
Abstract
Introduction:
This study aims to investigate the combined association between insulin resistance (IR) levels, relative grip strength (RGS), and the incidence of nonalcoholic fatty liver disease (NAFLD), stratified by sex, using longitudinal data.
Methods:
The study included 1702 adult participants aged 51–88 years who completed surveys in both 2013–2014 and during a subsequent follow-up in 2019–2020. NAFLD was assessed using the hepatic steatosis index, and RGS was measured using the JAMA-5030J1 equipment (SAEHAN, Korea). To assess the interaction between RGS and IR levels and their impact on NAFLD risk, we employed a proportional hazards Cox regression model. Hazard ratios (HR) and 95% confidence intervals (95% CI) were calculated for NAFLD incidence.
Results:
After adjusting for various confounding variables, we observed a significant decrease in NAFLD risk in the middle RGS group (HR = 0.70, 95% CI = 0.53–0.93) and high RGS group (HR = 0.31, 95% CI = 0.22–0.44) compared to the low RGS group. In addition, significant sex differences were noted in the relationship between IR, RGS levels, and NAFLD incidence across different groups.
Conclusions:
This study highlights that higher RGS levels are independently associated with a reduced risk of developing NAFLD. Notably, RGS emerges as a predictive indicator for assessing NAFLD risk.
Introduction
Nonalcoholic fatty liver disease (NAFLD) is characterized by the accumulation of abnormal fats in the liver in the absence of other liver diseases. 1 It is a leading cause of liver diseases, associated with chronic conditions such as type 2 diabetes, cardiovascular diseases, hepatitis, cirrhosis, hepatocellular carcinoma, and liver transplantation. Globally, NAFLD prevalence was 29.8% in 2019 and has steadily increased since 1991. 2 In South Korea, the number of NAFLD patients rose from 318,000 in 2018 to 407,000 in 2022. Also, The health care costs related to NAFLD have increased by 1.74 times in 2021 compared to 2018, posing significant national and international financial burdens. Therefore, urgent implementation of effective management strategies to reduce NAFLD prevalence is crucial. 2,3
Increased levels of muscular strength have been identified as a powerful predictor of future health in older adults. 4 Relative grip strength (RGS), which is absolute grip strength (AGS) divided by body mass index (BMI, kg/m2), has been indicated as a more effective measure than AGS alone for assessing muscle weakness, 5 and cardiovascular disease risk. 6 Indeed, muscle strength has been reported as a more critical factor than muscle mass in predicting health outcomes, showing a close association with insulin resistance (IR) and the risk of NAFLD. 7
The association between NAFLD and RGS has been extensively studied, yet previous research has encountered challenges in confirming the independent relationship between muscle strength and NAFLD, primarily due to insufficient consideration of factors such as physical activity levels and co-morbidities other than obesity. 7,8 Furthermore, since many studies have been cross-sectional in nature, 7 –9 there remains a need for future research to elucidate the relationship between RGS and the risk of NAFLD development. 7
Previous studies have suggested that IR may mediate the association between RGS and NAFLD, 7 although they have not definitively established the risk of NAFLD occurrence based on the interaction between RGS and IR. Therefore, this study aims to investigate the relationship between RGS levels, the risk of IR, and the incidence of NAFLD After adjusting for various confounders [age, sex, sleep time, estimated glomerular filtration rate (eGFR), high sensitivity C-reactive protein (hs-CRP), lean body mass, alcohol intake, smoking status, IR, exercise participation, diabetes, hypertension]. In addition, we aim to explore gender differences and examine how the interaction between IR and RGS levels influences the risk of NAFLD development.
