
Abstract
Objective:
Previous studies suggested that elevated serum γ-glutamyl transferase (GGT) level is an independent predictor of coronary artery disease (CAD) and heart failure (HF). However, whether serum GGT level has a predictive role for HF after percutaneous coronary intervention (PCI) remains unclear. This study aimed to evaluate the association of GGT with HF after PCI in a Chinese population.
Methods:
Five thousand six hundred thirty-eight patients were divided into three groups according to GGT tertiles: first tertile (GGT <19.6 U/L; n = 1875), second tertile (GGT ≥19.6–32.9 U/L; n = 1880), and third tertile (GGT ≥32.9 U/L; n = 1883). There were 165 (2.9%) HFs during a long-term follow-up. The average follow-up time was 35.9 ± 22.6 months.
Results:
The incidence of HF in the first tertile is 62 (3.3%), second tertile is 38 (2.0%), and third tertile is 65 (3.5%). The HF incidence was significantly lower in second tertile compared with that in the first tertile or in the third tertile (both P < 0.05). A U-shaped curve was observed according to quintiles (Q1:3.4%, Q2: 3.0, Q3:1.6%, Q4: 2.9%, Q5: 3.7%, P = 0.042). The multivariate Cox proportional hazards model showed after adjustment of confounders, the association remains significant (P = 0.046).
Conclusions:
This study indicated that serum GGT concentration was independently associated with HF after PCI. The baseline serum GGT level less than 19.6 or ≥32.9 increases HF risk in CAD patients who underwent PCI.
Introduction
Heart failure (HF) is a worldwide epidemic that is associated with considerable hospitalization and mortality. 1 Recently, several studies have shown that elevated γ-glutamyl transferase (GGT) levels are associated with increased risk of coronary artery disease (CAD), 2 –5 mortality, 6,7 and HF. 8,9 Wang et al. 8 enrolled 18,353 Finnish men and 19,726 women who were 25–74 years of age and free of HF at baseline to investigate the relation between serum GGT levels and HF incidence. The authors found moderate to high levels of serum GGT (from the 50th to the 90th percentiles) were significantly associated with HF incidence in men and women in Finland. Wannamethee et al. 9 also found elevated GGT was associated with increased risk of HF in elder men. Radovanovic et al. 10 investigated the mechanism underlying the association between GGT and HF progression and found that GGT levels are associated with left ventricular remodeling in patients with chronic ischemic HF. Although percutaneous coronary intervention (PCI) is an effective therapy and improves the outcomes in CAD patients, a part of CAD patients who underwent PCI developed HF in clinical practices.
As mentioned above, the association of serum GGT level with HF was identified in an epidemiological study. Further, the relation between serum GGT level and CAD had been well established. Therefore, the relation between GGT levels and HF in CAD patients who underwent PCI is an interesting topic and worth clarifying. However, up to date, the relation between GGT levels and HF incidence in CAD patients who underwent PCI remains unclear. In this study, we enrolled 5638 CAD patients who underwent PCI to investigate the association of GGT levels and HF in a Chinese population.
Methods
Design and study population
This study is a part of the Clinical Outcomes and Risk Factors of Patients with Coronary Heart Disease after PCI (CORFCHD-PCI) study carried out in the Department of Cardiology, First Affiliated Hospital of Xinjiang Medical University. The details of the design have been registered on
The study protocol was approved by the Ethics Committee of the First Affiliated Hospital of Xinjiang Medical University. Because of the retrospective design of the study, the need to obtain informed consent from eligible patients was waived by the ethics committee.
In this study, a total of 6050 patients with CAD after PCI were evaluated initially. Four hundred twelve patients were excluded due to no GGT data available, acute infections, malignancies, hepatobiliary disease, or HF. Finally, there were 5638 patients enrolled in this study. The flow chart of inclusion and exclusion of participants was shown in Fig. 1. The PCIs were performed according to standard techniques, by experienced interventionalists. All the investigators passed a formal training before participating in the study.
