
Abstract
Background:
Visceral obesity is associated with insulin resistance, diabetes, and cardiovascular diseases. Vaspin [visceral adipose tissue (VAT)-derived serpin] may be a novel adipokine related to obesity and its metabolic consequences.
Objective:
The aim of this study was to investigate the relationships among serum vaspin levels and VAT and the components of metabolic syndrome.
Methods:
A cross-sectional analysis of healthy men (n=97) and women (n=156) for clinical, laboratory, and anthropometric factors was undertaken. Serum vaspin levels were measured. Abdominal VAT and subcutaneous adipose tissue were measured by computed tomography.
Results:
Of 253 subjects, 47 (18%) had metabolic syndrome: 33 men (34%) and 14 women (9%). Serum vaspin concentration was significantly lower in men than in women and significantly lower in men with metabolic syndrome than in men without metabolic syndrome. Serum vaspin level tended to decrease with increasing number of metabolic syndrome components, and was negatively correlated with waist circumference, systolic and diastolic blood pressure, serum triglyceride level, and abdominal VAT, but positively correlated with high-density lipoprotein cholesterol level. However, after adjustment for sex, this correlation disappeared.
Conclusions:
Low serum vaspin levels are associated with male gender and metabolic syndrome, particularly in men, and with the majority of metabolic syndrome components.
Introduction
Visceral adipose tissue (VAT)-derived serine protease inhibitor (vaspin), a member of the serine protease inhibitor family, is a newly identified adipokine that was originally isolated from the visceral adipose tissue of Otsuka Long–Evans Tokushima Fatty (OLETF) rats aged 6–30 weeks old. 6,7 The OLETF rat is an animal model of metabolic syndrome. 8 Vaspin is detectable in OLETF rats at 6 weeks and is highly expressed in adipocytes of visceral white adipose tissues at 30 weeks, the age when obesity, body weight, and insulin levels peak in OLETF rats. 7 Serum vaspin levels decrease with worsening of diabetes and body weight loss at 50 weeks and are normalized by treatment of OLETF rats with insulin or the insulin-sensitizing agent pioglitazone. 7 Vaspin may have an insulin-sensitizing effect, which may stem from normalization of altered expression of genes relevant to IR in mice with diet-induced obesity. 7 Vaspin is also expressed in human adipose tissues, and its expression has been shown to be higher in obese subjects than in nonobese subjects. 9
Many studies have documented the association between vaspin and obesity and/or T2DM. 1,3,4,7,9 –15 In patients with IR, serum vaspin level is positively correlated with VAT 14 and body mass index (BMI). 15 This suggests that IR may influence the correlation between serum vaspin level and VAT. However, the correlation between serum vaspin level and DM is controversial, 10,13 and studies on the correlation between serum vaspin level and metabolic syndrome are limited. 16 –18 In the present study, we investigated the relationships among serum vaspin levels and VAT and components of metabolic syndrome.
Subjects and Methods
Study population and design
The present study was designed to explore the associations between adiposity and adipokines in the Korean population, and some of its findings have been presented before. 19 In the present study, we recruited healthy adult volunteers (120 men and 180 women) by advertising. Volunteers had to meet the following criteria: (1) Age 19–70 years; (2) judged as healthy by a responsible physician with no abnormality identified on a medical evaluation, including medical history and physical examination; (3) not pregnant in the case of females; and (4) not taking any medication at the time of the study. Participants who were not suitable to participate for any reason, in the opinion of the responsible physician, were excluded. As a result, the final study population included 253 participants (97 men and 156 women).
The study protocol was approved by the Institutional Review Board at Ilsan Paik Hospital (IRB No. IB-0704-025). Informed consent was confirmed by the IRB. All participants were provided informed consents. All participants completed a self-administered questionnaire that included demographic characteristics, general health status, smoking history, and current medications.
Clinical, laboratory, and anthropometric measurements
Anthropometric and body composition measurements were taken from all study participants before breakfast, with the participants wearing light clothing but no shoes. In addition, height, waist circumference (WC), and hip circumference (HC) were measured. BMI was calculated as weight (kg)/height (m)2. WC was measured midway between the inferior margin of the last rib and the crest of the ileum in the horizontal plane. HC was measured around the pelvis at the point of maximal protrusion of the buttocks. Waist-to-hip ratio (WHR) was calculated as WC/HC. The circumferences were measured to the nearest 0.1 cm. Blood pressure was measured from the right arm subsequent to the participant sitting at rest for a period of 20 min. The mean of two consecutive blood pressure recordings was used for statistical analysis.
