
Abstract
This study was conducted to determine the molecular epidemiology of blaKPC-encoding Klebsiella pneumoniae recovered from three public hospitals in Brazil. Molecular investigation of blaOXA-48, blaKPC, blaNDM, blaCTX-M, blaSHV, blaTEM, blaIMP, and blaVIM resistance genes was performed in 99 K. pneumoniae isolates from inpatients of intensive care units. Antimicrobial susceptibility was determined with a Vitek-2 System, except for polymyxin B, which was evaluated by the microbroth dilution test. Clonal relatedness was established by pulsed-field gel electrophoresis and multilocus sequence typing. Screening resistance genes showed that K. pneumoniae isolates carried the blaKPC (88.9%), blaSHV (73.5%), blaTEM (72.2%), and blaCTX-M (43.9%) genes. The most frequent sequence types (STs) were ST273, ST11, ST 1298, ST13, ST2687, and ST37. We report new STs in K. pneumoniae that have not been detected previously in Brazil. K. pneumoniae belonging to the same clone is present in different hospitals in the same region, showing the spread of multidrug-resistant K. pneumoniae.
Introduction
The emergence of infections caused by carbapenem-resistant Klebsiella pneumoniae (CR-KP), mainly in patients in intensive care units (ICUs), is a global concern. The transmissibility and limited therapeutic options for treating these infections make it difficult to control this multiresistant pathogen. In Brazil, K. pneumoniae carbapenemase (KPC) is the most predominant carbapenemase in Enterobacteriaceae. 1 The rapid spread of KPC-producing K. pneumoniae (KP-KPC) worldwide appears to be related to the dominant sequence types ST258 and ST11 that belong to CC258 clonal complex. 2 Previous studies showed that specific plasmids are successfully spreading and harbor resistance among K. pneumoniae strains in Brazilian hospitals. 1 Determining the resistance genotypes can reduce delays in administering adequate therapy and may decrease the high mortality of infectious KP-KPC. 2
The aim of study was to determine the molecular epidemiology of blaKPC-encoding Klebsiella pneumonia recovered from three public hospitals in the Midwestern region of Brazil, which have not been widely examined.
Materials and Methods
Human subject protection
This study was approved by the ethics committee of Federal University of Mato Grosso do Sul (CAAE—50087815.2.0000.0021).
Bacterial identification and susceptibility test
In this study, we selected 99 nonduplicate isolates of CR-KP obtained between March 2013 and March 2014 from patients in ICUs at 3 Brazilian public hospitals: Hospital A, Hospital B, and Hospital C of Mato Grosso do Sul state, which have 592, 352, and 271 beds, respectively.
The K. pneumoniae identification and antimicrobial susceptibility tests were performed with a Vitek 2 System (bioMérieux, Marcy L'Etoile, France). Antimicrobial susceptibility tests to determine the minimal inhibitory concentrations (MICs) of polymyxin B were performed by the broth microdilution technique using polystyrene plates and polymyxin B sulfate (Eurofarma, São Paulo, Brazil) and interpreted according to BrCast guidelines (S ≤ 2 mg/L). 3 Escherichia coli ATCC 25922 and Pseudomonas aeruginosa ATCC 27853 were used as quality control strains. E-test (bioMérieux) strips were used to determine the MICs of tigecycline. The results were interpreted according to the U.S. Food and Drug Administration—FDA (≤2.0 mg/L, susceptible; 4.0 mg/L, intermediate; and ≥8.0 mg/L, resistant).
Multidrug resistant (MDR) was defined as nonsusceptibility to at least one agent in three or more antimicrobial categories, whereas extensively drug resistant (XDR) was defined as nonsusceptibility to at least one agent in all, but two or fewer antimicrobial categories. 4 The agents used to define these categories were aminoglycosides (amikacin and gentamicin), piperacillin-tazobactam, carbapenems (imipenem, meropenem, and ertapenem), cephalosporins (cefazolin, ceftriaxone, and cefepime), cephamycin (cefoxitin), fluoroquinolones (ciprofloxacin), glycylcyclines (tigecycline), and polymyxin B.
Molecular detection of antimicrobial resistance genes and clonal relationship
K. pneumoniae isolates were screened by polymerase chain reaction (PCR) with β-lactamase genes using conditions and primers previously described (Table 1).5–8 The equipment used to carry out the PCR technique was Thermal cycler T100 (Bio-Rad, Hercules, CA).