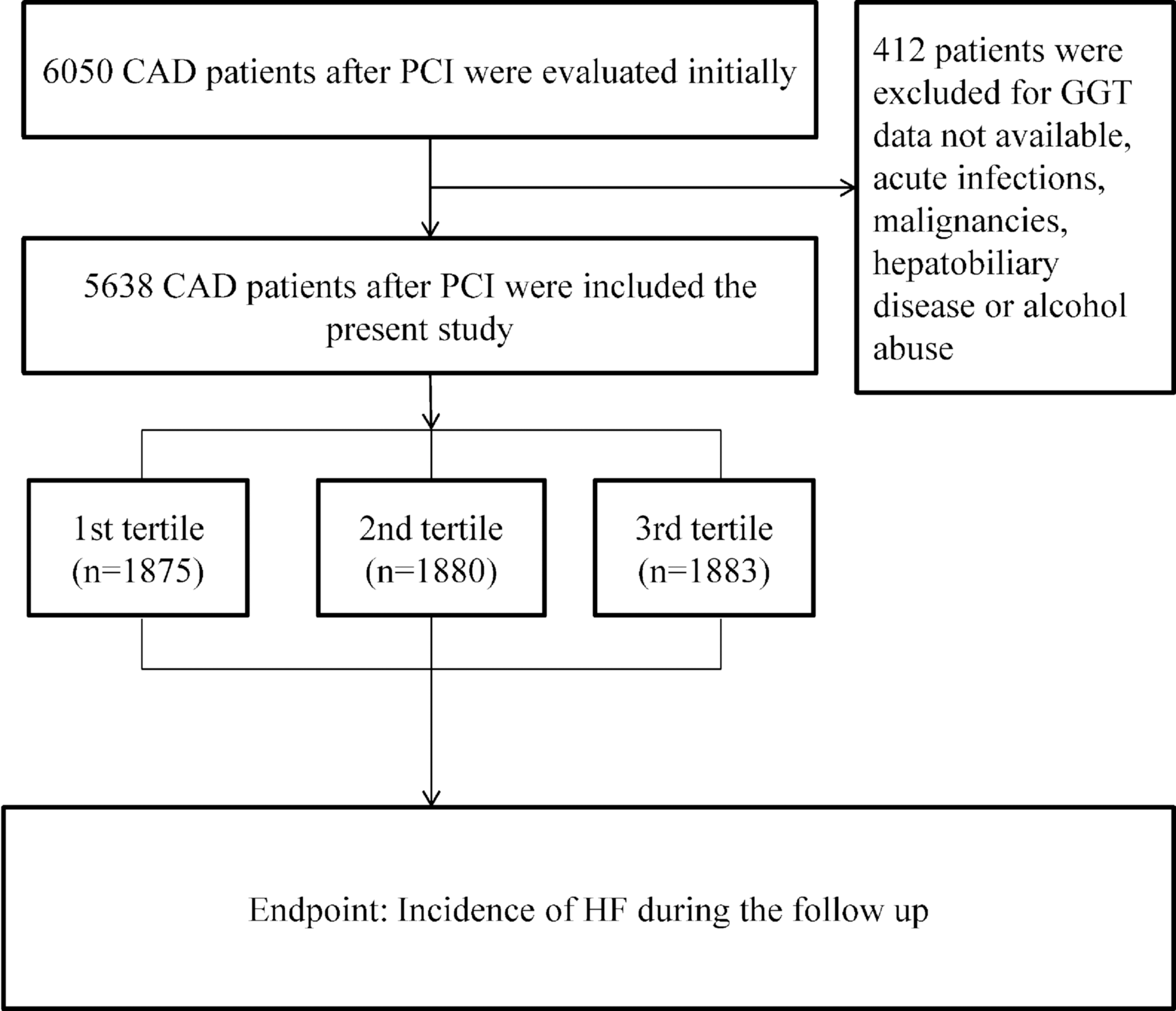
The flow chart of participant's inclusion.
