
Abstract
Background:
This study investigated the association of four metabolic obesity phenotypes with incident coronary artery disease and stroke in a large-scale, community population-based, prospective Korean cohort observed for over 10 years.
Methods:
The study participants included 7374 adults aged 40–69 years, drawn from the Korean Genome and Epidemiology Study. Participants with different metabolic obesity phenotypes were categorized according to body weight and metabolic health status into four groups: metabolically healthy nonobese (MHNO), metabolically healthy obese (MHO), metabolically unhealthy nonobese (MUHNO), and metabolically unhealthy obese (MUHO). Combined cardiovascular events were defined as coronary artery disease and stroke. We used multivariate Cox proportional hazards regression models to prospectively assess hazard ratios (HRs) with 95% confidence intervals (CIs) for incident coronary artery disease or stroke over 10 years after the baseline survey.
Results:
During the follow-up period, newly developed coronary artery disease, stroke, and combined cardiovascular events were diagnosed in 151 (2.0%), 137 (1.9%), and 283 (3.8%) participants, respectively. After adjusting for confounding variables, the HRs (95% CIs) for incident combined cardiovascular events were 1.81 (1.34–2.46) in the MUHO group, 1.29 (0.92–1.81) in the MUHNO group, and 1.21 (0.81–1.79) in the MHO group compared with those in the MHNO group.
Conclusions:
This study revealed distinct risks associated with four metabolic obesity phenotypes concerning incident coronary artery disease and stroke. After adjusting for potential confounding variables, the results indicated that MUHO, but not MUHNO or MHO, showed a higher risk of developing coronary artery disease and stroke than MHNO.
Introduction
Coronary artery disease and stroke are the leading causes of mortality and disability among adults globally, 1 with their incidence reportedly on the rise, posing a significant threat to public health. 2,3 In South Korea, heart disease ranks second, with stroke following as the fourth leading cause of mortality. 4 Consequently, cardiovascular diseases (CVDs), including coronary artery disease and stroke, incur higher medical expenditures than other noncommunicable diseases, 5 making their prevention essential from a public health perspective. This necessitates managing risk factors such as obesity and metabolic syndrome, which unfortunately continue to increase in South Korea due to the adoption of westernized lifestyle habits. 6,7
The concept of metabolic health has emerged as a potential tool for the prediction and prevention of CVDs. While not considered superior to established risk prediction models, it offers valuable insights for the prediction of CVD risk, especially in subgroups, such as individuals across different body mass index (BMI) categories. 8
Obesity, defined by BMI, is a remarkably heterogeneous condition with varying metabolic manifestations among individuals. Considering metabolic abnormalities alongside obesity, rather than relying solely on BMI, appears to reflect the risk of CVDs better. 9,10 This approach categorized metabolic obesity phenotypes into four categories: metabolically healthy nonobese (MHNO), metabolically healthy obese (MHO), metabolically unhealthy nonobese (MUHNO), and metabolically unhealthy obese (MUHO). 11
Recent evidence suggests that MUHO patients are at risk for CVDs, with MHO and MUHNO patients having a higher CVD risk than MHNO patients. Notably, a U.S. study revealed a higher probability of major adverse cardiovascular events among MUHNO patients than among MHNO patients. 12 In contrast, a U.K. study highlighted a higher risk of atherosclerotic CVDs in MHO patients compared to MHNO patients. 13 Nonetheless, limited studies have been conducted on diverse ethnic groups, and few prospective cohort studies have investigated the association between the four metabolic obesity phenotypes and incident cardiovascular outcomes. Therefore, the present study aimed to investigate the association of the four metabolic obesity phenotypes with incident coronary artery disease and stroke in a large-scale, community population-based, prospective Korean cohort observed for over 10 years.
