
Abstract
An essential part of the Israeli intervention program aimed to contain the spread of carbapenemase-producing Enterobacterales (CPE) has been the establishment of national surveillance system, where the institutional rates are determined by both clinical and surveillance cultures. The objectives of the study were to analyze the effect of changes in surveillance culture media on the rates and microbiological characteristics of CPE in a multicenter study. The rates were compared during 2 years in and between four centers. Two centers (Tel-Aviv and Beilinson) had changed their surveillance media to CHROMagar™ mSuperCARBA™ after 1 year, and two centers (Rambam and Hillel-Yaffe) had continued to use CHROMagar KPC. There was an increase in the rates of surveillance CPE in Tel-Aviv and Beilinson following the change in media, whereas the rates remained the same or declined in Rambam and Hillel-Yaffe, respectively. The rates of clinical CPE remained unchanged in Rambam and Hillel-Yaffe, declined in Tel-Aviv, and increased in Beilinson but to a lesser extent compared with the increase in surveillance CPE. The relative composition of the CPE mechanisms and species changed in Tel-Aviv, with an increase in non-Klebsiella pneumoniae species and in carbapenemase other than KPC. Our study shows that changes in surveillance media may contribute to significant changes in the rate of surveillance CPE that may be irrespective of actual epidemiological changes. Therefore, determination of institutional burden of CPE and the assessment of intervention results should be based primarily on the rate of clinical CPE rather than surveillance culture reports.
Introduction
Since the beginning of the millennium, carbapenemase-producing Enterobacterales (CPE) have become a major problem in health care systems worldwide. In Israel, a nationwide outbreak of CPE emerged in 2006, which was caused primarily by KPC-producing Klebsiella pneumoniae (KPC-KP) clonal complex (CC)-258.1,2 An essential part of the intervention that had led to the containment of the epidemic 1 has been the detection and isolation of carriers, by the widespread use of rectal surveillance cultures. This policy had since been recommended in other countries as well. 3
In recent years, new types of CPE, including VIM-, NDM-, and OXA-48-producing Enterobacterales, have disseminated into countries where the CC-258 KPC-KP were previously dominant, for example, Israel 4 or the United States. 5 Thus, surveillance culture (SC) media that were adequate for the detection of the CC-258 KPC-KP clone, which is characterized by high carbapenem minimal inhibitory concentration, 6 may no longer be sufficiently sensitive. 7 Due to this concern, we evaluated at the Tel-Aviv Sourasky Medical Center (TASMC) the analytic performance of a new SC media, the CHROMagar™ mSuperCARBA™. We found that the CHROMagar mSuperCARBA was more sensitive in detecting CPE isolates (83%) compared with “older” SC media such as the CHROMagar KPC (65%) and MacConkey agar with Imipenem (69%). 7
Consequently, in August 2017 we replaced the SC media to the CHROMagar mSuperCARBA media, and subsequently, we have witnessed a dramatic increase in the rate of CPE. Therefore, the initial objectives of the study were to analyze the effect of changes in SC media on the institutional rates of SC CPE, including their molecular and microbiological characteristics in a comparative multicenter study. In addition, we examined the interplay between the CPE rates as reported from surveillance versus clinical cultures and the differential effects of each of these parameters on the institutional rate of CPE.
Materials and Methods
Study design and settings
The study was a retrospective multicenter survey of the CPE rates in four general hospitals in Israel in relation to their use of different SC media. We aimed to analyze the CPE rates in hospitals before and after SC media were replaced versus hospitals where the SC media were not changed during the same period. In the first center, TASMC, the survey included two 1-year periods, before and after the replacement of the SC media in August 2017 (Table 1). TASMC is a 1,500-bed, tertiary care center in Tel-Aviv, Israel. The CPE rates in TASMC were first compared to two institutions where the SC media remained unchanged during the same time period (August 2016–July 2018): (1) the Rambam Medical Center (RMC), a 940-bed tertiary care center in Haifa (Northern Israel), and (2) Hillel-Yaffe Medical Center (HYMC), a 500-bed general hospital in the city of Hadera, located ∼45 km between Tel-Aviv and Haifa.
Clinical and Surveillance Culture Institutional Rates of Carbapenemase-Producing Enterobacterales
BMC, Beilinson Medical Center; CPE, carbapenemase-producing Enterobacterales; NA, not assessed; TASMC, Tel-Aviv Sourasky Medical Center.
