
Abstract
Background:
The purpose of this cross-sectional study was to examine the impact of below-average cardiovascular fitness and inactivity on the metabolic syndrome among an understudied population—undergraduate men and women, ages 18–24 years.
Methods:
Between January, 2010, and May, 2012, we assessed anthropometric, biochemical, and clinical measures in a convenience sample of students (n=1610) enrolled in an introductory nutrition course at a public university. We quantified the prevalence of metabolic syndrome criteria, estimated cardiovascular fitness via a 1-mile Rockport Walk Test, and evaluated daily activity via pedometer. Subjects were classified as below-average, average, and above-average fitness based upon the Rockport Walk Test; activity levels were classified as low active, somewhat active, active, or highly active according to average steps per day.
Results:
Those with below-average fitness (10%) were at increased risk for being overfat, having abdominal obesity, and having the metabolic syndrome as compared to those with average or above-average fitness (odds ratio: 12.4, 10.0, and 4.7, respectively; all P<0.01). Twenty percent of subjects were low active (<7500 steps/day) and had a greater number of metabolic syndrome criteria as compared to very active subjects (>12,500 steps/day) (0.94±0.05 vs. 0.73±0.05, P=0.01).
Conclusions:
Young, college-age adults with below-average cardiovascular fitness and/or low activity levels are at increased risk for obesity and the metabolic syndrome. Future studies should examine how promoting lifestyle habits that increase physical activity and reduce sedentary behaviors during the young adult years can improve metabolic health.
Introduction
The young adult years are filled with transitions and “firsts,” including securing full-time employment, co-habitation, and/or moving away from parents. Lifestyle choices and routines formed during these transitional years have the potential to positively and/or negatively impact long-term health. One of the critical lifestyle choices that can influence the incidence of metabolic syndrome is physical activity. According to the Spring 2011 American College Health Assessment, more than half of college adults report insufficient activity levels and 23% report no physical activity over the previous week. 3 Despite having >3.5 hours of leisure time per day, 4 college students report a number of barriers to participating in leisure-time activity, including perceived difficulty associated with physical exertion, lack of time, and lack of social support. 5 Increasing computer and technology usage appears to reduce time spent in other activities; inactive college students report significantly more screen time compared to active students. 6
Inactivity negatively impacts young adult health. Desai et al. found that physical inactivity is related to a higher body mass index (BMI) in over 4000 undergraduates. 7 Sachek et al. reported that high estimated cardiovascular fitness was associated with favorable lipid profiles and blood glucose levels among college students at a private, 4-year institution. 8 Previously, we observed in a group of over 2000 undergraduates that those with the highest level of self-reported physical activity had the lowest level of metabolic syndrome. 9 With more that 17 million “emerging adults” enrolled at one of the more than 4000 colleges and universities in the United States, 10,11 the campus environment is an ideal and convenient setting to examine young adult health. 12 Yet few studies have comprehensively studied physical activity, cardiovascular fitness, and chronic disease risk among college adults 13 despite evidence of this population's high rates of weight gain and declining rates of physical activity. 14
Therefore, the current study had two main purposes: First, to determine whether college students with below-average cardiovascular fitness, as determined by the Rockport 1-mile walk test, had greater criteria of metabolic syndrome; and second, to determine whether college students reporting the lowest level of activity, as determined by pedometer, had greater criteria of metabolic syndrome.
Methods
Between January, 2010, and May, 2012, a convenience sample of students between the ages of 18 and 24 years enrolled in an introductory nutrition course were recruited during the fall, spring, and summer academic terms for the ongoing, cross-sectional Young Adult Health Risk Screening Initiative at the University of New Hampshire (UNH). 15 All methods were in accordance with standards and protocols associated with the use of subjects in human research and approved by UNH's Institutional Review Board for the Protection of Human Subjects. Ninety-five percent (n=1834) of the students enrolled in the course (n=1952) provided written, informed consent at the start of the term. Of these participants, 4% (69) were excluded due to the age parameters of the study, and 8% (n=155) were excluded due to missing anthropometric, biochemical, clinical, or fitness measurements generally associated with absence or lack of compliance. Data were collected from a total of 1610 subjects (27% men, 73% women).
All anthropometric, biochemical, and clinical measures were performed in the morning after a 10- to 12-hr overnight fast with participants wearing T-shirts and shorts. Participants were instructed to avoid intense activity (≥4 hours) and alcohol (≥48 hours) before their self-scheduled appointment. Participants were also instructed to void immediately prior to measurements.