Materials and Methods
Study overview and study participants
The Korean Genome and Epidemiology Study (KoGES) conducted by the Korea Disease Control and Prevention Agency was a population-based, prospective cohort study. Its aim was to investigate chronic disease prevalence and associated risk factors among adults aged 40–69 years in Ansan (an urban area) and Anseong (a rural area) in Korea. This study's participants were recruited from the Korea Association Resource project, a part of the KoGES. A previous study describes details on the methodology and study participants of the KoGES. 14
Data collection in this study included sociodemographic information and past medical history recorded using a self-administered questionnaire, laboratory biochemical measurements, and anthropometric measurements. In addition, each study participants completed a health-related behavior questionnaire covering alcohol consumption, smoking habits, and physical activity. An “alcohol drinker” was defined as an individual who consumed alcoholic beverages at least twice a week. A “current smoker” was identified as someone who smoked during the study period. A “regular exerciser” was characterized by engaging in moderate-to-vigorous physical activities for over 30 min daily. The interviewers used a standardized protocol to inquire about the participants's smoking, drinking, and physical activity habits. 14
The history of incident coronary artery disease and stroke for each participant was collected using self-reported questionnaires administered by well-trained examiners during follow-up sessions. In-depth personal interviews were conducted to confirm an incident coronary artery disease and stroke case when a participant reported an incident coronary artery disease and stroke event in the personal medical history questionnaire. Moreover, when the participants self-reported having a certain disease, interviewers cross-checked if the diagnosis was received from a doctor to improve the survey reliability. Combined cardiovascular events were defined as coronary artery disease and stroke.
Baseline examinations were performed between 2001 and 2002, while subsequent follow-up examinations were carried out biennially until 2012. Of the 8840 participants in the baseline survey, 188 individuals with BMI <18.5 kg/m2 or a history of coronary artery disease, stroke, or chronic heart failure were excluded. During the 10-year follow-up period, 1270 participants who were lost to follow-up or had incomplete follow-up data were further excluded. In addition, eight participants with missing data on coronary artery disease, stroke, waist circumference, blood pressure (BP), fasting plasma glucose, triglyceride (TG), or high-density lipoprotein cholesterol (HDL-C) were excluded. Finally, 7374 participants were included for analysis after these exclusions.
Hypertension was defined as systolic blood pressure (SBP) ≥140 mmHg, diastolic blood pressure (DBP) ≥90 mmHg, or the current use of hypertension medication. Diabetes was defined as a fasting plasma glucose level ≥126 mg/dL, HbA1c level ≥6.5%, or current use of diabetes medication. Dyslipidemia was defined as total cholesterol ≥240 mg/dL, TG ≥200 mg/dL, HDL-C <40 mg/dL, low-density lipoprotein cholesterol ≥160 mg/dL, or current use of dyslipidemia medications.
The study protocol adhered to the ethical guidelines of the 1975 Declaration of Helsinki, as reflected in an a priori approval by the Institutional Review Board (IRB) of Yonsei University Yongin Severance Hospital (IRB Approval No. 9-2016-0013). Written informed consent was obtained from all participants who voluntarily participated in the study.
Clinical and biochemical measurements
Trained personnel conducted anthropometric measurements using standardized procedures. Participants' height, body weight, and waist circumference were measured with the individual wearing light clothing without shoes. BMI was calculated as weight (kg) divided by height squared (m2). Waist circumference was measured at the midpoint between the lower border of the rib cage and the iliac crest. SBP and DBP were measured using a mercury sphygmomanometer.
Blood samples were collected in the morning after overnight fasting. Fasting plasma glucose, total cholesterol, TG, and HDL-C levels were measured using an automatic analyzer (ADVIA 1650; Siemens, Tarrytown, NY).
Definition of metabolic obesity phenotypes
A metabolically unhealthy participant was defined as an individual with at least two of the following four metabolic risk factors: (i) elevated BP (SBP ≥130 mmHg, DBP ≥85 mmHg, or an intake of any antihypertensive medication); (ii) high fasting plasma glucose levels (≥100 mg/dL or the use of insulin or any antidiabetic medication); (iii) high plasma TG levels (≥150 mg/dL); and (iv) low HDL-C levels (<40 mg/dL in men or <50 mg/dL in women). Obesity was defined as a BMI of ≥25 kg/m2 (vs. <25 kg/m2 for nonobese individuals) according to the Asia-Pacific BMI criteria based on the Asia-Pacific regional guidelines of the World Health Organization and International Obesity Task Force. 15 In this study, the waist circumference criterion was omitted due to its collinearity with BMI.