Since SC media were not replaced in any other hospital in Israel during the same time period, we included additional center (the Beilinson Medical Center, BMC) where the SC media were replaced in August 2016, and therefore, the period studied was August 2015–July 2017. BMC is a 1,300-bed tertiary care center located in Petah-Tikva, 12 km east to Tel-Aviv.
Microbiological methods and CPE surveillance policy
The SC media used in the four institutions throughout the study are presented in Table 1. The TASMC laboratory was the only one in the country that had used the MacConkey with imipenem 1 mg/L media, 8 before August 2017. CHROMagar KPC and mSuperCARBA media were produced under license by a local manufacturer (Hylabs, Rehovot, Israel).
The microbiological processing of rectal SC for CPE in all centers was determined by specific instructions of the Israeli Ministry of Health 9 that included the analysis of every suspicious colony grown on SC media by PCR assays for the following genes: blaKPC, blaNDM, blaOXA-48, and blaVIM. The PCR assays were performed by the Xpert® Carba-R assay (Cepheid, Sunnyvale, CA) in the HYMC and BMC laboratories or by in-house assays at the TASMC 10 and RMC 11 laboratories. Bacterial identification was done by MALDI-ToF, using either the VITEK-MS® (BioMérieux, Marcy-l'Étoile, France) at TASMC or the Biotyper® system (Bruker Corporation, Billerica, MA) at all other centers. Growth of nonfermenting organisms was not reported.
The policies for the selection of patients for CPE screening by rectal SC were determined by the same guidelines. 9 Briefly, SC were collected in patients following either (1) a recent contact with another CPE carrier (postcontact surveillance) or (2) in patients admitted from suspected endemic environment, such as those admitted from other institutions (admission surveillance). The implementation of these guidelines is continuously monitored by the Ministry of Health,9,12 as are all new cases of CPE.
Data collection and statistical analysis
Data about CPE cultures from each center were extracted from the local laboratory information system by the corresponding laboratory director and were delivered anonymized to author AA. Both postcontact and admission SC were included in the analysis. The rates of CPE were calculated using either the total number of hospitalization days or the total number of SC performed as denominators, to reflect both the institutional burden of CPE and the efficacy of the surveillance process, respectively. The rates were compared between the periods at the same institution by the z-score test using the online OpenEpi software. 13
Trend analysis was done using the Joinpoint Regression Program version 4.0.0.014 and included the following analyses: (1) overall trend (in ln transformation) expressed as average percent change (APC) and joinpoint identification (i.e., identification of points of trend change); (2) trend analysis with “jump model” set at the 13th month (i.e., the replacement of SC media at TASMC and BMC), to determine whether the overall trend was affected by the SC media change; and (3) pairwise comparison of all four centers (six comparisons in total) to determine whether the trends were parallel in each center compared to the other three centers. 15
The (1-specificity) value was calculated as the number of SC with suspicious growth that were either negative by blaKPC, blaNDM, blaOXA-48, and blaVIM PCR (see above) or identified as nonfermenting bacteria, using either the total number of samples with suspicious colonies (both PCR-negative and PCR-positive samples) or the number of hospitalization days as denominator. The specificity of the SC media was calculated for CPE only, since the defined target for SC in Israel is CPE only, that is, excluding noncarbapenemase–producing carbapenem resistant Enterobacterales (NCP-CRE). 9
Results
The effect of change in surveillance culture media on the institutional burden of CPE in TASMC and BMC
Following the change in the SC media in August 2017, there has been an increase in the rate of SC CPE that continued throughout the following year (Table 1 and Fig. 1a). The overall trend had zero joinpoints and a positive APC of 5.69 (p < 0.05) that became not significant in the jump model (Fig. 1b). The increase in SC CPE in the second period was marked by an increase in the rates of NDM-CPE and OXA-48-CPE (7.58 fold and 3 fold, respectively) and in CPE species other than K. pneumoniae (Fig. 1a and Supplementary Table S1). Consequently, the rates of SC NDM-CPE and Escherichia coli CPE became higher in the second period compared with KPC-CPE and K. pneumoniae CPE, respectively. In contrast, the total rate of clinical CPE declined by 46% (Fig. 1a and Table 1), mostly due to a decline in KPC-CPE and K. pneumoniae CPE (Table 2), without an increase in the rate of clinical NDM-CPE.