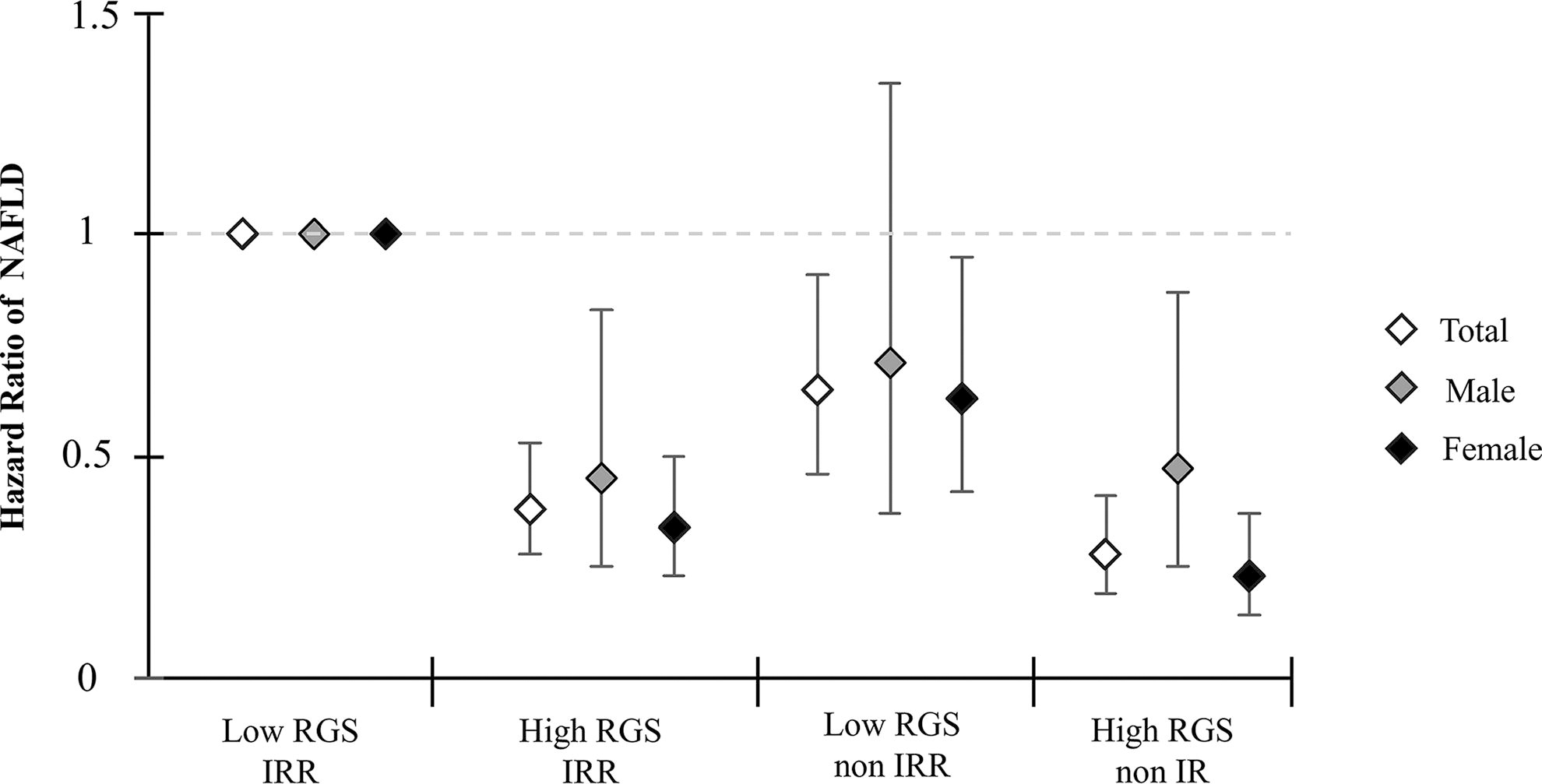
Hazard ratio of NAFLD according to joint association RGS level and IRR by sex. Multivariable adjusted age, sex, sleep time, eGFR, hs-CRP, lean body mass, alcohol intake, smoking status, HOMA-IR, exercise participation, diabetes, and hypertension. eGFR, estimated glomerular filtration rate; HOMA-IR, homeostatic model assessment for insulin resistance; hs-CRP, high sensitivity C-reactive protein; IRR, insulin resistance risk; NAFLD, nonalcoholic fatty liver disease; RGS, relative grip strength.