Primers Used to Identify Genes Encoding Beta-Lactamases Using the Polymerase Chain Reaction Technique and Respective References
CTX-M, cefotaximase; IMP, imipenemase; KPC, Klebsiella pneumoniae carbapenemase; NDM, New-Delhi metallo-betalactamase; OXA, oxacillinase; SHV, sulfhydryl variable β-lactamase; TEM, temoniera β-lactamase; VIM, Verona imipenemase.
The clonal relationship between K. pneumoniae isolates was investigated by pulsed-field gel electrophoresis using the XbaI restriction endonuclease (Promega, Madison, WI) in the CHEF-DR III apparatus from Bio-Rad Laboratories (Hercules, CA) and analyzed with BioNumerics fingerprinting software (Applied Maths, Sint-Martens-Latem, Belgium). 9 Multilocus sequence typing was performed to subtype CR-KP by amplification and sequencing of seven housekeeping genes, including gapA, infB, mdh, pgi, phoE, rpoB, and tonB. 10 The allelic profiles and STs were determined using the Institute Pasteur Klebsiella multilocus sequence typing (MLST) database.
Results
The 99 CR-KP isolates were obtained from the urine (42.4%), tracheal aspirates (22.2%), blood (16.2%), catheter tips (7.1%), surgical wound exudates (8.1%), and other (4.0%) clinical specimens. Antimicrobial susceptibility tests showed high rates (>85%) of resistance to β-lactams, quinolones, and gentamicin antibiotics. Twelve (12.1%) K. pneumoniae isolates were considered XDR and 87 (87.9%) were MDR. Seventy-six (76.8%) isolates were resistant to all carbapenems. A lower percentage of resistance was observed against amikacin (5.1%), polymyxin (18.2%), and tigecycline (20.2%).
Screening for antimicrobial resistance genes showed that 88.9% of CR-KP isolates carried blaKPC, but blaOXA-48, blaNDM, blaVIM, and blaIMP were not detected. Extended-spectrum beta-lactamase (ESBL) genes were detected in most isolates: blaSHV (73.5%), blaTEM (72.2%), and blaCTX-M (43.9%). Fifty-four (54.5%) CR-KP isolates contained these three ESBL genes.