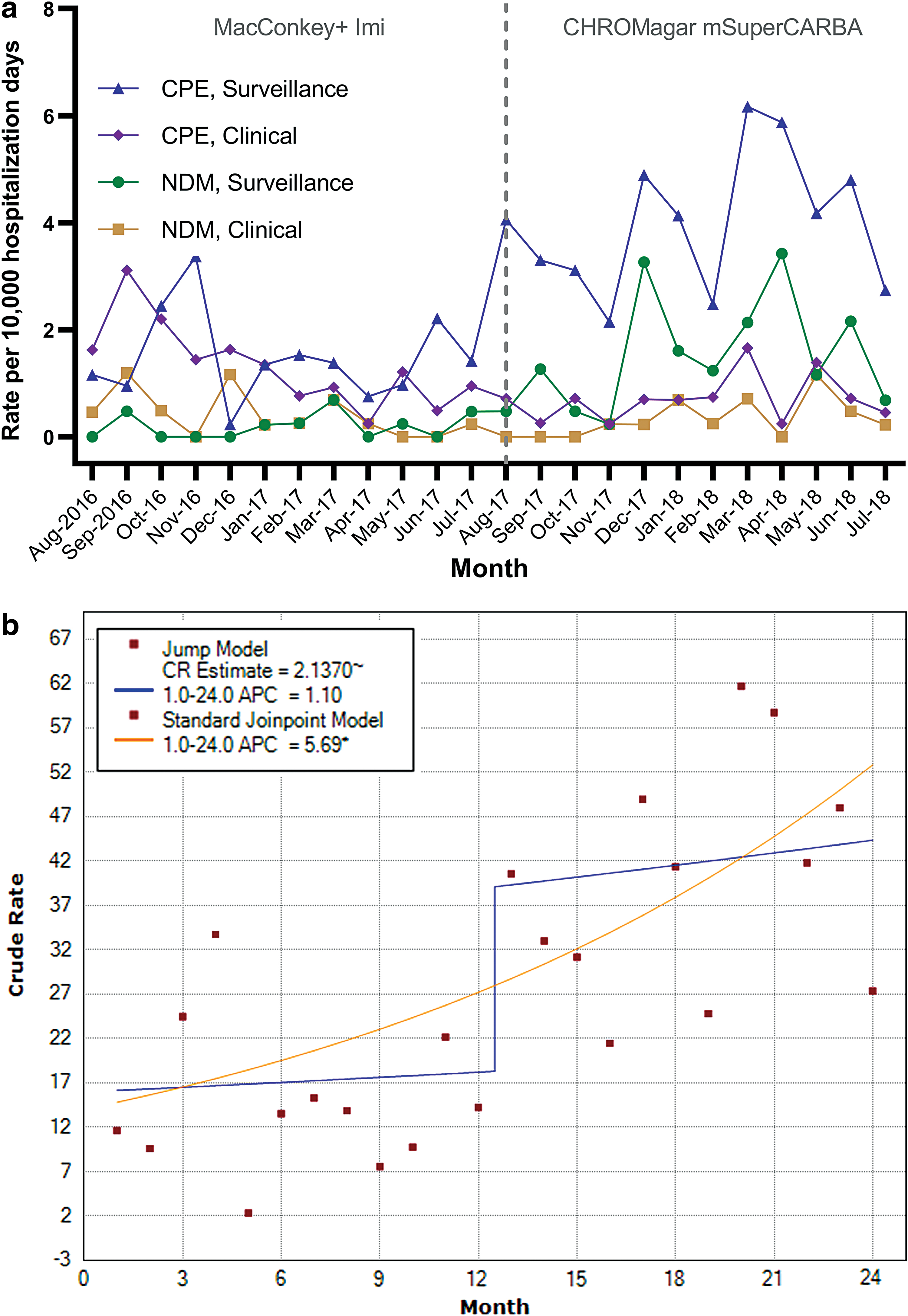
Institutional rates of CPE in TASMC.
Institutional Rates of PCR-Negative Surveillance Culture Isolates and Specificity for the Detection of Carbapenemase-Producing Enterobacterales
PCR was done for the following genes: blaKPC, blaNDM, blaOXA-48, and blaVIM.