Clinical and demographic characteristics collection
The demographic data, cardiovascular risk factors, and laboratory data including blood routine parameters and biochemical indicators for all patients were recorded. Cardiovascular risk factors included smoking status, drinking, previously diagnosed diabetes mellitus, hypertension, and a history of familial CAD, previous medical and/or surgical diseases, medications. Hypertension was defined when the patient was on active treatment with antihypertensive drugs or blood pressure measurements ≥140/90 mmHg on at least two separate occasions. 11 Diabetes mellitus was positive in patients with a definite history of diabetes and treatment with glucose-lowering agents or a fasting plasma glucose ≥7.1 mmol/L or 2-hr postload glucose ≥11.1 mmol/L. 12 The diagnostic criteria for hyperlipidemia were mainly obtained from “Guideline of Chinese adult dyslipidemia Prevention and Treatment (2016).” 13 Height and weight were obtained while the participants wore light clothing without shoes. Body mass index (BMI) was calculated by dividing the weight in kilograms by the height in meters squared. Persons reporting regular tobacco use in the previous 6 months were considered as current smokers. Persons who were ingesting alcohol in the last 6 months were considered to be alcohol users. 14
GGT detection
Fasting blood samples were collected before coronary angiography with at least 12 hr of fasting. The catalytic activity of GGT in plasma was measured at 37°C with an enzymatic colorimetric assay using standard methods in the Central Laboratory of the First Affiliated Hospital of Xinjiang Medical University. The measuring range in plasma is 3–1200 U/L. The consensus value is ≤60 U/L for healthy men and ≤40 U/L for healthy women.
Follow-up
In our center, all the patients who underwent PCI will receive regular follow-up after discharge at the end of 1 month, 3 months, 6 months, 1 year, 3 years, and 5 years. In this study all the patients were followed up for at least 2 years, the longest follow-up time is 10 years. The average follow-up time was 35.9 ± 22.6 months. The investigators followed the patients, either by office visits or by telephone contacts as necessary. The compliance of the drugs and adverse events were assessed at every visit for clinical follow-up. Incidence of HF comprised of a diagnosis of CAD with LVEF <40%, presence of current symptoms of HF, current treatment with a loop diuretic, and plasma N-terminal pro-B-type natriuretic peptide (NT-pro-BNP) concentration more than 125 ng/L. 15
Statistical analyses
All analyses were performed using SPSS 22.0 for Windows statistical software (SPSS, Inc., Chicago, IL). We classified patients into three groups according to GGT tertiles in the subsequent analyses. Continuous variables were expressed as mean ± standard deviation or median (25th to 75th percentiles) values, whereas categorical variables were presented as percentages. The differences between normally distributed numeric variables were evaluated by one-way ANOVA, while non-normally distributed variables were analyzed by Mann–Whitney U test or Kruskal–Wallis variance analysis as appropriate. Chi-squared test was employed for the comparison of categorical variables. Kaplan–Meier analysis was used for cumulative incidence rates of long-term outcomes and log-rank test was used to compare between groups. To construct the Cox model, univariate models for each of all predictor variables were run, with those variables that were significant (P < 0.05) in univariate analysis were then simultaneously entered into a multivariable Cox model. We also put ejection fraction (EF), angiotensin converting enzyme inhibitor/angiotensin receptor blocker (ACEI/ARB) use, and uric acid (UA) in the multivariable Cox model. The hazard ratios (HRs) and 95% confidence intervals (CIs) were calculated. The cumulative survival curves for the primary outcome and each secondary endpoint were constructed using the Kaplan–Meier method and compared using the log-rank test. P < 0.05 was considered significant.
Results
Baseline data
The study included 5638 patients who were divided into 3 groups according to GGT activity tertiles: first tertile (GGT <19.6 U/L; n = 1875), second tertile (GGT ≥19.6–32.9 U/L; n = 1880), and third tertile (GGT >28.7 U/L; n = 1883). Baseline data are shown in Table 1. A number of variables were significantly different between the patients in GGT tertiles including age, diabetes, blood glucose, total cholesterol, triglyceride, high-density lipoprotein cholesterol, and low-density lipoprotein cholesterol (all P < 0.05). There was no significant difference in therapy of β-blocker, ACEI or ARB, and statins, in addition to smoking, alcohol drinking, hypertension, BMI, BUN, creatinine, and UA among the three groups (all P > 0.05).
