
Abstract
Background/Purpose:
This research was performed to determine the effect of naringenin (NAR) in experimental hyperuricemia (HU) induced by potassium oxonate (PO) on uric acid levels and xanthine oxidase (XO), inflammation, apoptotic pathway, DNA damage, and antioxidant system in kidney tissue.
Study Design:
Wistar Albino rats were categorized into four groups: (1) Control group, (2) PO group, (3) [PO+NAR] (2 weeks) group, and (4) PO (2 weeks)+NAR (2 weeks) group.
Methods:
The first group was not administered any drug. In group 2, PO was administered intraperitoneally 250 mg/kg/day for 2 weeks. In the third group, 100 mg/kg/day NAR was given intraperitoneally 1 hr after PO injection for 2 weeks. In the fourth group, PO was injected for the first 2 weeks, followed by NAR injection for the second 2 weeks. Serum uric acid levels, XO, nuclear factor-kappa B, tumor necrosis factor-alpha, interleukin-17, cytochrome c, 8-Hydroxydeoxyguanosine (8-OHdG), glutathione peroxidase (GPx), and caspase-3 levels in kidney were determined.
Results:
HU increased the levels of inflammatory and apoptotic parameters, XO, and 8-OHdG levels in kidney. Administration of NAR caused a decrease in these values and an increase in GPx levels.
Conclusions:
The results of the study show that NAR treatment reduces serum uric acid levels, and apoptosis, inflammation, and DNA damage; increases antioxidant activity in kidney in experimental HU.
Introduction
Hyperuricemia (HU) which is a disease characterized by increased uric acid levels in the blood is associated with chronic kidney disease, coronary heart diseases, hypertension, stroke, neurodegenenerative disorders, and metabolic syndrome. 1 Uric acid is the final product of purine breakdown. Xanthine oxidase (XO), an enzyme that locates at the end of purine nucleotide metabolism, catalyzes the oxidation of hypoxanthine to xanthine and xanthine to uric acid. Levels above 7 mg/dL in men and 6 mg/dL in women are defined as HU. 1 It has been found that HU includes rapid increase in proinflammatory cytokine levels such as interleukin (IL)-6, IL-1β, and tumor necrosis factor-alpha (TNF-α). 2
Apoptosis, an energy-dependent, genetically programmed form of cell death has roles in developmental biology, tissue regulation, kidney injury, and carcinogenesis. 3,4 The role of apoptosis has been shown in HU. It has been reported that HU increased apoptosis in kidney in rats through caspase 3 activity increase. 5 In HU-induced renal tubular injury, caspase 8, caspase 3, caspase 9, and cytochrome c levels are upregulated. 6 In another study, expression of proapoptotic proteins such as cleaved caspase 3 and caspase 9, and bax was upregulated in HU in mice kidney. But the level of antiapoptotic protein bcl-2 was dramatically downregulated. 7
HU also increases oxidative stress markers, and reduces antioxidant enzyme levels such as glutathione peroxidase (GPx) in rat kidney. 5 Furthermore, 8-Hydroxydeoxyguanosine (8-OHdG) immunostaining was upregulated in glomerular cells in the renal cortex in experimental hyperuricemic rats. 8
Flavonoids act as a direct antioxidant through reactive oxygen species (ROS) scavenging and metal chelation. 9 Flavonoids have antioxidant and anti-inflammatory properties 9 as well as antihyperuricemic effects. It was reported that corn silk which contains 12 types of major flavonoids include naringenin (NAR) that decreased the uric acid levels, and the XO activity in serum 10 through XO enzyme inactivation. 11 NAR, one of the most abundant flavonoids, has anti-inflammatory, 12 antiapoptoic, 13,14 antioxidant, 12 hypouricemic, 10 and antidiabetic 12 properties. NAR also reduces oxaliplatin-induced DNA damage in mice through moderating 8-OHdG levels. 15
NAR (50 mg/kg) also attenuated gout-induced renal injury via improving renal function parameters, suppressed inflammatory cytokines, and oxidative stress. 16 It has been reported that 10 and 50 mg/kg NAR attenuated renal impairment due to HU through decreasing the release of inflammatory cytokines such as IL-6 and TNF-α nuclear factor-kappa B (NF-κB). 17
Due to systemic damage such as apoptosis, inflammation, and oxidative stress in kidney during HU and also considering the beneficial effect of NAR on these parameters, this research aimed to determine effects of 2 weeks of administration of NAR on apoptotic marker such as caspase 3, and cytochrome c; oxidative DNA damage marker (8-OHdG); antioxidant activity such as GPx; inflammatory cytokines such as TNF-α, NF-κB, and IL-17; XO activity in kidney tissue and uric acid levels in serum in experimentally HU of rats. Inflammation and oxidative stress cause an injury in kidney. 16,17 Research on the effect of NAR on renal injury in hyperuricemic conditions (during or posthyperuricemia) would be important clinically.
