable resistance to serum killing and neutrophil phagocytosis. Mouse lethality assay revealed that these three strains had the LD50 of less than 102–103 CFU, while others had the LD50 of 104–105 CFU (Table 5).
Mouse Lethality Assay of the Selected Hypervirulent Klebsiella pneumoniae Strains
R, a phagocytic rate of <50% at 30 min; S, a phagocytic rate of ≥50% at 30 min.
A strain was defined as serum sensitive at grades of 1–2, intermediately resistant at 3–4, and resistant at 5–6.
LD50, 50% lethal dose; CFU, cell forming unit.
Discussion
There is still lack of a consensus definition of hvKp. In this study, we took the clinical features into account combined with microbiological genotypes. We solely focused on the clinical isolates cultured from subcutaneous drainage of community-acquired liver abscess cases, and an hvKp strain was defined on the basis of co-harboring virulence genes rmpA/rmpA2, iucA, iroB, and peg-344. On other aspects, previous studies have also defined hvKp upon the demonstration of a positive string test. 27 However, only 31.9% (15/47) of clinical isolates in this study showed hypermucoviscosity. Similarly, a recent study conducted in east China with 45 liver abscess associated K. pneumoniae strains also reported that only 28.9% (13/45) of the strains displayed a positive string test. 28 In other words, a definition solely relying on a positive string test may possibly exclude a relative number of hvKp from community-acquired liver abscess associated K. pneumoniae strains.
Although various definitions of hvKp have been used in previous studies, the pathogenicity of defined hvKp has seldom been determined. In the current study, ST23 (n = 17) ST and K1 serotype (n = 20) were dominant in defined hvKp. All hvKp strains had the positive detection of virulence genes rmpA/rmpA2, iucA, iroB, and peg-344. However, only 46.8% (22/47) of hvKp strains displayed resistance to serum killing. Furthermore, mouse lethality assay revealed that the LD50 of the six representative strains ranged from 102–105 CFU. Generally, strain virulence differed significantly within hvKp in this study. Although mouse lethality assay is accurate for identification of hvKp, it is time consuming and rather difficult to perform; thus, this definition has not been widely applied.
K. pneumoniae has been the leading cause of community-acquired liver abscess in China, as well as in other Asian countries. 6 Fortunately, liver abscess associated hvKp has been relatively susceptible to commonly used antimicrobial agents. All hvKp isolates in the current study were susceptible to imipenem, meropenem, piperacillin–tazobactam, amikacin, and aztreonam. Only one strain (RJ-Kp24) had the production of ESBLs, with the positive detection of blaCTX-M-14, and was resistant to ceftazidime, cefotaxime, and cefepime. CTX-M-14 belonged to CTX-M group 9 variants and was dominant in China, South-East Asia, South Korea, and Japan. 29 The horizontal gene transfer of blaCTX-M-14 on the conjugative plasmid contributes to the formation of multidrug resistant hvKp. Furthermore, clinical K. pneumoniae isolates with combined virulence and resistance have been increasingly reported, especially for the carbapenem-resistant hvKp isolates. 25 The convergence of multidrug resistance and enhanced virulence in K. pneumoniae has the potential to cause the next clinical crisis.
Rapid diagnosis and appropriate antimicrobial treatment have significantly improved the clinical outcome of patients with community-acquired K. pneumoniae liver abscess and prevent metastatic complications. However, hvKp is able to produce invasive infections at various sites. If clinical therapy can be individualized based on the predicted virulence of the specific strain, there could be a significant impact on the treatment of hvKp infections. The distinct clinical behaviors of hvKp and cKp strains also make it possible to reach a consensus definition of hypervirulence in K. pneumoniae. In contrast, further investigations are also needed to identify the environmental reservoir for these hvKp strains.
Footnotes
Ethical Approval
All procedures performed in this study involving human participants and animals were in accordance with the ethical standards of the Institutional Review Board Ethics Committee of Renji Hospital. For this type of study formal consent is not required.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by National Natural Science Foundation of China (Grant nos. 81802065), Shanghai Sailing Program (Grant no. 18YF1413300), and a research fund from Renji Hospital for young scholars (Grant no. PYIII-17-010). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the article.