Characteristics of Participants of the Three Groups
ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; BMI, body mass index; BUN, blood urea nitrogen; Cr, creatinine; EF, ejection fraction; GLU, glucose; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; TC, total cholesterol; TG, triglyceride; UA, uric acid.
Clinical outcome
There were 165 (2.9%) HFs during the follow-up. The incidence of HF in the first tertile is 62 (3.3%), second tertile is 38 (2.0%), and third tertile is 65 (3.5%). The HF incidence was significantly lower in second tertile compared to that in the first tertile or in the third tertile (Both P < 0.05). Univariate Cox regression analysis showed that compared to patients in the first tertile, the patients in the second tertile have a decrease risk in HF (HR = 0.570, 95% CI: 0.376–0.864, P = 0.008). However, we did not find significant difference between the first tertile and the third tertile (HR = 0.882, 95% CI: 0.614–1.267, P = 0.497, Table 2). As shown in Fig. 2 and Table 3, the multivariate Cox proportional hazards model showed after adjustment of confounders of smoking, alcohol drinking, family CAD history, hypertension, GLU, TG, EF, UA, and ACEI/ARB use, the association remains significant (P = 0.046). A U-shaped curve was observed according to quintiles (Q1:3.4%, Q2: 3.0, Q3:1.6%, Q4: 2.9%, Q5: 3.7%, P = 0.042, Fig. 3).
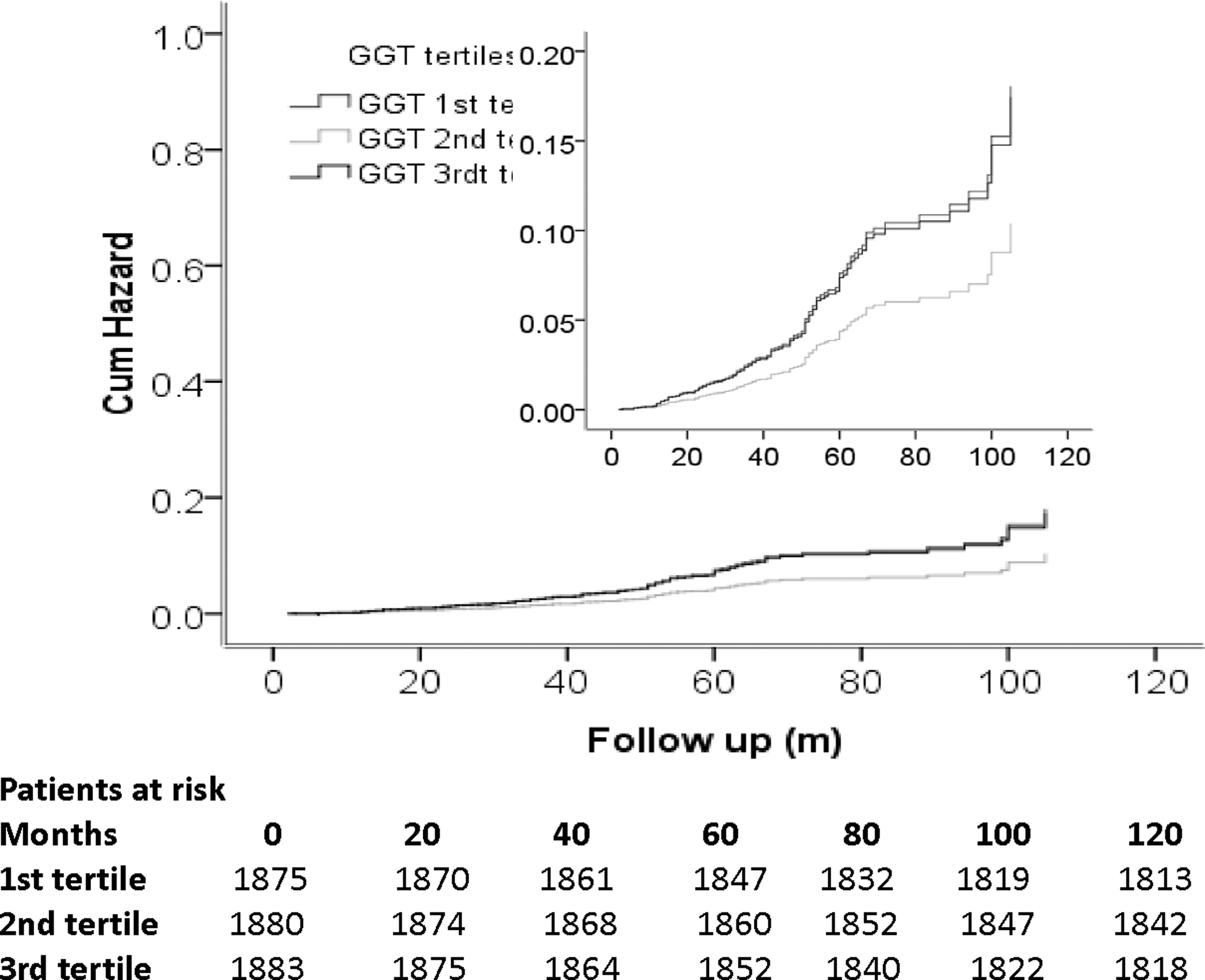
Cumulative Kaplan–Meier estimates of the time to the first adjudicated occurrence of HF. HF, heart failure.