Materials and Methods
Eight to 12 weeks old 35 Wistar type male rats were used in this sudy. The Ethical Approval (2020–2013) of the study was given by Selcuk University Experimental Animals Research and Application Center. The rats were adapted to the environment at 22°C ± 2°C. and 12/12 hr light-dark cycle. The rats were fed a standard diet and water ad libitum. To induce HU, potassium oxonate (PO) (Cat. No.: J60400, 98% purity; Thermofisher Scientific Company) was dissolved in 0.9% saline and given by i.p. way at the dosage of 250 mg/kg/day for 2 weeks. 18 Experimental groups were performed as follows;
1. Control group (n = 7), 2. PO group (n = 9), 3. [PO+NAR] (2) group (n = 9), and 4. PO (2)+NAR (2) group (n = 10) (Fig. 1).
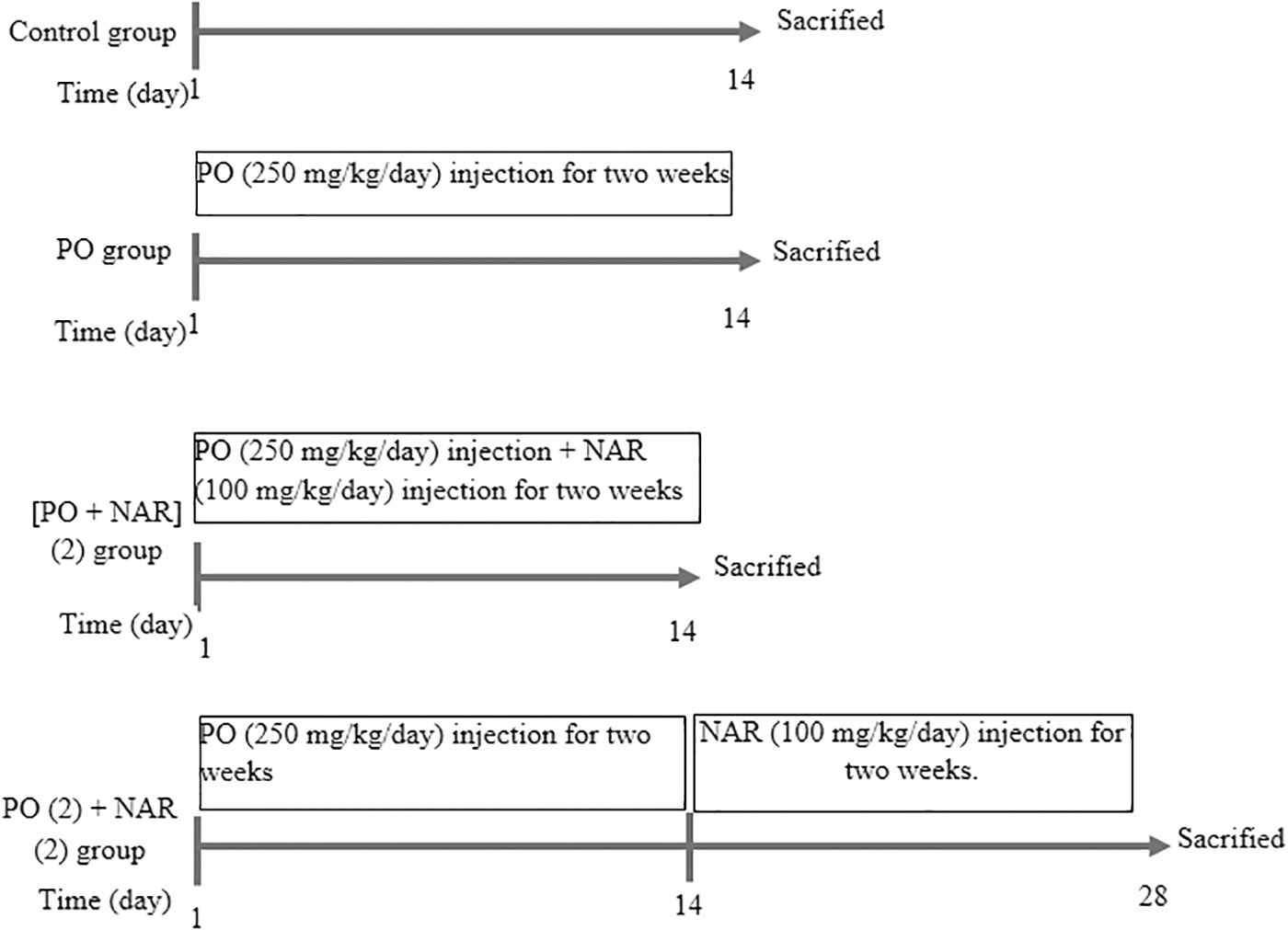
Experimental timeline of study. NAR, naringenin; PO, potassium oxonate.
0.5% sodium carboxymethylcellulose solution was used to dissolve the NAR (N5893, with ±95% purity; Sigma-Aldrich). The dosage of NAR was 100 mg/kg/day i.p. 11 between day 1 and 14 in [PO+NAR] (2) group, and between day 15 and 28 in PO (2)+NAR (2) group.
Blood samples were taken from the rats under general anesthesia [i.p. ketamine HCl (60 mg/kg) and xylazine (5 mg/kg) (Rompun, Bayer)] via intracardiac method and then the rats' lives were ended by cervical dislocation at day 15 in the control group, PO group, and [PO+NAR] (2) group; and day 29 in the PO (2)+NAR (2) group. The blood samples were taken into the tubes and centrifugated in 3500 rpm speed for 10 min to obtain serum samples. The kidney tissue samples were also taken. The kidney tissues were homogenized via 9 × phosphate buffer solution and then centrifuged (5000 g-5 min) to obtain supernatant samples. The supernatant samples were stored at −80°C until analysis.
GPx, caspase 3, cytochrome c, IL-17, NF-κB, TNF-α, XO, and 8-OHdG analyses of the kidney tissues were performed using commercial ELISA kits.
Biochemical analysis
Biochemical Analysis: GPx, caspase 3, cytochrome c, IL-17, NF-κB, TNF-α, XO, and 8-OHdG levels were analyzed in kidney samples through using commercial ELISA kits according to the manufacturer's instructions by using the ELISA reader BMG LABTECH (Germany).
The test kits used in the experiments are as follows; TNF-α (E-EL-R0019; Elabscience) in kidney (pg/mL), GPx (E-EL-R2491; Elabscience) in kidney (pg/mL), caspase 3 (E-EL-R0160; Elabscience) in kidney (ng/mL), cytochrome c (E-EL-R0006; Elabscience) in kidney (ng/mL), IL-17 (E-EL-R0566; Elabscience) in kidney (pg/mL), NF-κB (E-EL-R0673; Elabscience) in kidney (ng/mL), XO (E-EL-R2585; Elabscience) in kidney (ng/mL), and 8-OHdG (E-EL-0028; Elabscience) in kidney (ng/mL).
Serum uric acid levels were analyzed using abbott brand test kits in the Architect C16000 autoanalyzer in the biochemistry laboratory of Medicana Hospital, in KONYA-TURKEY.