Total cross-sectional abdominal and visceral fat areas were measured with a computed tomography (CT) scanner (Somatom Plus 4; Siemens, Forchheim, Germany) using an established protocol. 20 A cross-sectional scan (thickness 10 mm) centered at the L4–L5 vertebral disc space was obtained with the participant in the supine position using a radiograph of the skeleton as a reference. This was used to establish the positions of the scans to the nearest millimeter. The abdominal subcutaneous adipose tissue (SAT) area was calculated by subtracting the abdominal VAT area from the total adipose tissue area.
Blood samples were collected from all participants after an overnight fast (10 h) between 08.30 h and 10.30 h, and plasma was stored at −70°C until analysis. Serum vaspin levels were measured with a sandwich enzyme-linked immunosorbent assay (ELISA) kit (AdipoGen, Seoul, Korea) according to the manufacturer's instructions. 12 Inter- and intraassay coefficients of variation were 3.3%–9.1% and 1.3%–3.8%, respectively. The mean of two duplicated values was used for statistical analysis. Fasting plasma glucose, total cholesterol (TC), triglyceride (TG), and high-density lipoprotein cholesterol (HDL-C) levels were measured enzymatically using an autoanalyzer (ADVIA 1650; Bayer Ltd., Tokyo, Japan). High-sensitivity C-reactive protein (hsCRP) was measured by enzyme immunoassay (EIA) using a Modular P800 chemistry analyzer (Roche, Basel, Switzerland). Plasma insulin levels were measured by radioimmunoassay using an Hitachi E170 chemistry analyzer (Hitachi Ltd., Tokyo, Japan). IR index was calculated from the fasting plasma insulin level, and the plasma glucose level was estimated by homeostasis model assessment (HOMA) where 21 HOMA=fasting plasma insulin (IU/mL)·fasting plasma glucose (mmol/L)/22.5.
Metabolic syndrome and obesity assessment
The presence of metabolic syndrome was determined according to the criteria of the 2005 revised National Cholesterol Education Program Adult Treatment Panel III (NCEP ATP III). 22 We defined visceral obesity as a WC of ≥90 cm for men or ≥80 cm for women.
Statistics
Data for continuous variables are shown as the mean±standard deviation (SD). Continuous variables were compared using an independent t-test, and categorical data were compared using a chi-squared test. Simple relationships between serum vaspin levels and other variables were determined using Pearson correlation analysis. Partial correlation analyses were performed to adjust for covariate effects and identify independent relationships. All significance tests were two-sided, and the results were considered statistically significant at P<0.05. All statistical analyses were performed using SAS for Windows (version 9.2; SAS Institute Inc., Cary, NC).
Results
Clinical and anthropometric characteristics and relationship between serum vaspin levels and metabolic syndrome
A total of 47 (18%) subjects had metabolic syndrome, including 33 men (34%) and 14 women (9%) (P<0.001). The groups with metabolic syndrome (MetS+) were older than those without (MetS−). MetS+ individuals had significantly higher BMI, WC, HC, SBP, DBP, fasting plasma insulin and glucose levels, HOMA-IR, TG levels, total abdominal fat, abdominal VAT and SAT, and hsCRP levels, and lower HDL-C levels, compared to MetS− individuals. There was no significant difference in serum vaspin level between the MetS+ and MetS− groups (P=0.06).
There was a significant difference in serum vaspin level between men and women (0.82±1.45 vs. 1.37±1.94, P<0.001) (Fig. 1). In men, MetS+ individuals had significantly higher BMI, WC, HC, SBP, DBP, fasting plasma insulin and glucose levels, HOMA-IR, TG levels, total abdominal fat, abdominal VAT and SAT, and hsCRP levels, and lower HDL-C levels, compared to MetS− individuals. There was a significant difference in serum vaspin level between MetS+ and MetS− individuals (P=0.02). In women, MetS+ individuals were older than MetS− individuals. MetS+ individuals had significantly higher BMI, WC, HC, DBP, fasting plasma insulin and glucose levels, HOMA-IR, TG levels, total abdominal fat, and abdominal VAT and SAT, and lower HDL-C levels, compared to MetS− individuals. There was no significant difference in serum vaspin level between MetS+ and MetS− individuals (P=0.24) (Table 1).