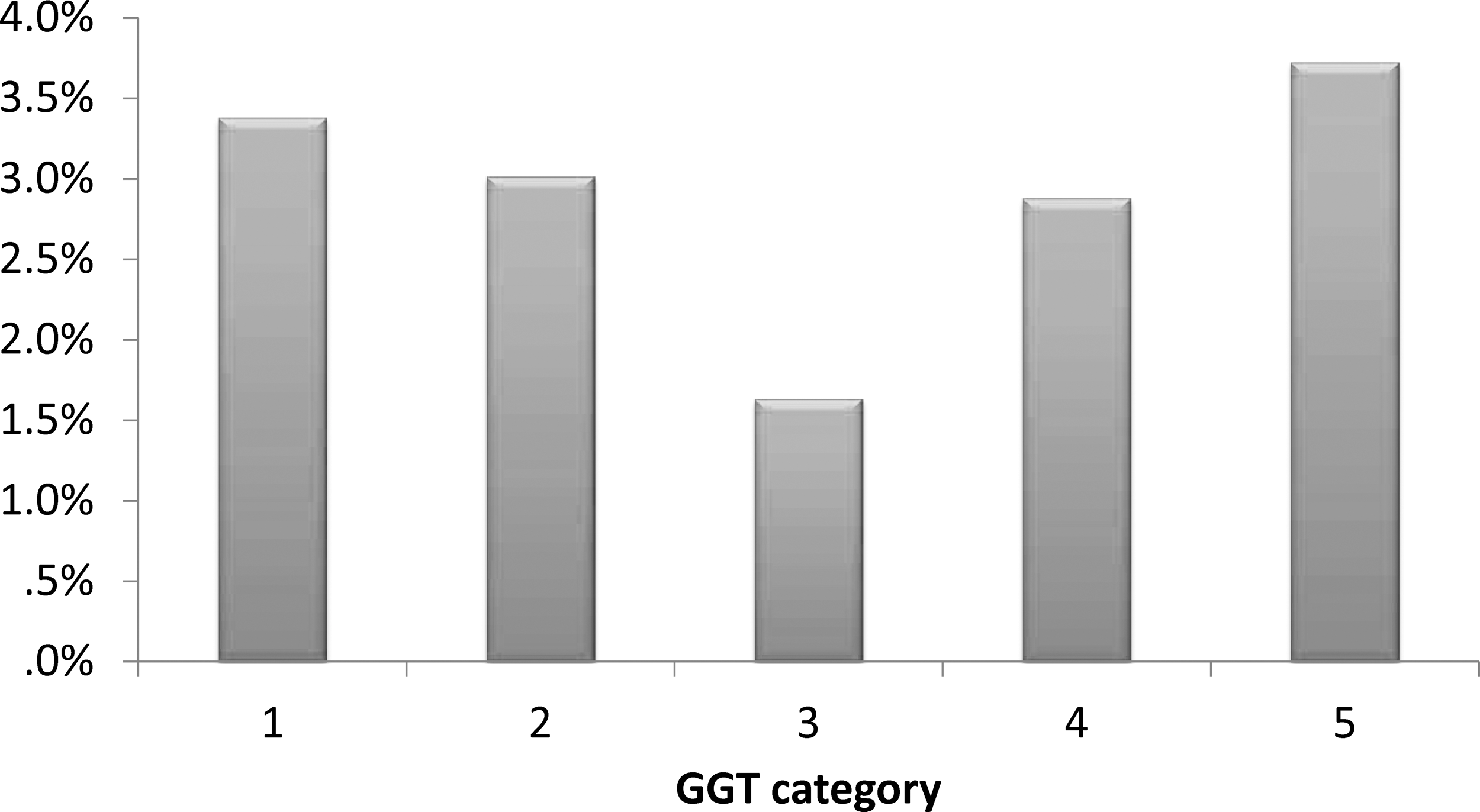
Comparison of incidence of HF among five groups. A U-shaped curve was observed.