Similar to TASMC, the period that followed the change in SC media in BMC (August 2016 onward) was marked by an increase in the rate of SC CPE (Table 1 and Fig. 2). The overall trend had zero joinpoints and a positive APC of 5.67 (p < 0.05) that became not significant in the jump model (Supplementary Fig. S1). The increase in SC CPE was mostly due to KPC-CPE of various species. Unlike TASMC, the rates of NDM- or OXA-48 CPE did not change (Supplementary Table S1). Although the rate of clinical CPE increased as well, the magnitude of the change was smaller compared to the change in the rate of SC CPE (1.93 vs. 2.67, respectively). In pairwise comparison, the trend in BMC was parallel to the trend in TASMC (Supplementary Fig. S2).
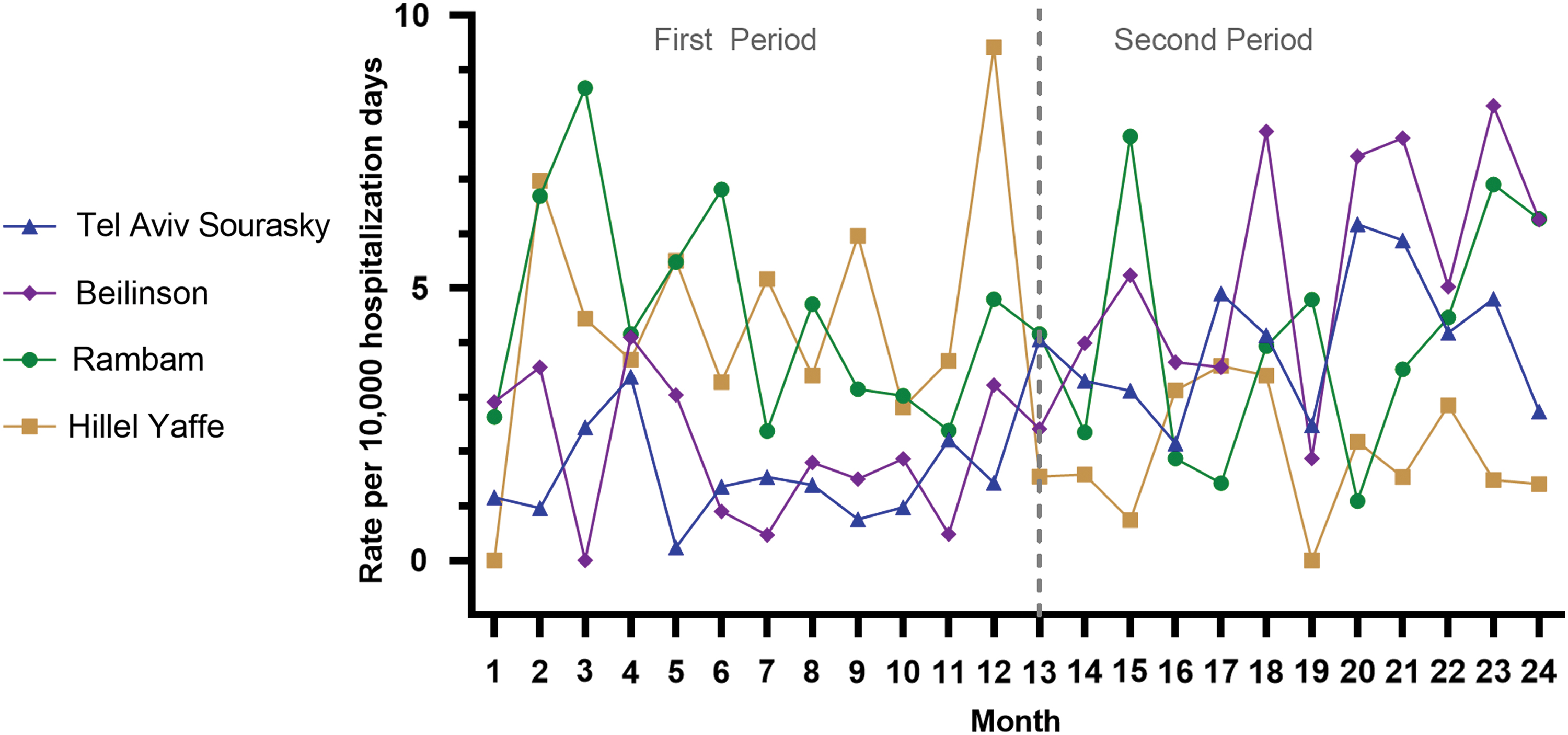
Institutional rates of total surveillance culture CPE at the four institutions. The dates of reporting were August 2016 until July 2018 (TASMC, RMC, and HYMC) or August 2015 until July 2017 in BMC. BMC, Beilinson Medical Center; HYMC, Hillel-Yaffe Medical Center; RMC, Rambam Medical Center. Color images are available online.