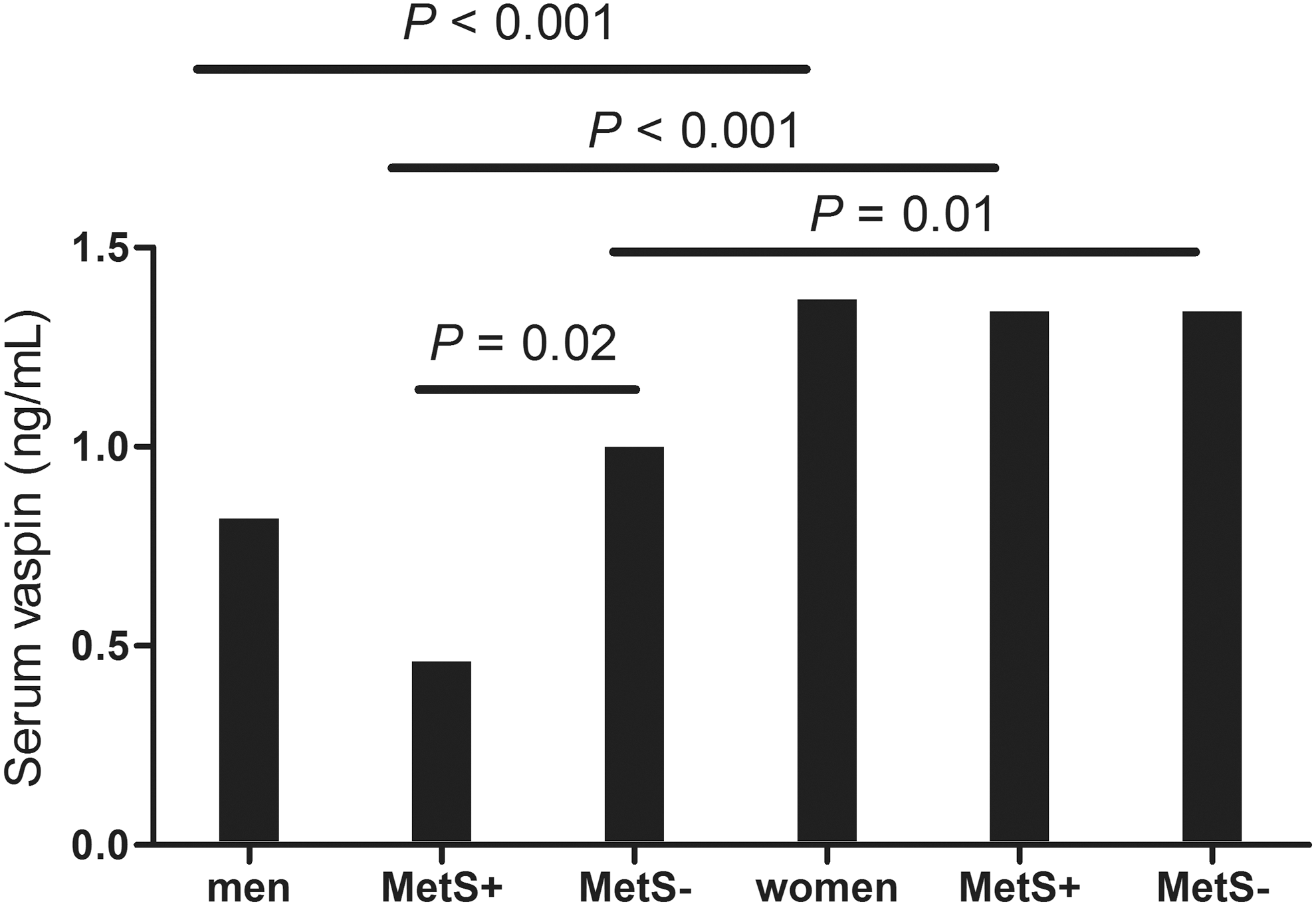
Mean serum vaspin levels according to sex and metabolic syndrome classification. Overall serum vaspin levels collapsed across metabolic syndrome groups were significantly lower in men than in women. Moreover, the serum vaspin concentration was lower in men in the MetS+than in the MetS− group, whereas no significant difference was observed between the metabolic syndrome groups in women. MetS+, with metabolic syndrome; MetS−, without metabolic syndrome.