Statistic
Kolmogorov Smirnov test was used to determine normal distribution. Later, multivariate analysis of variance was used to compare the quantitative values of the groups. The P values under 0.05 were considered statistically significant. The values are expressed as means ± standard deviation.
Results
Uric acid
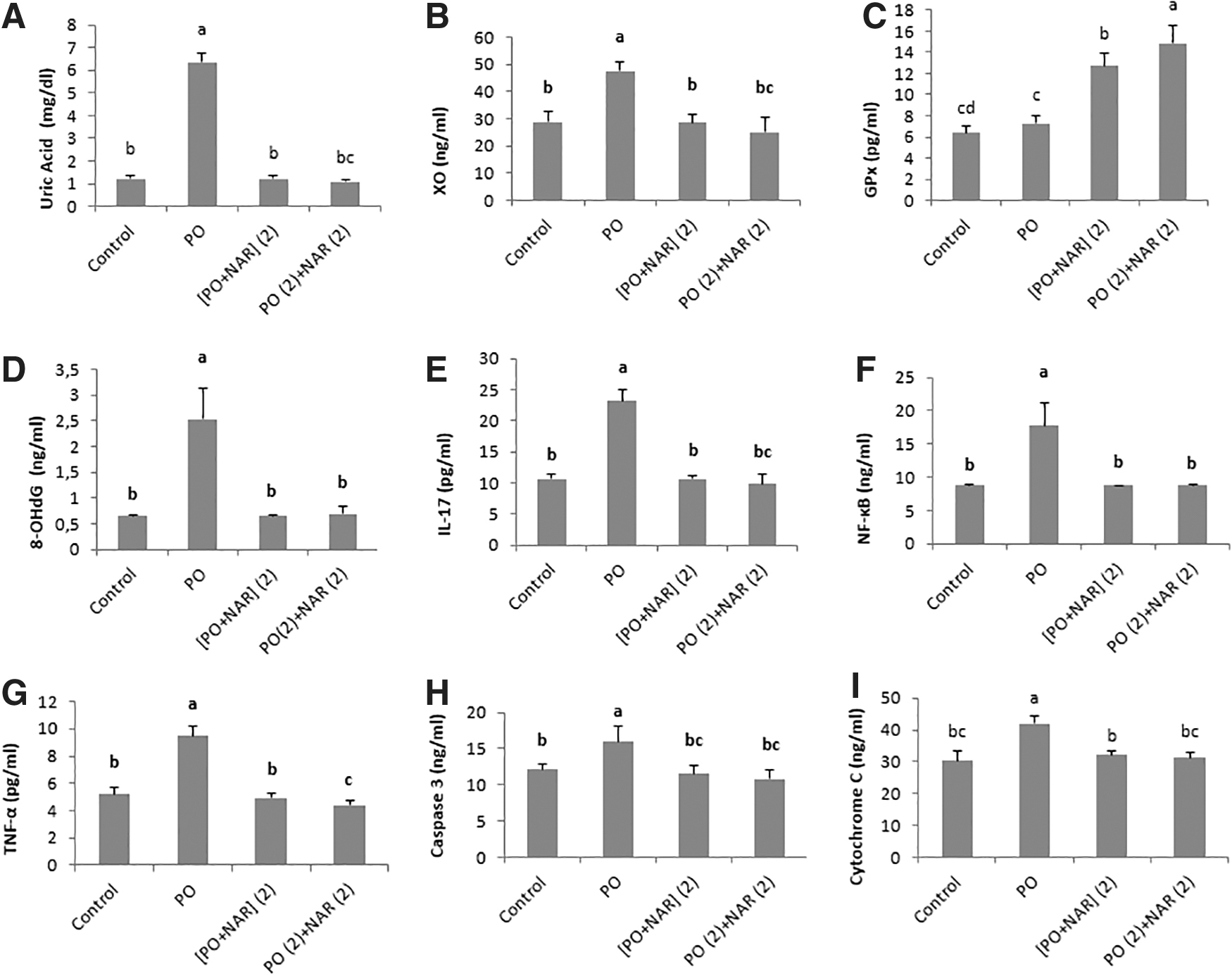
The values of serum UA levels of the groups control, PO, [PO+NAR] (2), and PO (2)+NAR (2) were 1.21 ± 0.14; 6.37 ± 0.36; 1.21 ± 0.18; and 1.08 ± 0.12; respectively. PO injection caused an increase (P < 0.001) in the serum uric acid (UA) levels when compared to the control group. NAR treatment decreased (P < 0.001) the UA levels significantly in both treatment groups (Fig. 2A).