Univariate Cox Regression Analysis Results for Heart Failure
CAD, coronary artery disease; CI, confidence interval; GGT, γ-glutamyl transferase; HR, hazard ratio; SE, standard error.
Multivariable Cox Regression Analysis Results for Heart Failure
Discussion
In this study, we first evaluated the association of baseline GGT levels with the incident HF after PCI. We found both decreased and elevated baseline GGT levels increased the HF incidence after PCI and a U-shaped curve was present between GGT and incident HF. In other words, moderate level of GGT (19.2–39.2U/L) is beneficial for HF after PCI.
Previous studies showed that elevated GGT level is associated with morbidity and mortality from cardiovascular disease (CVD). Further, a number of studies indicated that serum GGT levels were associated with increased risk of myocardial infarction, HF, and mortality after PCI. 2 –7,16–19 However, the mechanism of this association remains unclear. Several possible explanations of this association are lack of strong evidences. Previous study 20 suggested that GGT participates in glutathione metabolism and in the extracellular degradation of tantioxidant glutathione GSH, thereby triggering a prooxidant action. However, whether GGT is an innocent bystander or a causal contributor to the development of CVD remains unclear. In addition, elevated GGT may be caused by alcohol consumption and light to moderate alcohol drinking may have a protective effect against CAD and myocardial infarction. 21 –23 However, the relation between elevated GGT and light to moderate alcohol drinking have not been established yet. Further, the protective effect of alcohol on CAD and myocardial infarction may not exist at all according to two recent publications. 24,25 Therefore, although many observational studies suggested elevated GGT was associated with increased risk and mortality of CAD, the relation between GGT and CAD patients after PCI have not been established yet. Several previous studies suggested elevated baseline GGT levels were associated with HF incidence. In our study, we found not only elevated GGT level but also decreased GGT level were associated with incidence of HF in CAD patients after PCI. Further, we also found a U-shaped curve presented between the GGT level and the incidence of HF. Our results challenged the previous reports and provided new evidences for the relation between GGT and HF.
A few strengths of our study are as follows. On one hand, a large sample size is a strength of our study, which improved the statistical power. On the other hand, all the patients were CAD after PCI and were followed up for a long term up to 10 years, the follow-up duration is longer compared to previous studies. However, several limitations of our study also should be mentioned. First, we only collected the baseline GGT data during the study duration. Therefore, the effect of dynamic changed GGT levels cannot be analyzed. Second, this is a retrospective study. Third, a better way to found HF events could be the health system registries interrogation. However, we are not able to carry out this action. Therefore, in our study the incidence of HF may be underestimated. Finally, this study is a single center study. Therefore, our results need to be further verified by a multicenter, prospective study.
In conclusion, this study suggests that decreased physiological serum GGT concentration is independently associated with long-term all-cause mortality and cardiac mortality in CAD patients who underwent PCI.
Footnotes
Acknowledgments
We are grateful to the Department of Cardiology, the First Affiliated Hospital of Xinjiang Medical University for their support and expertise in conducting this study. This research was funded by the National Natural Science Foundation of China (U1603381, 81760043, and 81560070).
Author Disclosure Statement
No conflicting financial interests exist.