According to these criteria, participants were assigned to one of the following four groups: (i) the MHNO group, which comprised participants with BMI <25 kg/m2 and fewer than two metabolic risk factors; (ii) the MHO group, which consisted of participants with BMI ≥25 kg/m2 and fewer than two metabolic risk factors; (iii) the MUHNO group, which comprised participants with BMI <25 kg/m2 and at least two metabolic risk factors; and (iv) the MUHO groups, which comprised participants with BMI ≥25 kg/m2 and at least two metabolic risk factors.
Statistical analyses
Baseline characteristics of study participants with different phenotypes were compared using either a one-way analysis of variance or the Kruskal–Wallis test for continuous variables according to the normality of distribution. Categorical variables were compared using the chi-squared test. Continuous data are presented as means ± standard deviations or medians (interquartile ranges), while categorical data are expressed as numbers and percentages (%).
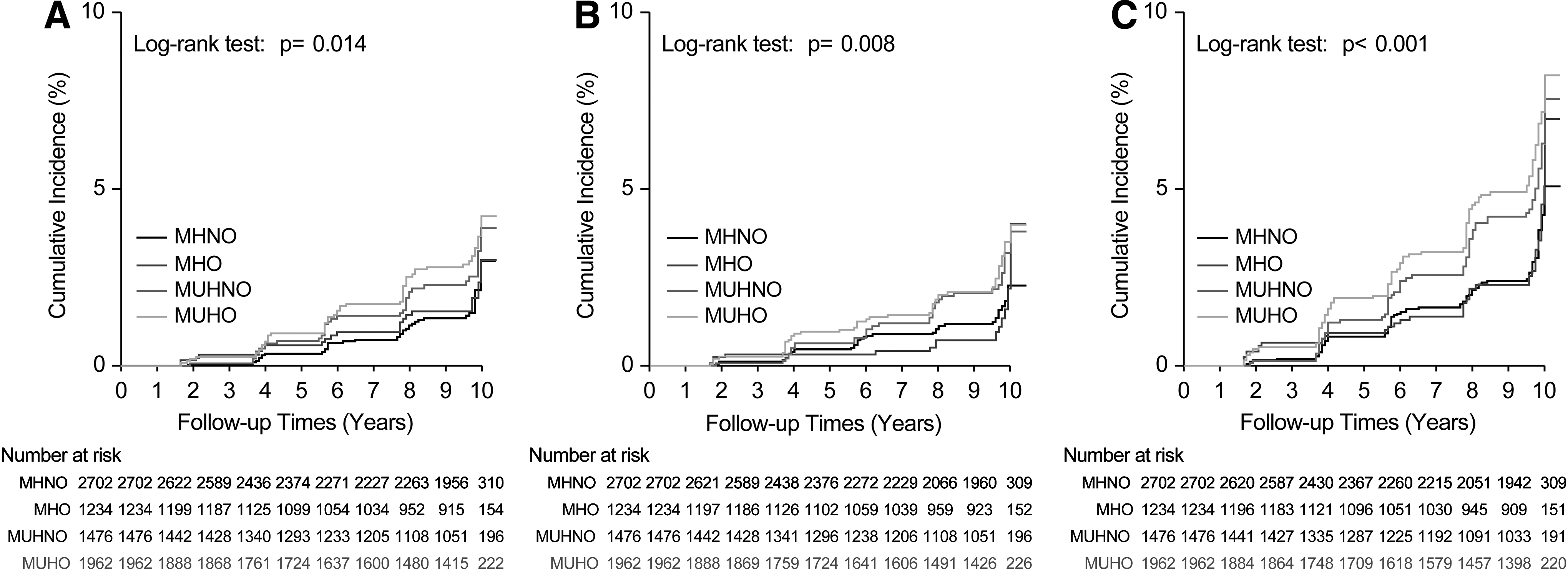
Survival data were censored after the first event, and individuals without the event were censored after the last follow-up. The cumulative incidence of the first incident coronary artery disease, stroke, and combined cardiovascular events was determined by constructing Kaplan–Meier curves. Differences in cumulative incidence among the groups for incident coronary artery disease, stroke, and combined cardiovascular events were examined using log-rank tests.
To confirm event occurrence risks over time after adjusting for potential confounding variables, multivariate Cox proportional hazards regression models were used to estimate the hazard ratios (HRs) with 95% confidence intervals (CIs) for incident coronary artery disease, stroke, and combined cardiovascular events, with the MHNO group serving as the reference group. All statistical analyses were performed using SAS statistical software version 9.4 (SAS Institute, Inc., Cary, NC), with statistical significance set at P < 0.05.