Effect of NAR on markers of oxidative damage/antioxidant enzyme in the kidney. Levels of
Xanthine oxidase
The values of XO levels of the groups control, PO, [PO+NAR] (2), and PO (2)+NAR (2) were 28.88 ± 3.58; 47.6 ± 3.43; 28.53 ± 3.08; and 25.17 ± 5.36; respectively. When the kidney tissue was evaluated in terms of XO activity, a significant enhancement was seen in the PO group compared to the control group (P < 0.001). The XO activity was significantly lower in both NAR groups (P < 0.001) when compared with the PO group (Fig. 2B).
Glutathione peroxidase
The values of GPx levels of the groups control, PO, [PO+NAR] (2), and PO (2)+NAR (2) were 6.38 ± 0.64; 7.26 ± 0.74; 12.74 ± 1.24; and 14.86 ± 1.68; respectively. The PO injection did not lead to a significant change in the GPx activity according to control group (P > 0.05). But NAR treatment increased (P < 0.001) the GPx activity significantly (P < 0.001). The treatment in the PO (2)+NAR (2) group was more effective in increasing the GPx activity than the [PO+NAR] (2) group (P < 0.001; Fig. 2C).
Tumor necrosis factor-alpha
The values of 8-OHdG levels of the groups control, PO, [PO+NAR] (2), and PO (2)+NAR (2) were 5.22 ± 0.53; 9.46 ± 0.71; 4.95 ± 0.38; and 4.38 ± 0.38; respectively. The PO injection caused a significant increase (P < 0.001) in the TNF-α levels when compared to the control group. NAR administration reversed this to the control levels in the [PO+NAR] (2) group. NAR supplementation reduced this parameter. A significant decrease (P < 0.001) was observed in both the NAR treatment groups compared to the PO group. The treatment in the PO (2)+NAR (2) group was more effective in decreasing the TNF-α levels (P < 0.001) than the [PO+NAR] (2) group (Fig. 2G).
Interleukin-17
The values of IL-17 levels of the groups control, PO, [PO+NAR] (2), and PO (2)+NAR (2) were 10.59 ± 0.83; 23.14 ± 1.87; 10.69 ± 0.5; 9.79 ± 1.58; respectively. PO led an increase in IL-17 levels (P < 0.001). However, no difference was observed in treatment groups. NAR administration reversed this to the control levels in both the treatment groups (P < 0.001) (Fig. 2E).
Nuclear factor-kappa B
The values of NF-κB levels of the groups control, PO, [PO+NAR] (2), and PO (2)+NAR (2) were 8.75 ± 0.09; 17.74 ± 3.34; 8.74 ± 0.04; and 8.76 ± 0.08; respectively. When the kidney tissue was evaluated in terms of NF-κB levels, a significant increase (P < 0.001) was seen in the PO group compared to the control group. NAR administration reversed this to the control levels in both the treatment groups (P < 0.001). There was no difference in drug efficacy in both the treatment groups (P > 0.05) (Fig. 2F).
Cytochrome C
The values of cytochrome c levels of the groups control, PO, [PO+NAR] (2), and PO (2)+NAR (2) were 30.41 ± 2.86; 42.05 ± 2.22; 32.11 ± 1.45; and 31.2 ± 1.8; respectively. PO increased cytochrome c levels compared to the control group (P < 0.001). However, NAR administration reversed this to the control levels in both the treatment groups (P < 0.001). There was no difference in drug efficacy in both the treatment groups (P > 0.05) (Fig. 2I).