Data are shown as the mean±standard deviation.
Logarithmic transformation performed before analysis.
P<0.05, ‡ P±0.01, § P±0.001 for patients in the MetS+ group vs. those in the MetS− group across sexes.
P<0.05, ¶ P<0.01, ** P<0.001 for men vs. women according to metabolic syndrome group.
MetS+, with metabolic syndrome; MetS−, without metabolic syndrome; BMI, body mass index; WC, waist circumference; HC, hip circumference; SBP, systolic blood pressure; DBP, diastolic blood pressure; HOMA-IR, homeostasis model assessment-insulin resistance; HDL-C, high-density lipoprotein cholesterol; VAT, visceral adipose tissue; SAT, subcutaneous adipose tissue; hsCRP, high-sensitivity C-reactive protein.
In MetS+ individuals, there were significant differences in age, WC, SBP, DBP, HDL-C level, and abdominal VAT and SAT between men and women. In MetS− individuals, there were significant differences in BMI, WC, HC, SBP, DBP, total cholesterol level, TG level, HDL-C level, and abdominal VAT and SAT between men and women (Table 1). In both MetS+ individuals (P<0.001) and MetS− individuals (P=0.01), there were significant differences in serum vaspin levels between men and women.
Serum vaspin levels decreased with increasing number of metabolic syndrome components, but not significantly (P for trend=0.05; Fig. 2). Vaspin levels were lower in the MetS+ than in the MetS− group for: Individuals under 30 years of age (P=0.022), particularly males (P=0.042); individuals with a BMI greater than 25 (P=0.004); and in males with a WC greater than 90 cm (P=0.048).
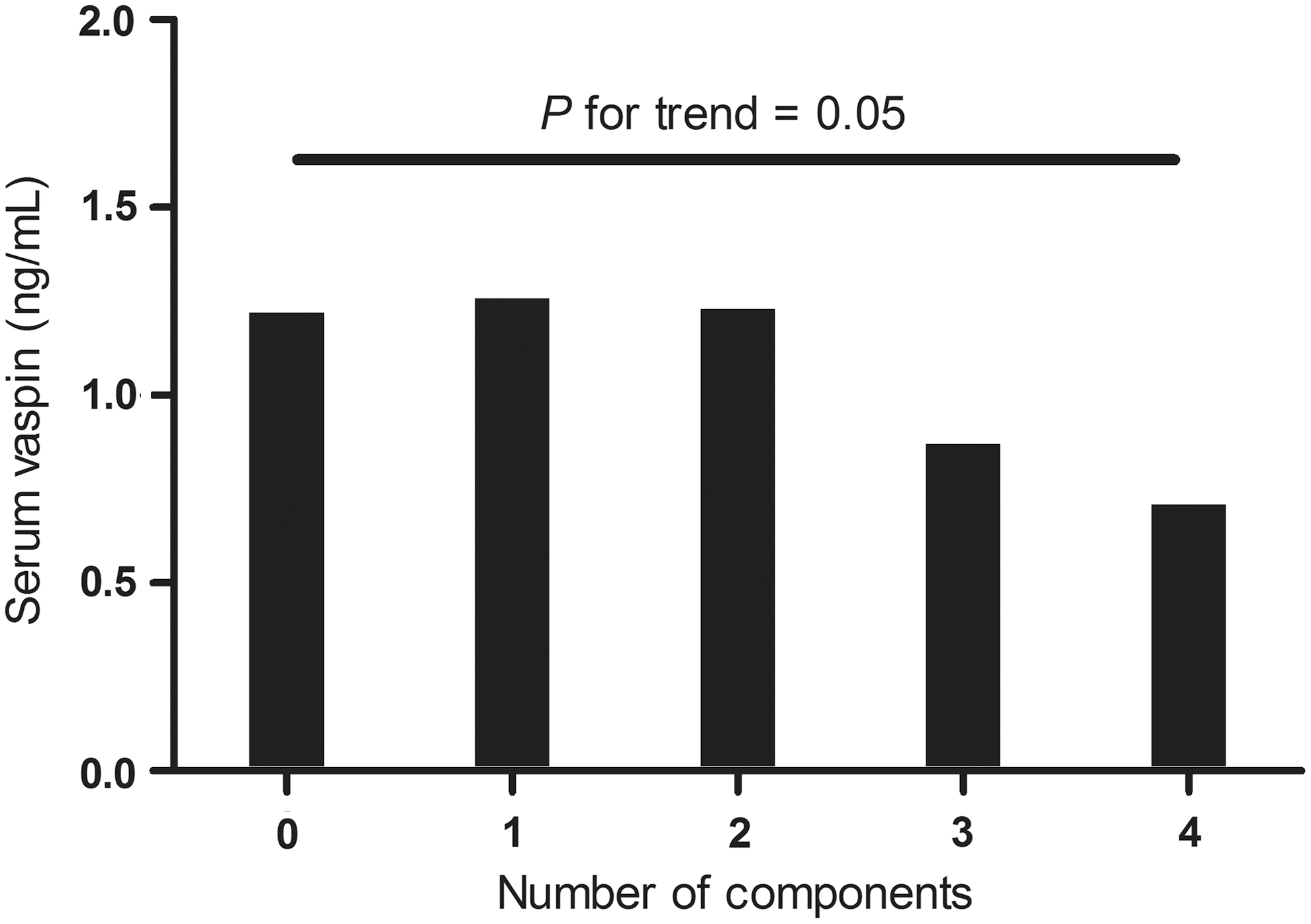
Mean serum vaspin level according to number of metabolic syndrome components. Serum vaspin levels decreased with increasing number of metabolic syndrome components, but not significantly.
Relationship between serum vaspin level and clinical and anthropometric parameters
Pearson correlation analysis of the associations between serum vaspin level and anthropometric measurements, metabolic variables, and abdominal fat distribution was performed. Serum vaspin level was negatively correlated with WC (γ=−0.171), SBP (γ=−0.170), DBP (γ=−0.187), serum TG level (γ=−0.142), and abdominal VAT (γ=−0.130), and positively correlated with HDL-C level (γ=0.177). However, this correlation disappeared in the partial correlation analysis adjusted for sex (Table 2).