Results
Supplementary Table S1 presents the baseline characteristics of the study participants between the participants who were retained for follow-up and had complete follow-up data and participants who were lost to follow-up or had incomplete follow-up data. Table 1 summarizes the baseline characteristics of 7374 participants categorized into four metabolic obesity phenotypes. Among them, 36.6% (n = 2702), 16.7% (n = 1234), 20.0% (n = 1476), and 26.6% (n = 1962) exhibited the MHNO, MHO, MUHNO, and MUHO phenotypes, respectively.
Baseline Characteristics of the Study Participants According to the Four Metabolic Obesity Phenotypes
Data are presented as means ± standard deviations, medians (interquartile ranges) for continuous variables, or n (%) for categorical variables. P values were obtained using a one-way analysis of variance, Kruskal–Wallis test, or chi-squared test.
P values represent the difference in each variable among the MHNO, MHO, MUHNO, and MUHO phenotypes: *difference in each variable between the MHNO and MHO phenotypes, **difference in each variable between the MUHNO and MUHO phenotypes, and ***difference in each variable between the MHO and MUHNO phenotypes.
BMI, body mass index; DBP, diastolic blood pressure; FPG, fasting plasma glucose; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; MHNO, metabolically healthy nonobese; MHO, metabolically healthy obese; MUHNO, metabolically unhealthy nonobese; MUHO, metabolically unhealthy obese; SBP, systolic blood pressure; TG, triglyceride.
Table 2 presents the incidence of coronary artery disease, stroke, and combined cardiovascular events over the 10-year period, with biennially calculated incidence rates. Of the 7374 participants, 2.0% (n = 151), 1.9% (n = 137), and 3.8% (n = 283) experienced new cases of coronary artery disease, stroke, and combined cardiovascular events, respectively. The incidence rate per 2 years was 0.3–0.8 for coronary artery disease, 0.4–0.7 for stroke, and 0.7–1.2 for combined cardiovascular events.
Incidence of Coronary Artery Disease and Stroke During the Follow-Up Period
Figure 1 depicts the cumulative incidence of coronary artery disease (Fig. 1A), stroke (Fig. 1B), and combined cardiovascular events (Fig. 1C) using Kaplan–Meier curves according to the four metabolic obesity phenotypes. During the observational period, the cumulative incidence of combined cardiovascular events showed a higher tendency in the order of MUHO, MUHNO, MHO, and MHNO.