Anthropometric measures
Height and body mass were measured using calibrated equipment and after participants removed their shoes: Height (cm) was measured via a wall-mounted stadiometer (Accustat Genentech, San Francisco, CA) following standard protocols, and body mass (kg) was measured via digital scale (#2000A, Life Measurement Inc, Concord, CA). Waist circumference (cm) was measured via Gulick tape measure at the iliac crest following the protocol described by the National Health and Nutrition Examination Survey (NHANES). 16 Height, body mass, and waist measures were collected in duplicate and averaged. Body composition was assessed via bioelectrical impedance following manufacturer's instructions (Tanita, 300A); overfat was defined as ≥20% body fat for men, and ≥33% body fat for women. 17
Biochemical and clinical measures
Blood samples were obtained via fingerstick and immediately analyzed by a desktop analyzer (Cholestech LDX; Orlando, FL) for glucose, total cholesterol (TC), high-density lipoprotein cholesterol (HDL-C), and triglyceride (TG) concentrations, as described previously. 9 Low-density lipoprotein cholesterol (LDL-C) was calculated by the Friedewald equation. 18 Systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured in both arms via an automated cuff (HEM-711DLX; Omron, Bannockburn, Illinois) after the participant was seated and quiet for a minimum of 5 min; the two measures were averaged prior to analyses.
Metabolic syndrome measures
Metabolic syndrome and its five criteria (abdominal obesity, elevated TGs, low HDL-C, elevated blood pressure, and high fasting glucose) were classified according to the parameters established jointly by the American Heart Association and the National Heart, Lung and Blood Institute. 19 Participants who reported taking medication for hypertension (n=6) or hyperglycemia/diabetes (n=13) were classified as having elevated blood pressure or blood glucose, respectively. Participants were categorized as having zero, one, two, or three or more criteria; they were categorized as having metabolic syndrome if they had three or more of these criteria.
Physical activity and cardiovascular fitness measures
Activity was determined via self-recorded daily steps. Participants were provided a pedometer (SW-200 Digi-walker, New Lifestyles; Lees Summit, MO) and step log, instructed on the proper usage of the device, and asked to self-record their daily steps for 5 weekdays and 2 weekend days. Relative cardiovascular fitness [maximal oxygen uptake (VO2max) mL·kg−1·min−1] was estimated via a 1-mile Rockport Walk Test during a second self-scheduled appointment. 20 All subjects were instructed to walk as fast as they could for 1 mile on an indoor track. Immediately upon completion of the 1-mile walk, subjects reported their 10-sec heart rate obtained from the carotid artery. The 10-sec heart rate was then converted to beats per minute. VO2max mL·kg−1·min−1 was calculated using the predication equation established by Dolgener et al. for college students 21 :
[88.768+(8.892×Sex: 0=women, 1=men) – (0.0957×body mass in pounds)−(1.4537×finishing time in minutes)−(0.1194×60-sec heart rate)].
These estimated cardiovascular fitness levels were characterized as below average (<41.5 mL·kg−1·min for men;<34.1 mL·kg−1·min−1 for women), average (41.5–50.9 mL·kg−1·min−1 for men; 34.1–40.6 mL·kg−1·min for women), or above average (≥51.0 mL·kg−1·min for men; ≥40.7 mL·kg−1·min for women) as defined by George et al. 22
Data management and statistical analyses
All variables were checked for extreme outliers via boxplot analysis and violations of normality and, if necessary, removed (i.e., daily steps) or transformed (i.e., triglycerides) prior to statistical analyses, respectively. Actual data presented are untransformed and presented as frequencies or means±standard error (SE). Chi-squared tests for independence were used to evaluate prevalence differences. Mean differences were tested via analysis of covariance (ANCOVA) using the general linear model; gender served as a covariate. Group comparisons, using the estimated marginal means, were assessed by post hoc multiple comparison test with the use of the Bonferroni adjustment. Self-recorded daily steps were categorized into four groups (i.e., <7500, 7500–9999, 10,000–12,500, >12,500 steps/day) according to the indices proposed by Tudor-Locke and Bassett. 23 Logistic regression, adjusted for sex, was used to assess the impact of fitness level on different categorical risk factors (abdominal obesity, low HDL, high TGs, hypertension, elevated fasting glucose, overfat) and to calculate odds ratios (OR) and 95% confidence intervals (CIs), comparing those with below average measured VO2max with those in the average- or above-average VO2max. Significance was established as P<0.05. All statistical analyses were performed by SPSS v. 19.