The molecular characterization of the 99 K. pneumoniae included in the study was done using the techniques of pulsed-field gel electrophoresis (PFGE) and MLST. Of 38 distinct profiles identified using the PFGE technique, 8 identical profiles were observed in 2 hospitals (Fig. 1).
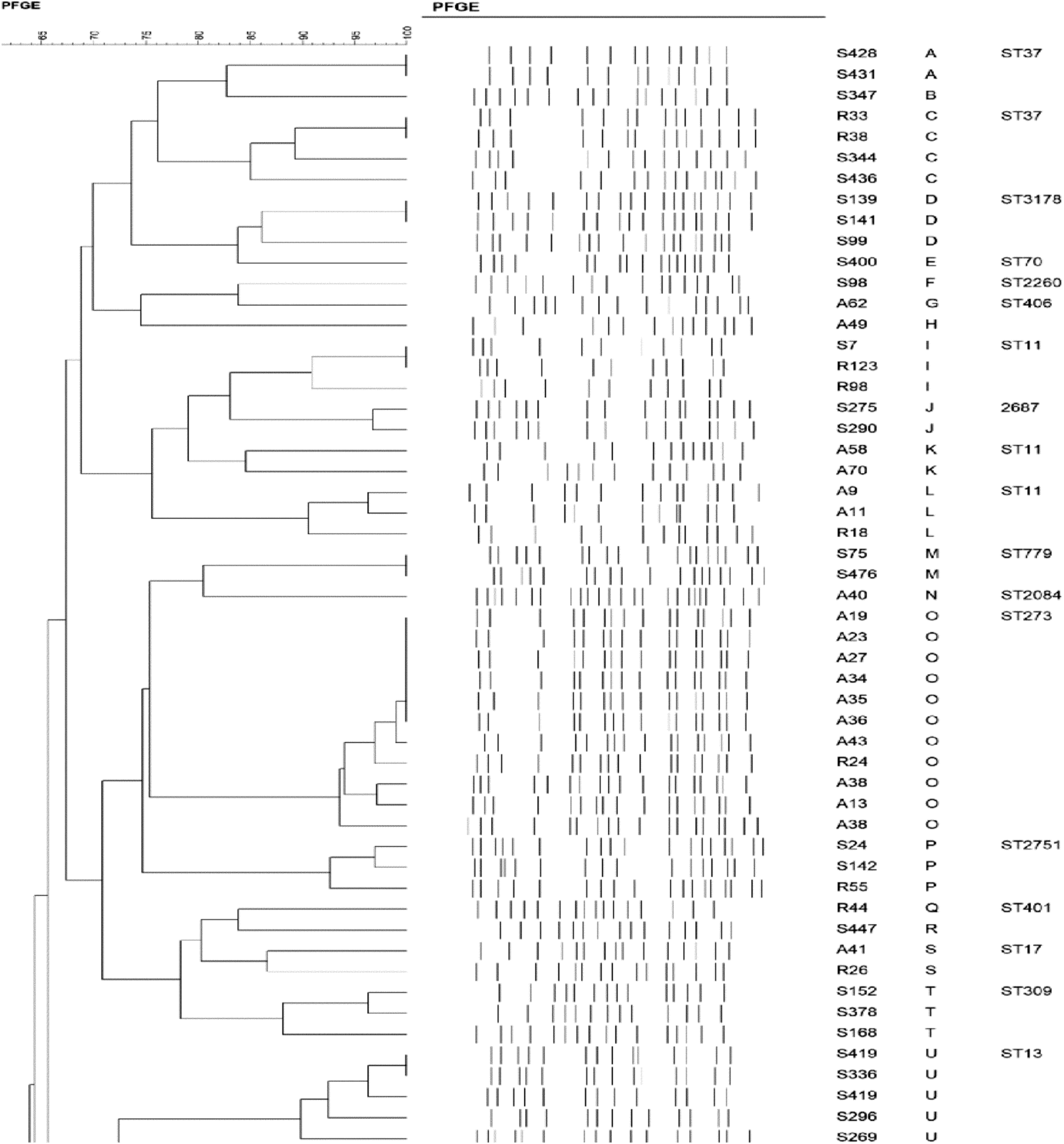
Molecular typing of 99 pulsotypes from carbapenem-resistant Klebsiella pneumoniae isolated in Mato Grosso do Sul, Brazil.
Table 2 presents antimicrobial susceptibility and resistance genes of the most frequent STs: ST273 (13, 13.1%), ST11 (11, 11.1%), ST1298 (10, 10.1%), ST13 (8, 8.1%), ST2687 (7, 7.1%), and ST37 (6, 6.1%). The most prevalent STs in each hospital were ST1298, ST273, and ST13 in Hospital A, B, and C, respectively. ST11 was detected in all hospitals studied (Fig. 2). Other ST types detected were ST309 (n = 4), ST304, ST2751 and ST3178 (n = 3), ST17 (n = 2), ST323 and ST779 (n = 2), ST70, ST401, ST406, ST1075, ST2084, and ST2260 (n = 1).
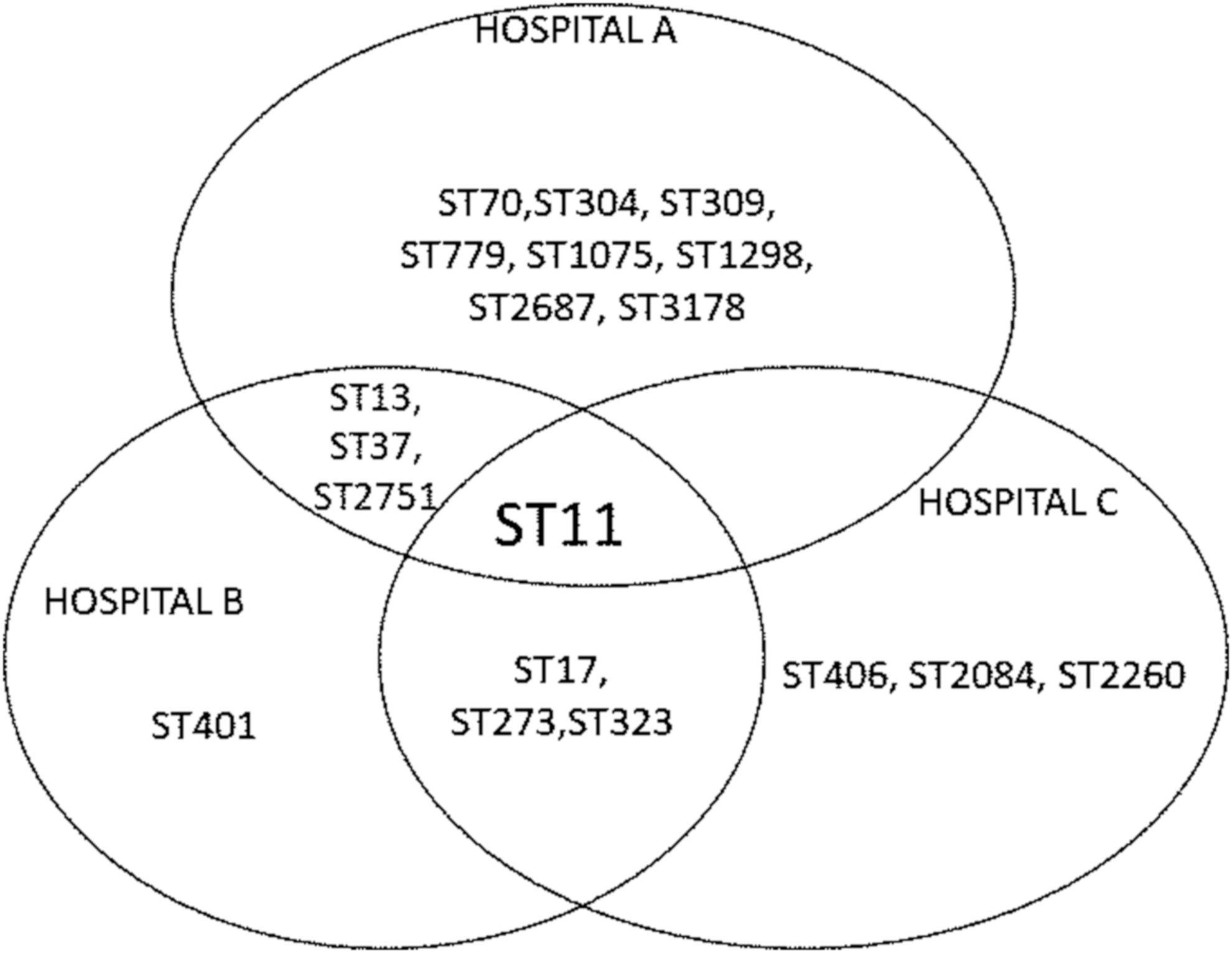
Distribution of the most common Klebsiella pneumoniae STs in three hospitals of Mato Grosso do Sul state, Brazil. STs, sequence types.
Sequence Types, Antimicrobial Resistance and Resistance Genes of Klebsiella pneumoniae According to Hospital of Origin
AMI, amikacin; CIP, ciprofloxacin; ERT, ertapenem; IPM, imipenem; MER, meropenem; POL B, polymyxin B; ST, sequence type; STNI, ST not identified; TIG, tigecycline.
Discussion
In ICUs, CR-KP is a major infectious agent in the urinary tract, lower respiratory tract, bloodstream, and surgical wound infection.1,11 In addition to the high resistance to carbapenem antibiotics, K. pneumoniae recovered from patients in ICUs were resistant to most antibiotics recommended for treatment. Similar to the results of a previous study, 12 tigecycline and polymyxin were among the drugs showing lower resistance and may be considered therapeutic options for treating infections caused by MDR K. pneumoniae.