Cumulative incidence of coronary artery disease
Figure 2 shows a forest plot of HRs with 95% CIs for incident coronary artery disease, stroke, and combined cardiovascular events according to the four metabolic obesity phenotypes. MUHO and MUHNO showed a significantly higher risk of incident coronary artery disease and combined cardiovascular events than MHNO.
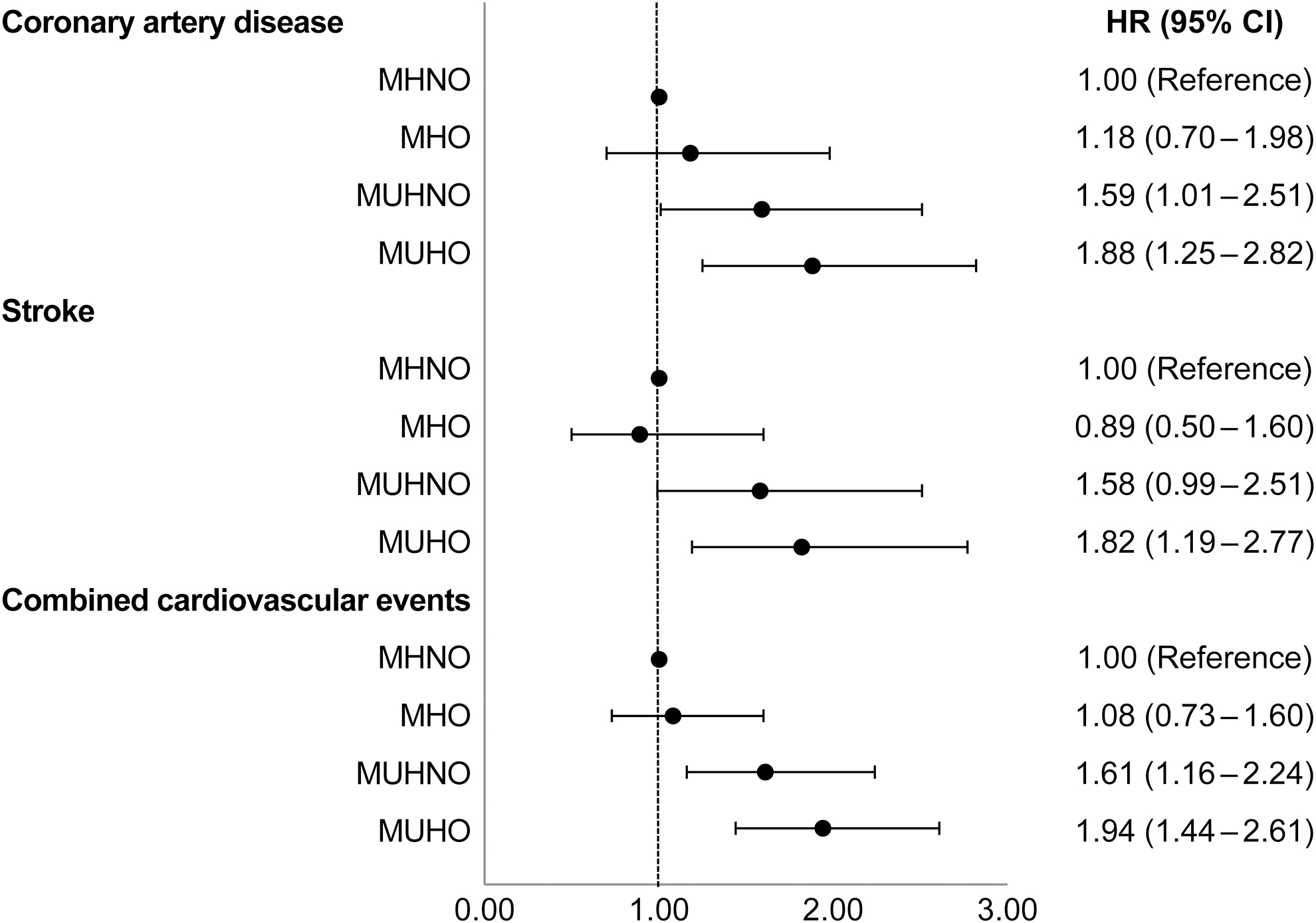
Forest plot of HRs with 95% CIs for incident coronary artery disease, stroke, and combined cardiovascular events according to four metabolic obesity phenotypes. CI, confidence interval; HR, hazard ratio.
Table 3 presents the multivariate Cox proportional hazards regression analysis results for incident coronary artery disease or stroke according to the four metabolic obesity phenotypes. Model 1 was adjusted for age and sex; model 2 for age, sex, and lifestyle behaviors (smoking, alcohol consumption, exercise); and model 3 for age, sex, lifestyle behaviors, and socioeconomic status (residential area, household income, educational level). After adjusting for potential confounding variables, the HRs (95% CIs) for incident coronary artery disease [1.75 (1.15–2.67)], stroke [1.67 (1.09–2.58)], and combined cardiovascular events [1.81 (1.34–2.46)] in the MUHO group were significantly higher than those in the MHNO group. In contrast, the HRs (95% CIs) for incident combined cardiovascular events in the MUHNO group [1.29 (0.92–1.81)] and MHO group [1.21 (0.81–1.79)], after adjusting for potential confounding variables, were not significantly higher than those in the MHNO group.
Hazard Ratios and 95% Confidence Intervals for Incident Coronary Artery Disease and Stroke According to the Four Metabolic Obesity Phenotypes
Model 1: adjusted for age and sex.
Model 2: adjusted for age, sex, smoking, alcohol consumption, and exercise.
Model 3: adjusted for age, sex, smoking, alcohol consumption, exercise, residential area, household income, and educational level.
Supplementary Table S2 presents the multivariate Cox proportional hazards regression analysis results for incident coronary artery disease or stroke separately in men and women across the four metabolic obesity phenotypes.