Logarithmic transformation performed before analysis.
γ, correlation coefficient (Pearson correlation analysis); BMI, body mass index; WC, waist circumference; HC, hip circumference; SBP, systolic blood pressure; DBP, diastolic blood pressure; HOMA-IR, homeostasis model assessment-insulin resistance; HDL-C, high-density lipoprotein cholesterol; VAT, visceral adipose tissue; SAT, subcutaneous adipose tissue; hsCRP, high-sensitivity C-reactive protein. Statistically significant figures are in bold.
In men in the MetS+ group, serum vaspin levels were correlated with age (P=0.032) and HDL-C (P=0.008), whereas serum vaspin levels were correlated with serum TG levels in men in the MetS− group (P=0.003). However, no significant correlations were found between serum vaspin levels and other factors in women, regardless of metabolic syndrome group (Table 3).
Logarithmic transformation was performed before analysis.
P<0.05, ‡ P<0.01.
γ, correlation coefficient (Pearson correlation analysis); MetS+, with metabolic syndrome; MetS−, without metabolic syndrome; BMI, body mass index; WC, waist circumference; HC, hip circumference; SBP, systolic blood pressure; DBP, diastolic blood pressure; HOMA-IR, homeostasis model assessment-insulin resistance; HDL-C, high-density lipoprotein cholesterol; VAT, visceral adipose tissue; SAT, subcutaneous adipose tissue; hsCRP, high-sensitivity C-reactive protein.
Discussion
There was no difference in mean serum vaspin level between MetS+ and MetS− individuals. Mean serum vaspin level was lower in men compared to women. In men, mean serum vaspin level was lower in MetS+ individuals compared to MetS− individuals. Mean serum vaspin level tended to decrease with increasing number of metabolic syndrome components. Serum vaspin level was negatively correlated with WC, SBP, DBP, serum TG level, and abdominal VAT, but positively correlated with HDL-C level. However, after adjustment for sex, this correlation disappeared.