Although K. pneumoniae shows good sensitivity to tigecycline, the emergence of tigecycline resistance in blaKPC-2 has been reported. 13 A study conducted to evaluate K. pneumoniae in different regions of Brazil 14 reported resistance rates of 38.1% to tigecycline. According to Perez et al., 12 tigecycline combined with other antimicrobial agents is effective for treating infections caused by KPC- and OXA-48-producing K. pneumoniae. The profile of antibiotic resistance varies by region and even between hospitals in the same city. Thus, determining the resistance profile of different hospitals is essential for guiding therapeutic choices. This is the first description of resistance to tigecycline and polymyxin in Mato Grosso do Sul state. These results should expand the knowledge of K. pneumoniae antimicrobial resistance in Brazil.
Polymyxin has been considered “last-line” treatment for MDR Gram-negative infections worldwide. 12 Increased polymyxin resistance rates have been observed in recent years in Brazil. 15 In this study, 18.2% (18/99) CR-KP isolates were polymyxin B resistant. The mechanisms involved with polymyxin resistance in these CR-KP samples were previously reported. 16
KPC-producing K. pneumoniae is prevalent in North America, Greece, Italy, Taiwan, Colombia, China, Argentina, and Brazil. 2 Our data show that KPC production is the main mechanism of resistance in K. pneumoniae isolated in ICUs in public hospitals in Mato Grosso do Sul state. The high rates of resistance to β-lactams and other antimicrobial classes are likely related to the concomitant presence of different resistance mechanisms.
Study with the multilocus sequence typing shows that ST258 and ST11 STs are the globally prevalent clones in K. pneumoniae. 2 These STs belong to the clonal complex CC258, which has spread rapidly worldwide. ST273, ST11, and ST17 belong to the clonal complexes CC147, CC258, and CC17, respectively. Further studies are needed to establish whether the STs found in our research are groups of closely related strains.