Results
The sample was comprised of predominately white (95%) students within their first 2 years of college (88%). Twenty-seven percent of the sample was enrolled in an allied health or nutrition major, and the majority (91%) were nonsmokers. Approximately 72% of the participants had BMIs within a healthy range (18.5–24.9 kg·m2) and 23% of males and 18% of females were classified as overfat. The average predicted VO2max was 46.5 mL·kg−1·min−1 for men and 39.6 mL·kg−1·min for women (P<0.01) (Table 1). Nineteen percent of participants were classified as low active, 33% somewhat active, 25% active, and 23% highly active according to daily steps. Activity levels did not differ between men and women (P=0.64).
Data are presented as means±standard error (SE). Mean differences between men and women were analyzed via an independent samples t-test.
Ninety percent of the sample was classified as having average or above-average fitness. Participants with below-average fitness levels were taller, heavier, and had greater waist circumference, BMI, and body fat than those with average and above average fitness (Table 2; P<0.01). Additionally, those with below-average fitness had higher TC, LDLs, triaclyglycerides, glucose levels, and higher SBP and DBP than those with average and above-average fitness (Table 2; P<0.01). Participants with below-average fitness levels had fewer self-recorded daily steps as compared to the above average fitness group (9682±283 vs. 10,754±153, P<0.01) and also had 17% and 28% lower estimated VO2max levels than the participants with average and above average fitness, respectively (Table 2; P<0.01).
Data are presented as means±standard error (SE). Mean differences between levels of fitness were tested via analysis of covariance (ANCOVA) using the general linear model; gender served as a covariate.
Different lowercase superscript letters indicate significant differences between fitness levels. Triacylglycerides were log10 transformed for the normalization of the distribution prior to statistical analysis; untransformed means are presented.
HDL-C, high-density lipoprotein cholesterol; LDL, low-density lipoprotein cholesterol.
Sixty percent of the total sample had one or more criteria for metabolic syndrome, 21% had two or more, and 5% had the metabolic syndrome. More than three-quarters (77%) of subjects with below-average fitness levels had one or more criteria for metabolic syndrome, whereas 63% and 48% of those with average or above-average fitness had one or more criteria, respectively (Table 3). The most prevalent criterion for metabolic syndrome in the below-average fitness group was abdominal obesity, whereas low HDL-C and high blood pressure were the most common metabolic syndrome criteria in the average fitness and above-average fitness groups (Table 2). College students with below-average fitness were over 10 times more likely to have abdominal obesity and be overfat and nearly five times more likely to have the metabolic syndrome compared to students with average and above-average fitness (Table 4). The number of metabolic syndrome criteria also differed with activity level: Highly active students had fewer metabolic syndrome criteria as compared to somewhat active and low-active students (0.73±0.05 vs. 0.89±0.04 and 0.94±0.05, respectively; both P<0.05) (Fig. 1).
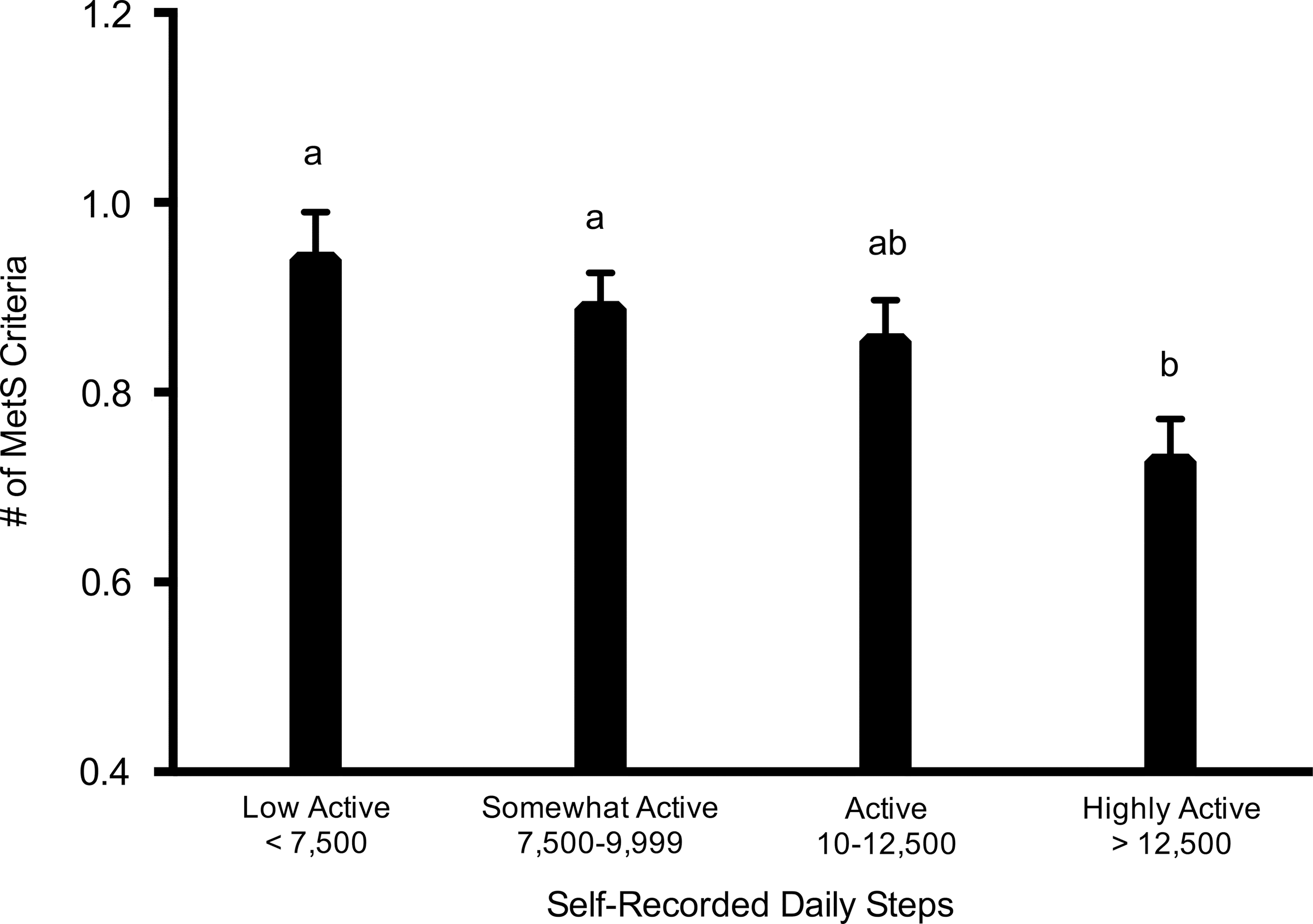
Relationship between number of metabolic syndrome criteria and self-recorded daily steps. Mean differences between categories of self-recorded steps were tested via analysis of covariance (ANCOVA) using the general linear model; sex served as a covariate. MetS, metabolic syndrome.