Lack of an increase in the rates of SC-CPE in other Israeli hospitals
To compare the epidemiology of CPE in the same periods, we examined the data obtained from two hospitals that had not changed their SC media during that period. In RMC there were no changes in the overall trend (APC = −0.72, p > 0.05) and between the periods in SC or clinical CPE (Fig. 2 and Table 1). The rate of SC KPC-CPE declined, while the rate of SC NDM-CPE increased in the second period, although the SC NDM-CPE rate was still lower (3.6 fold) compared with rate of SC KPC-CPE (Table 2).
In HYMC, the overall rate of SC CPE declined (Fig. 2) with zero joinpoints and an APC of −4.26 (p < 0.05). The decline in SC CPE was mainly due to a decline in SC KPC CPE, with a reduction in the rates of both K. pneumoniae and E. coli CPE (Table 2).
In pairwise comparison, RMC and HYMC had parallel trend, and both were nonparallel with the trends in either BMC or TASMC (Supplementary Fig. S2).
Specificity of the surveillance culture media in the four institutions
The specificity values for the detection of CPE for all SC media were very high (97%) and varied slightly between the periods in a manner similar to the variations in the rates of PCR-negative isolates (see below and in Table 2).
In RMC and HYMC, where the CHROMagar KPC media was used throughout the study, the rate of PCR-negative isolates remained relatively stable (Table 2). The rate of PCR-negative isolates per 1000 SC declined in HYMC in the second period, in parallel with the decline in SC CPE and the increase in the number of SCs performed (Table 1).
The change in SC media to CHROMagar mSuperCARBA had led to different effects on the SC specificity in TASMC and BMC. In TASMC, where the transition was from MacConkey agar with Imipenem, the rate of PCR-negative isolates per 1000 SCs did not change, and the rate out of all PCR-tested isolates declined, likely as a result of the increased rate of PCR-positive isolates (i.e., CPE). In BMC, where the transition was from CHROMagar KPC, the rate of PCR-negative isolates increased more than fivefold, and the rate out of all PCR-tested isolates increased from about 52% to 70%. The rate of PCR-negative isolates per 1000 SCs tested from CHROMagar mSuperCARBA was twice higher in BMC compared with TASMC.
Discussion
An integral part of the Israeli national intervention program aimed to contain the spread of CPE has been the establishment of national surveillance system in 2007. 1 Since then, similar surveillance programs have been enacted in various countries. 16 The monitoring of CPE in Israel includes reports from both clinical and surveillance cultures, and since CPE are more commonly detected in SC than in clinical cultures, 12 the institutional burden of CPE is determined mainly by positive SC CPE in asymptomatic patients. Hence, changes in the SC methodology may have profound effect on the reported CPE rates even without actual, significant epidemiological change in the institution. An increasing number of positive SC CPE may in turn lead to changes in surveillance policies (e.g., increase in the number of SC performed)12,17 and thus amplifying even further the rate of SC CPE, as was actually seen in TASMC.
In a previous study, the CHROMagar mSuperCARBA media exhibited better analytical sensitivity 7 compared with the CHROMagar KPC and the MacConkey agar with Imipenem media, which were used in the first period of the current study by BMC and TASMC, respectively. The CHROMagar mSuperCARBA media were also more sensitive compared with the CHROMID® Carba media (bioMérieux, France) (97% vs. 90.9%, respectively). 18 In our study, we have seen a dramatic increase in the rate of SC CPE in TASMC and BMC following the change to the CHROMagar mSuperCARBA media in the second period.
In contrast, the rate of SC CPE remained the same or even declined during the same time period in the two hospitals that continued to use the CHROMagar KPC media (RMC and HYMC, respectively). These differences in the trend of SC CPE between the institutions (Table 1 and Supplementary Fig. S2) along with the disappearance of the upward trend in the jump model in TASMC and BMC (Fig. 1b and Supplementary Fig. S1) support the hypothesis that the changes in TASMC and BMC were caused to a great extent by the change in the diagnostic method (i.e., the SC media).