According to previous studies, ST258 is prevalent European countries and the United States and ST11 (a single-locus variant of ST258) is more prevalent in Asia, 2 and has also been reported in Latin America.1,2
In many regions of Brazil, there are no data on clonal complexes associated with resistance to carbapenems among Enterobacteriaceae species. 17 In Brazil, ST11, ST340, and ST437 are the most frequent patterns reported in KPC-2-producing K. pneumoniae.1,15,17 Interestingly, in our study, most of CR-KP isolates were characterized as ST273, ST11, and ST1298, whereas ST258, ST512 and ST437 (single-locus variants of ST258), and ST340 were not detected. These results show that these STs may vary according to the geographical region.
Unlike that observed in Asia,18,19 in our study, ST273 was not related to K. pneumoniae carrying blaNDM gene. However, we detected one colistin-resistant K. pneumoniae ST273, as previously described in Italy. 20
In our study, CR-KP of ST273 harbored blaSHV and blaTEM (100%), blaKPC (91.7%), and blaCTX-M (36.4%) genes. Most CR-KP isolates belonging to ST273 showed sensitivity to tigecycline and polymyxin B. One ST273 CR-KP strain was polymyxin resistant (MIC = 8 mg/L), whereas no resistance to tigecycline or amikacin was recorded.
ST11, the most prevalent ST in this study, is among the most frequently described STs in Brazil.1,17 It has been reported in several countries of Latin America, Asia, beyond India, the United Kingdom, Turkey, Spain, and Sweden. 2 According to a previous study, ST11 may be related to colistin resistance in K. pneumoniae. 21 In our study, 4 out of 18 CR-KP resistant to polymyxin (MIC ≥32 mg/L) belonged to ST111. The ability of K. pneumoniae ST11 to acquire resistance and its virulence power determine its prevalence in this profile and success of infection. 22
Recently, we reported ST1298 in polymyxin-resistant K. pneumoniae. 16 In this study, 10 K. pneumoniae of ST1298 were found in Hospital A. In our study, ST1298 CR-KP presented a higher rate of tigecycline resistance compared to the other STs.
ST13 was described in previous studies with K. pneumoniae carrying blaTEM 23 and blaOXA-4824 in Europe and was reported in KPC-producing K. pneumoniae from northeastern and southeastern Brazil. 14 Corroborating these results, our study showed a high prevalence of KPC-producing K. pneumoniae of ST13 in the studied hospitals. We found that ST11 and ST13 were related to high rates of polymyxin resistance. The selective pressure caused by polymyxins likely contributed to selection of this resistance and limited its treatment.
ST37 has been described in K. pneumoniae β-lactamases producing KPC, New-Delhi metallo-betalactamase (NDM), and IMP-4 in China,25–27 the OXA-48 in Saudi Arabia, 28 ESBL in Africa, 29 and KPC in Brazil. 21 In our study, this clone harbors blaSHV, blaTEM, blaCTX-M, and blaKPC genes.
This study describes for the first time in Brazil the STs ST304, ST309, ST401, ST406, ST779, and ST251 in MDR K. pneumoniae. Further studies are needed to determine the relationship of these STs with antimicrobial resistance.
The results obtained reveal dissemination of K. pneumoniae belonging to the same clone in different hospitals in the same region. The transfer of blaKPC, blaTEM, and blaCTX-M genes likely contributed to the high rate of carbapenem resistance observed in MDR K. pneumoniae isolates.
Conclusions
K. pneumoniae belonging to the same clone is present in different hospitals in the same region. New STs were described in carbapenem-resistant K. pneumoniae in Brazil. Transfer of blaKPC, blaSHV, blaTEM, and blaCTX-M genes has contributed to the high rate of carbapenem resistance observed in MDR K. pneumoniae isolates.
Footnotes
Acknowledgments
We thank the staff of the hospital microbiology laboratories, particularly Caroline Conci Campos, Nádia Cristina Pereira Carvalho, Fernando Aguilar Lopes, Carolina Tieppo, and Sidiane Ferreira do Carmo, for providing the K. pneumoniae strains. We would like to thank Isadora Rezende and Yanara Miranda Ferreira for helping with the laboratorial tests.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was financed, in part, by Coordenação de Aperfeiçoamento de Pessoal de Nível Superior—Brazil (CAPES)—Finance code 001 and by Universidade Federal de Mato Grosso do Sul and by Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq), Instituto Oswaldo Cruz (IOC)—Fiocruz.