Data are presented as percentages. Prevalence differences between fitness groups were assessed by chi-squared test for independence.
TAG, triacylglyerides; HDL-C, high-density lipoprotein cholesterol.
Odds ratios (OR) calculated with logistic regression; gender served as a covariate.
CI, confidence interval; HDL-C, high-density lipoprotein cholesterol.
Discussion
To our knowledge, this is the first study to report on the relationship between all components of the metabolic syndrome and cardiovascular fitness among college students. The major finding was that approximately 10% of the students in our sample had lower than average fitness and were at high risk for metabolic syndrome, as well as obesity.
Our findings demonstrate that students with below-average fitness have greater cardiometabolic risk than those with average or above-average fitness. We found that college students with below-average fitness had a five-fold increased risk of having the metabolic syndrome, a 10-fold increased risk of having abdominal obesity, and a 12-fold increased risk of being overfat as compared to college students with average or above-average fitness. Other research suggests that below-average fitness levels during this time negatively impact health. Sacheck et al. found physical fitness was inversely associated with blood glucose and lipids among first-year students. 8 Cardiovascular fitness has also been inversely associated with body fat among young women 16–24 years old 24 and positively associated with insulin sensitivity in a nationally representative sample of adolescent boys 12–19 years. 25 Among Spanish university students, cardiovascular fitness was negatively correlated with BMI, body fat, and blood pressure. 26
Findings from the longitudinal Coronary Artery Risk Development in Young Adults (CARDIA) study showed that low fitness levels doubled the risk of developing hypertension, diabetes, and the metabolic syndrome 15 years later. 27 Likewise, the Amsterdam Growth and Health Longitudinal Study found that the presence of the metabolic syndrome at the age of 36 was associated with a greater decline in cardiorespiratory fitness levels from early adolescence as compared to those without the metabolic syndrome. 1 Importantly, research also suggests that exercise interventions have the potential to reduce disease risk factors among young adults: Cederberg et al. found that the improved cardiovascular endurance observed following an 8-week intensive military training of 1112 young Finnish men correlated to reductions in BMI, waist circumference, body fat, blood pressure, and blood lipids. 28
The current study also suggests that students with low activity, as determined by steps per day, have a greater number of metabolic syndrome criteria than those who are highly active. Others have found that college students spend 4 hr per day engaged in sedentary activities, primarily participating in studying and “screen time” activities (i.e., television, computer, and video games). 6,29 Although the clinical implications are unknown, our findings showed college students with the lowest levels of activity have the highest number of metabolic syndrome criteria. In addition to the positive health outcomes associated with increasing daily activity, a growing body of evidence suggests that decreasing sedentary activities may have independent benefits. 30 A large prospective study of over 100,000 American adults conducted by the American Cancer Society showed that excessive time spent sitting increased all-cause death rates independent of physical activity level. 31 Given the rapidly evolving use of technology by all ages, a better understanding of the cardiometabolic impact of prolonged inactivity is warranted.