Why did serum vaspin levels not differ between MetS+and MetS− individuals? First, serum vaspin level may not represent VAT. We expected that serum vaspin level would represent all VAT. However, in this study, serum vaspin level was negatively correlated with abdominal VAT. Vaspin has been identified from VAT of OLETF rats, 6,7 but in those studies it was not expressed in all VAT, and in OLETF rats aged 6–30 weeks, when obesity peaks in these rats, it decreased with worsening of diabetes and body weight loss. 7 In a human study, vaspin mRNA expression was only detectable in 23% of the VAT and 15% of the SAT samples, and was not detectable in lean subjects (BMI <25). 9 In the same study, there was no correlation between visceral vaspin expression and VAT or VAT/SAT ratio, as determined by CT analysis. Because vaspin mRNA expression was detectable in the SAT, SAT is a compounding factor when analyzing the correlation between serum vaspin level and VAT. However, in the present study, serum vaspin level was not correlated with SAT in men or women, nor with the VAT/total abdominal fat ratio or VAT/SAT ratio in men, or women (data not shown). We also did not find a correlation between serum vaspin level and IR. Serial changes in serum vaspin level in subjects would be helpful to find this correlation. Thus, serum and tissue vaspin concentrations may not be related to VAT or IR state.
Second, serum vaspin level differed between men and women. Men and women have different adipose tissue distributions. The increase in body weight in boys is primarily due to an increase in lean mass, whereas that in girls is due to an increase in fat mass. Moreover, menopause is followed by redistribution of adipose tissue toward a more central/android phenotype. 23 Differences in adipose tissue deposition between the sexes are likely to arise partly due to preferential post-absorptive direct free fatty acid (FFA) uptake by SAT in women and enhanced postprandial meal-derived FFA uptake by VAT in men. 23 Progesterone administration increases body and inguinal white adipose tissue masses in female rats, but not male rats. 24 Serum progesterone level is associated with approximately six-fold and two-fold increases in leptin and resistin mRNA levels, respectively, and a two-fold decrease in adiponectin mRNA level, in inguinal white adipose tissue in females; this phenomenon has not been observed in males. 24 Serum leptin 25 and adiponectin levels 26 are lower in men than in women. These sex differences in adipokine production suggest inherent differences in adipocyte function between the sexes or differential regulation by hormones, e.g., suppressive effects of androgens on leptin and adiponectin production. 26,27 They may also be directly and causally related to sex differences in whole-body insulin sensitivity and metabolism. 23 We found that plasma resistin, adiponectin, and leptin levels were lower in men than in women (P=0.002,<0.001,<0.001, respectively; data not shown). Furthermore, serum vaspin and plasma leptin levels were correlated (γ=0.214, P=0.001); however, the correlation disappeared after adjusting for sex. We found no significant differences in resistin and leptin levels between individuals in the MetS+ and MetS− groups; however, plasma adiponectin levels were significantly lower in individuals in the MetS+ compared with those in the MetS− group (52.12 μg/mL vs. 89.28 μg/mL, respectively; P<0.001).
In the present study, women did not have more total body fat than men (data not shown, P=0.67), but had more SAT and less VAT (P<0.001). Metabolic syndrome was more prevalent in men than in women (34% vs. 9%, P<0.001). Men and women had different WC and blood pressure values, irrespective of metabolic syndrome, age, HDL-C level, VAT, and SAT in MetS+ individuals, and BMI, HC, total cholesterol, and TG in MetS− individuals. These differences may have affected the relationship between serum vaspin levels and sex. Serum vaspin levels were correlated with WC, BP, TG level, HDL-C level, and VAT. However, these correlations disappeared after adjusting for sex. The causal nature of the relationship between serum vaspin level and sex is not clear.
It is not clear why serum vaspin was lower in MetS+ men than in MetS− men. A previous study found that plasma vaspin was lower in men than in women, but significantly higher in MetS+ men than in MetS− men. 16 However, this study included patients with diabetes (15% men, 17% women), some, but not all, of whom used antidiabetic medication. Plasma vaspin levels were lower in men who had a longer duration of diabetes or had microvascular complications. Thus, the presence of diabetes may be a compounding factor.