Discussion
The present study revealed that the four distinct metabolic obesity phenotypes posed different risks for incident coronary artery disease, stroke, and combined cardiovascular events in the large-scale, community population-based, prospective Korean cohort observed for >10 years. The MUHO group had a substantially higher risk for incident coronary artery disease, stroke, and combined cardiovascular events than the MHNO group. In addition, the cumulative incidence of combined cardiovascular events showed a higher tendency in the order of MUHO, MUHNO, MHO, and MHNO. Nevertheless, after adjusting for potential confounding variables, the HRs for incident combined cardiovascular events in the MUHNO and MHO groups were not significantly higher than those in the MHNO group.
Variations in cardiovascular event HRs among the four metabolic obesity phenotypes were observed due to differences in participant ethnicity/race across studies. A previous study involving participants from the United Kingdom reported that MUHO [HR: 1.71 (95% CI: 1.62–1.79)], MUHNO [HR: 1.55 (95% CI: 1.48–1.62)], and MHO [HR: 1.18 (95% CI: 1.10–1.27)] posed a higher risk of cardiovascular events than MHNO. 13 Kammerlander et al. analyzed 4381 participants with stable chest pain from the United States and found that MUHNO [HR: 1.61 (95% CI: 1.02–2.53)], but not MUHO [HR: 1.06 (95% CI: 0.66–1.72)] or MHO [HR: 1.06 (95% CI: 0.62–1.82)], posed a higher risk of cardiovascular events than MHNO at a median follow-up of 26 months. 12 These studies were conducted in Western countries where obesity is highly prevalent, highlighting the need to investigate the risk of incident cardiovascular events incurred by the four metabolic obesity phenotypes in various ethnic groups, particularly within the Korean population, which tends to have a relatively low BMI. 16
While previous studies have examined the association between metabolic health status and obesity with cardiovascular events in the Korean population, 17 –19 the current study has distinct strength, which is a large population-based cohort investigation conducted over a relatively long duration, shedding light on the risk of incident cardiovascular events linked to the four metabolic obesity phenotypes in the Korean population. Thus, the present study's findings expand on previous research by providing additional insights into the risk of cardiovascular events posed by the four metabolic obesity phenotypes.
In this study, MUHO, but not MUHNO or MHO, revealed a higher risk of incident coronary artery disease and stroke than MHNO, which differs from the findings of previous studies reporting a higher risk of incident cardiovascular events not only in MUHO but also in MUHNO and MHO, compared with MHNO. 13,20 In addition to racial differences, the differences in the definition of obesity may also contribute to these discrepancies. Notably, most previous studies defined obesity as a BMI of ≥30 kg/m2. In contrast, the present study followed the Asia-Pacific regional guidelines of the World Health Organization and International Obesity Task Force, defining obesity as a BMI of ≥25 kg/m2. 15
After adjusting for potential confounding variables, the HRs for incident cardiovascular events in the MUHNO and MHO groups were not significantly higher than those in the MHNO group; nonetheless, it is undesirable to conclude that the CVD risk incurred by MUHNO and MHO is as low as that posed by MHNO. The cumulative incidence of combined cardiovascular events showed a higher tendency in the order of MUHO, MUHNO, MHO, and MHNO. Therefore, efforts to reduce metabolic risk factors and maintain a nonobese would be necessary to prevent cardiovascular events related to MUHNO, MHO, and MUHO.
Several possible mechanisms could underlie the differential risks observed among the metabolic obesity phenotypes. A previous meta-analysis showed that MHO individuals exhibit higher levels of physical activity, spend less time engaging in sedentary behavior, and possess superior cardiorespiratory fitness compared to MUHO individuals. 19 This suggests that the observed favorable metabolic profile and lower CVD risks in MHO than MUHO could, at least in part, be influenced by these positive lifestyle factors and attributes.