Our findings are particularly relevant given that the emerging adult population may not prioritize health-related behaviors such as diet and exercise, in part, because they do not perceive themselves to be at risk for developing chronic disease. Although Munoz et al. found that over 90% of female college students surveyed (n=320) identified physical exercise as an activity that reduces risk of heart disease, 32 Collins et al. reported that two-thirds (67%) of college students incorrectly selected breast cancer as the leading cause of death for women, 33 and Green et al. found that more than two-thirds of college students (n=470) rated their own risk of cardiovascular disease as lower than their peers. 34 These misperceptions among young people are not surprising given the lack of available data or monitoring system that comprehensively captures nutrition, physical activity, and sedentary behaviors of young adults. 35 Further research is needed to ascertain if increasing students' awareness of their individual risk for future disease would predict greater participation in physical activity during the formative young adult years.
Our sample's estimated cardiorespiratory fitness levels were slightly higher (4%–8%) than levels reported by NHANES in men and women 20–29 years (44.5 and 36.5 mL·kg−1·min−1, respectively). 36 As VO2max decreases across all races/ethnic groups with age, this modest difference may be explained by our sample's young age range (i.e., 18–24 years). In addition, differences may be explained in methodology as our study estimated VO2max via a field test (i.e., 1-mile Rockport protocol), whereas NHANES used a submaximal treadmill test. 36 For example, Pribis et al. reported significantly lower cardiorespiratory fitness levels to our findings (17%–20% lower) via the Astrand bike protocol in 5101 college students, 37 whereas Sachek et al. found equivalent values to what we observed among first-year female undergraduate students using the Queens College Step Test. 8
This study has a number of strengths, including a large sample size, multiple measures of activity and fitness, and all components of the metabolic syndrome. However, the study's limitations should be noted. First, our subjects were recruited from a convenience sample of students enrolled in an introductory nutrition course. Although students from all of the university's five colleges complete the course to fulfill a graduation requirement, participation in the course may indicate a stronger interest in health as compared to college students who did not enroll in the course and, in fact, only 10% of the sample had below average fitness. Second, cardiorespiratory fitness was predicted via a field test that required subjects to walk at a self-perceived maximum effort, and self-recorded daily activity was estimated via pedometer and required subjects to correctly wear the provided device and accurately record daily values. Because subjects' participation and completion of these activities also contributed to their course-related assignments, subjects had added incentive to follow instructions. Nonetheless, poor compliance with these methodologies may have impacted predictions of VO2max and activity, respectively. Last, the findings may not be generalizable to college students of differing races or geographical regions due to our state institution's large percentage of white students.
In summary, our findings highlight the important relationship between daily activity, cardiovascular fitness, and health among young, college-age adults—a population largely unaware of their own risk of developing chronic disease. Our findings suggest that the low activity and fitness levels in today's emerging adult population put them at risk for metabolic syndrome, abdominal obesity, and unhealthy weight status and provide a foundation for examining the ability of increased activity to reduce future disease risk.
Footnotes
Acknowledgments
The authors thank Allison MacKenzie and Melissa Rodgers for fitness testing expertise and supervision; Anne Ronan for superb methodological support and oversight; Anna Palange and Leah Tully for clerical support and data entry; David Leach and UNH's Campus Recreation & Athletics staff for use of their facilities; and the numerous graduate and undergraduate research assistants for assistance with data collection. Partial funding was provided by the New Hampshire Agricultural Experiment Station. This is Scientific Contribution #2492.
Author Disclosure Statement
No competing financial interests exist.