Caspase 3
The values of caspase 3 levels of the groups control, PO, [PO+NAR] (2), and PO (2)+NAR (2) were 12.09 ± 0.73; 15.93 ± 2.24; 11.51 ± 1.13; and 10.8 ± 1.23; respectively. While a significant increase (P < 0.001) was observed in the caspase 3 values in the PO group compared to the control group, NAR administration reversed this to the control levels in both the treatment groups (P < 0.001). There was no difference in drug efficacy in both the treatment groups (P > 0.05) (Fig. 2H).
8-Hydroxydeoxyguanosine
The values of 8-OHdG levels of the groups control, PO, [PO+NAR] (2), and PO (2)+NAR (2) were 0.65 ± 0.0082; 2.53 ± 0.59; 0.65 ± 0.01; and 0.69 ± 0.14; respectively. PO led an increase (P < 0.001) in the 8-OHdG values according to the control group, NAR administration reversed this to the control levels in both the treatment groups (P < 0.001). There was no difference in drug efficacy in both the treatment groups (P > 0.05) (Fig. 2D).
Discussion
In our study, when we look at the results in general, the serum uric acid values were increased significantly and HU induced by PO. At the same time, it is seen that there was acceleration in apoptotic processes and DNA damage in the kidney tissues due to HU, but both NAR groups significantly suppressed apoptosis and DNA damage through suppressing cytochrome c levels, caspase 3 activity, and 8-OHdG values.
First of all, serum uric acid values were determined. The serum UA values were increased significantly in the PO group according to control values, indicating that HU model was achieved as the first target in the study. NAR treatment significantly reduced the uric acid levels which are induced by PO injection. In the study of Nguyen et al. the HU model was performed by i.p. PO injection (250 mg/kg), which is an uricase inhibitor, and UA values were increased significantly. 19 In a mouse model of PO-induced HU, it has been reported that the administration of anthocyanin, a flavonoid type, significantly reduced serum uric acid, and creatinine values. 20 In the PO-induced HU model, increased UA levels in serum were seen in HU in mice. 21
As emphasized in the studies above, the significant increase in serum UA levels due to HU in our study is similar to the aforementioned studies. In the PO-induced HU mice model, it was observed that serum uric acid levels decreased significantly to the normal levels by oral administrations of the flavonoids such as apigenin, myricetin, quercetin, kaempferol, morin, and puerarin at doses of 50–100 mg/kg. Authors stated that NAR only had significant effects at 100 mg/kg dose. Hypouricemic effects of all compounds were milder and oral NAR supplementation only had significant effects at 100 mg/kg dose. 11 However, in our study, NAR injection decreased serum uric acid values of the rats by decreasing XO activity, which were increased due to HU, to control levels, and this reveals the effectiveness of the NAR treatment.
Analysis of this study showed that in HU XO levels were increased significantly. However, the increase of XO values were suppressed significantly by NAR supplementation. It has been found that some flavonoids such as acacetin have beneficial hypouricemic effects due to their XO inhibitory activities, and it is predicted that they can be used in the treatment of real clinical situations such as HU and gout. 19 Yuan et al. reported that corn silk, which contains some major flavonoids includes NAR, and decreased the UA values and the serum XO activity by 26.69%, and 11.29%, respectively, in mice. In addition to their anti-inflammatory and antioxidant properties, flavonoids have anti-XO activity. 22,23 In our study, the reduced XO activity in the kidney due to NAR supplemantaion for 2 weeks is similar to the previously mentioned research.
Another parameter evaluated in our study was GPx. In kidney tissue, GPx levels were increased significantly in both NAR treatment groups. In a study, 250 mg/kg i.p. PO injection for 10 days, caused a decrease in GPx activity. 24 HU is associated with high oxidative stress level. 24,25 NAR treatment for 7 days increased GPx and catalase levels in thermally induced skin injury. 26 The fact that 100 mg/kg/day NAR supplementation for 2 weeks caused a increase in GPx levels in kidney in our study and is in parallel with previous studies.