Another important factor to consider is adipose tissue biology. 21 While there may not be a significant difference in the percentage of body fat between individuals with MHO and MUHO when groups are matched based on sex and BMI, 22 –24 marked differences exist in adipose tissue distribution between these two groups. Elevated abdominal fat mass and diminished gluteofemoral fat mass are indicative of the metabolic unhealthy phenotype, while diminished abdominal fat mass and augmented gluteofemoral fat mass are linked to the metabolic healthy phenotype. 25 –27 In addition to adipose tissue distribution and accumulation, adipogenesis, inflammation, and adiponectin are reported to be significant factors influencing MHO and MUHNO phenotypes. 9,21,28
The present study has strength in that we conducted a large population-based cohort study over a relatively long duration. We adjusted for well-known cardiovascular variables, such as age, sex, lifestyle behaviors (smoking, alcohol consumption, and exercise), and socioeconomic status (residential area, household income, and educational level), in the Cox regression analysis to minimize confounding. Therefore, we believe that our findings provide valuable data on the risk of incident cardiovascular events incurred by the four metabolic obesity phenotypes in the Korean population.
Nonetheless, this study has several limitations. First, despite its large population size, it was conducted on a Korean population alone, potentially limiting the generalizability of our findings to other racial/ethnic populations. Second, universally accepted standard definitions of the metabolic unhealthy phenotypes do not exist. However, the definition used in the present study aligns with that of previous studies 29,30 ; besides, the same definition has been used in our own previous study. 11
Third, a significant sample from the baseline population was excluded due to follow-up loss during the cohort study or incomplete follow-up data during the follow-up period, and our cohort lacks mortality data. Thus, selection bias may exist, as there could be differences between the characteristics of participants included in the analyses and those excluded. Further research is needed to confirm the risk of CVD according to the metabolic obesity phenotypes, including mortality data. Fourth, this study only considered the baseline metabolic obesity phenotypes, thus failing to demonstrate the effect of sequential changes in these phenotypes. Therefore, we could not analyze the association between changes in metabolic obesity phenotype and incident cardiovascular events, which significantly limits our study.
Fifth, the presence of incident coronary artery disease and stroke relied on the self-reported questionnaire. Although examiners consistently verified if the participant had obtained a diagnosis of coronary artery disease and stroke from a medical professional and were informed of the specific name of the diagnosis, specific confirmatory tests (such as coronary angiography or computed tomography angiography) conducted at the time of diagnosis could not be checked. In addition, the self-reported questionnaire on medication usage raises concerns about the accuracy of the medication assessment. To address this limitation, future research should consider conducting studies with access to comprehensive medical records or other objective data with long-term follow-up. Finally, residual confounding factors may have persisted, as is typically in any observational study.
Conclusions
This study revealed that the four distinct metabolic obesity phenotypes posed different risks for incident coronary artery disease, stroke, and combined cardiovascular events in the large-scale, community population-based, prospective Korean cohort observed for over 10 years. After adjusting for potential confounders, it was observed that MUHO individuals, but not MUHNO or MHO, showed a higher risk of coronary artery disease and stroke than MHNO. Nonetheless, it is undesirable to conclude that the CVD risk incurred by MUHNO and MHO is as low as that of MHNO. Further studies involving a large number of participants are required.
Footnotes
Acknowledgments
The authors thank Medical Illustration & Design (MID), a part of the Medical Research Support Services of Yonsei University College of Medicine, for providing excellent support with medical illustration.
Data Availability Statement
The datasets used or analyzed during the current study are available from the corresponding author upon reasonable request.
Authors' Contributions
J.-M.P. and J.-W.L. contributed to the study conceptualization. J.-M.P. and D.-H.J. contributed to the methodology. H.S.L. and J.Y. were responsible for the software. J.Y. participated in validation. H.S.L. and J.Y. conducted the formal analysis. J.-M.P. and J.-W.L. were involved in the investigation. D.-H.J. was responsible for resources. H.S.L. and J.Y. performed data curation. J.-M.P. and J.-W.L. wrote the original draft of the article. J.-M.P. and J.-W.L. reviewed and edited the article. H.S.L. was responsible for visualization. J.-W.L. was involved in supervision. D.-H.J. and J.-W.L. contributed to project administration. J.-W.L. was responsible for funding acquisition. All authors read and approved the final article.
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
This research was supported by the Korea Institute of Planning and Evaluation for Technology in Food, Agriculture, and Forestry (iPET) through the High Value-added Food Technology Development Program, funded by the Ministry of Agriculture, Food and Rural Affairs (MAFRA) (321030051HD030). In addition, it received a faculty research grant from Yonsei University College of Medicine (6-2020-0143).
Supplementary Material
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.