Diagnostic modifications may lead to significant alterations in the reported incidence of various infections, as was reported in Clostridium difficile 19 and Pertussis infections. 20 An important shortcoming of such studies is that it is difficult to assess the differential effect of the diagnostic modifications from those caused by “true” epidemiological changes. Thus, the inclusion of an additional marker that is not influenced by the diagnostic modifications is important.
In our study, we have shown that the use of clinical CPE as the primary marker for CPE surveillance can overcome the significant biases that can emerge when SC CPE are the main components of the surveillance, irrespective of the benefits of the use of CPE SC for the identification and isolation of carriers. 12 Since the most important target for prevention is clinical infection and not asymptomatic carriage, focusing the institutional efforts on the former can be more beneficial for patient's care. Indeed, the rate of clinical CPE had actually declined in TASMC, despite the increase in SC CPE following the change in SC media. In BMC, the increase in the rate of clinical CPE was smaller compared to the change in SC CPE (Table 1 and Fig. 2).
A puzzling phenomenon that was observed in TASMC was the change in the relative rates of different types of CPEs, including different carbapenemase mechanisms (an increase in NDM- and OXA-48 CPE) and bacterial species (an increase in species other than K. pneumoniae). Previous studies have shown that SC media differ in their analytical performances and that these differences might be more substantial in specific types of CPE (especially OXA-48 CPE) that are more challenging for detection.7,21 Thus, seemingly small differences in analytical sensitivity of new SC media may lead to “unearthing effect” and reveal a high prevalence of previously unnoticed CPE. Considering the stable low rate of clinical CPE during the second period in TASMC (including NDM- and OXA-48 CPE), we believe that this change in the relative rates of different CPE in TASMC was also mainly a result of the change in SC media.
A potential drawback of the increased sensitivity of the SC media is diminished specificity. Since identification of CPE was confirmed by the performance of PCR for carbapenemase genes in all suspicious colonies, 9 the main problem was not the reporting of false-positive result but the unnecessary spending of resources (PCR reagents and work) in these cases. Indeed, the majority of tests were actually performed on non-CPE colonies in all four centers (Table 2), but the rates of non-CPE tested differed between the institutions. The rates were especially low in BMC compared to the rates in RMC and HYMC that were using the same media (CHROMagar KPC), but increased dramatically after the media was changed to CHROMagar mSuperCARBA (from 4.15 to 21.43 per 1000 cultures, respectively). In contrast, the rates of PCR-negative tests in TASMC were much lower when using CHROMagar mSuperCARBA (10.01 per 1000 cultures) and had actually declined from 76% to 59% of the total number of PCRs performed (Table 2).
Although these differences might be related to difference in the rates of colonization by NCP-CRE in the different centers, it can also be a reflection of different testing practices between the institutions. Considering the high cost of these tests (40$ and more per test), the total cost spent merely on testing non-CPE colonies can easily reach between 16,000$ and 20,000$ per year. Such high costs that are “wasted” on negative results may deter clinical laboratories from switching to more sensitive SC media. Thus, aiming to maximal sensitivity of SC media is not a sufficient goal, and improved specificity must be taken into account in the design of new SC media.
The main limitation of our study is that the effect of the change in SC media was analyzed within TASMC and BMC by comparing two periods and not by parallel testing of the two SC media throughout the study. Although parallel testing of different SC media was used in our past studies, 8 due to the current high number of CPE SC (>28,000 per year) and their very low positivity rate (∼0.5%, Table 1), this design had become impractical and is not commonly used by recent studies.7,22,23 To tackle this problem, we applied statistical methods (such as the “jump model”) and used a comparison to other institutions. Moreover, to “neutralize” the possible effect of epidemiological changes, we used the rate of clinical CPE as a surrogate for the institutional burden of CPE that is independent of methodological changes.
In conclusion, our study shows that changes in SC media may lead to significant changes in the rate of SC CPE that might be irrespective of actual epidemiological changes. Therefore, the surveillance of institutional burden of CPE and the assessment of intervention results should be based primarily on the rate of clinical rather than SC CPE reports.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.