8-OHdG values in the kidney tissues in PO group were significantly increased. However, NAR reduced 8-OHdG values. It has been reported that NAR oxime showed its antioxidant activity due to reducing ROS-mediated 8-OHdG values, thus preventing oxidative DNA damage. 27 In our research, the increased DNA damage induced by HU in kidney was reduced by 2 weeks of NAR supplementation, which is in line with the previous studies mentioned above.
Kidney tissue was analyzed in terms of inflammation, it was determined that TNF-α, IL-17, and NF-κB levels were increased by HU, but decreased with NAR treatment. In a study, it was reported that NAR supplementation suppressed monosodium urate crystal-induced TNF-α, IL-17, and NF-κB level increase. 28 Xiao et al. reported that levels of proinflammatory factors such as IL-1β, IL-6, and TNF-α increased in kidney tissue in HU in rats. 29 Furthermore, 50 mg/kg/day NAR treatment for 3 months reduced the lipid profile significantly, and inhibited prooxidants and also inflammation marker levels in the hypercholesterolemic rat kidneys. 30
It has been reported that NAR suppresses IL-6, IL-17, and TNF-α production in a dose-dependent manner. 31 NAR suppressed IL-17, IL-6, and TNF-α levels in skin damage induced by ultraviolet irradiation. 32 NF-κB signal activation induced by HU caused renal inflammation in the hyperuricemic mouse tubule. 33 Moreover NAR reduced NF-κB, IL-6, IL-1β, and TNF-α levels in the the radiation-induced spleen injury. 34 The effect of NAR supplementation on NF-κB levels in kidney tissue in rats was not searched in the above-mentioned studies in a direct HU model. Suppression of NF-κB levels by NAR administration was in parallel with the studies mentioned above. In our research, the fact that i.p. NAR treatment-posttreatment at a dose of 100 mg/kg/day for 2 weeks suppressed the inflammation in the kidney tissue is similar to the previous studies.
Apoptosis levels in kidney tissues was increased in HU, but decreased with NAR injection. Cytochrome c release, which is regulated by bcl-2 proteins, is a necessary cofactor in the activation of caspases such as caspase 3 and caspase 9. 35 NAR inhibited H2O2-induced mitochondrial dysfunction, including decreased cytochrome c release, caspase 3 cleavage and bcl-2/bax ratio. 36
NAR also has antiapoptotic properties in cardiac ischemia reperfusion through suppressing mitochondrial cytochrome c release. 14 Also, it was reported that NAR suppelementation suppressed mitochondria-mediated apoptosis through reducing cytochrome c release from mitochondria. 37 Moreover, NAR suppressed caspase 3 activity in homocysteinemi. 38 Again, NAR protects against vancomycin-induced kidney damage through preventing apoptosis and oxidative stress, and 25 and 50 mg/kg doses are more effective than 100 mg/kg doses. 13 Yang et al. determined that UA causes apoptosis by increasing caspase 3 and bax levels. 39 In our research, caspase 3 and cytochrome c levels were reduced by the administration of 100 mg/kg NAR treatment-posttreatment which is parallel to research.
Conclusion
According to the results of this study, it is observed that i.p. NAR treatment/posttreatment for 2 weeks suppressed serum uric acid levels, apoptotic activity, oxidative DNA damage, and inflammation; increased antioxidant activity in the kidney tissue. The use of NAR and similar substances as a prophylactic or subsequent prophylactic in HU should be considered, taking into account the protective effect against organ damage.
Footnotes
Acknowledgment
The results described in this article were second part of PhD thesis of Z.C.
Authors' Contributions
Z.C.: Conceptualization, Investigation, Resources, Methodology, and Formal analysis. D.D.: Methodology. A.K.B.: Writing—Review and Editing, and Visualization. R.M.: Funding acquisition Writing-Review and Editing, Visualization, and Project administration.
Availability of Data and Materials
Yes. The datasets which were generated during the current study are available from the corresponding author on reasonable request.
Ethical Approval
Ethical Approval of this study was given by Selcuk University Experimental Animal Research and Application Center (2020–2013) and the study was done in this center.
Consent to Participate
Animal study.
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
Author R.M. has received research support from Selcuk University Scientific Research Project Coordinatorship (SUBAP) (Grant number [19202068]).