It is not known whether circulating vaspin is related to measures of obesity, insulin sensitivity, and glucose metabolism. Vaspin mRNA levels decrease with worsening of diabetes and increase after treatment with thiazolidinediones, suggesting that vaspin has an insulin-sensitizing effect. 28 Vaspin mRNA expression in adipose tissue is not detectable in lean glucose-tolerant individuals, but is induced by increased fat mass, decreased insulin sensitivity, and impaired glucose tolerance. 9 In insulin-resistant subjects, there is a significant correlation between changes in serum vaspin level and changes in anthropometric and metabolic parameters. 14,15 Serum vaspin level is associated with obesity and impaired insulin sensitivity, whereas T2DM may abrogate the correlation between vaspin and obesity. 12 Collectively, these findings suggest that vaspin expression is related to IR. We believe that serum vaspin levels may serve as a compensatory mechanism associated with metabolic syndrome. Vaspin may have antiatherogenic effects similar to those of interleukin-6. 29 –31 Vaspin has been shown to increase Akt phosphorylation, prevent the linoleic acid-induced decrease Akt phosphorylation in insulin-stimulated endothelial cells, 30 increase nitric oxide secretion in endothelial cells and in the isolated aorta of Sprague–Dawley rats, prevent the fatty acid-induced decreased in endothelium-dependent vasorelaxation in the isolated aorta, 31 and inhibit methylglyoxal (active metabolite of glucose)-induced endothelial cell apoptosis by preventing caspase-3 activation via inhibition of nicotinamide adenine dinucleotide phosphate oxidase-derived reactive oxygen species generation. 29
Furthermore, exercise and diet influence serum vaspin levels. Although exercise did not affect visceral vaspin levels in the diet-induced obese rat, it was associated with a significant reduction in HOMA-IR and significant improvement in other metabolic syndrome parameters. 32 However, exercise has been found to increase serum vaspin levels in humans. 12,33 Serum levels of vaspin were found to increase in lean and obese subjects who lost weight following a 4-week intensive physical training program. In contrast, sportsmen who had undergone long-term physical training had significantly lower serum vaspin levels compared to untrained age- and BMI-matched control subjects. 12 Moreover, a 6-month supervised aerobic exercise program increased serum vaspin levels in T2DM patients. 33 A short period of starvation did not affect serum vaspin levels, 34 whereas a 12-week high-fat diet in diet-induced obese Sprague–Dawley rats decreased serum vaspin levels. The transition from a high-fat diet to a basal diet for 4 weeks increased serum vaspin levels in the obese rats. 35 The authors speculated that the low serum vaspin was a result of worsened insulin resistance and elevated coherent nocuous adipokines induced by the high-fat diet.
Thus, serum vaspin may not reflect IR, but rather serves as a transient adaptation mechanism. In the present study, serum vaspin levels were correlated with VAT but not with HOMA-IR (a marker of IR). However, after adjusting for sex and the presence of metabolic syndrome, the correlation between serum vaspin and VAT disappeared, whereas the correlation between VAT and HOMA-IR remained (data not shown). Thus, it may be that vaspin reflects a change in the IR state, rather than IR itself, and mediates an improvement in IR. However, the causal nature of the relationship between serum vaspin levels and IR is not clear.
This study has some limitations. First, its cross-sectional design makes it difficult to determine the causality of the observed relationship between serum vaspin level and metabolic syndrome. Thus, prospective and intervention studies are needed to confirm the role of vaspin in metabolic syndrome. Second, we were unable to examine the effect of diet and exercise. Several studies have shown that vaspin concentrations are associated with diet and exercise. Third, the study population included significantly more females than males, and although we enrolled healthy participants who were not taking medication, significantly fewer females (9%) than males (34%) had metabolic syndrome. We plan to conduct a further study with a larger number of participants to confirm the results of the present study.
Despite its limitations, the strength of our study lies in the examination of various metabolic parameters related to the pathogenesis of metabolic syndrome in healthy participants without the confounding effects of severe chronic diseases.
Conclusion
Low serum vaspin levels are associated with metabolic syndrome, especially in men. Serum vaspin levels are also associated with most components of metabolic syndrome.
Footnotes
Acknowledgments
This study was sponsored by the Priority Research Centers Program through the National Research Foundation of Korea (NRF), funded by the Ministry of Education, Science and Technology (2010-0020224). This work was supported by the Inje Research and Scholarship Foundation in 2012.
Author Disclosure Statement
No competing financial interests exist.