Methods
Study design and population
This study utilized data from the Korean Genome and Epidemiology Study. Participants aged 51–88 years, who were selected from Anseong, Gyeonggi Province, South Korea, underwent baseline surveys from 2013 to 2014 and at least two follow-up surveys between 2019 and 2020. Initially, 4192 adults were enrolled. Exclusions included individuals with cardiovascular disease (n = 37), cancer (n = 27), or NAFLD (n = 673) identified during the baseline survey, resulting in 3455 participants. In addition, those exceeding daily alcohol intake guidelines (≥210 grams/day for men, ≥140 grams/day for women) were excluded (n = 729) to mitigate alcohol-related liver damage based on previous studies. 10 Finally, after excluding 1006 participants with missing data on NAFLD and RGS variables, a cohort of 1702 participants with an average follow-up period of 6.50 years was established. This study received approval from the Institutional Review Boards of Korea University Ansan Hospital and Seoul National University, and all participants provided written informed consent (IRB No. E2112/001-009).
Measured variables
IR risk and blood variables measurement
All study participants were instructed to maintain a fasting state of over 8 hr before serum collection for general blood tests. On the day of collection, blood samples were processed onsite using a centrifuge and sent to Seoul Clinical Laboratory. Utilizing the ADVIA 1800 auto-analyzer (Siemens, USA), we analyzed blood glucose, glycated hemoglobin (HbA1c), hs-CRP, serum creatinine, insulin, aspartate aminotransferase (AST), and alanine aminotransferase (ALT) to gather research data. Serum samples obtained from these tests were uniformly stored by the Genomics Research Team at the Korea Centers for Disease Control and Prevention. The eGFR was calculated using the modification of diet in renal disease study formula 11 based on serum creatinine, a method established in previous studies [in mL/min per 1.73 m2 = 175 × SCr–1.154 × age–0.203 × (0.742 if female)]. Homeostatic model assessment for insulin resistance (HOMA-IR) values 12 were determined using the formula (fasting insulin × fasting blood glucose/405) from previous research. IR risk was assessed based on prior studies correlating IR with lower limb strength, with HOMA-IR values ≥1.73 indicating IR risk. 13
Questionnaire and other variables
BMI was calculated using the formula weight (kg)/height2 (m2), based on height (cm) and weight (kg) measurements. Muscle mass was assessed using data from the Zeus 9.9 device (JAWON Medical, Korea). Surveys were conducted via one-on-one interviews by investigators, ensuring completeness through immediate review and revision postsurvey. Alcohol consumption was categorized as “no alcohol experience” if respondents answered “yes” to “Do you originally not drink alcohol or have you never drunk alcohol?” Additional questions were posed for those answering “no” regarding current drinking habits. Responses were classified as “past drinking” for “no” and “current drinking” for “yes.” Current smoking status was determined by responses to questions about lifetime cigarette consumption. “No smoking experience” applied if respondents had smoked more than 5 packs (100 cigarettes) in their lifetime and answered “yes,” with additional questions asked for “no” responses regarding current smoking habits. Responses were categorized as “past smoking” for “no” and “current smoking” for “yes.” Sleep duration was calculated as [(weekday sleep hours*5) + (weekend sleep hours*2)]/7, based on participant responses regarding their average hours of sleep on weekdays and usual bedtime on weekends over the past month. This measure was employed as a continuous variable in our analysis. Physical activity participation was categorized by responses to the question “Do you regularly engage in vigorous exercise that induces sweating?” Participants answering “no” were classified as “no regular exercise,” while those answering “yes” were categorized as “regular exercise participants.” Hypertension status was determined using established criteria 14,15 : systolic blood pressure ≥140 mmHg, diastolic blood pressure ≥90 mmHg, self-reported hypertension diagnosis, or current use of antihypertensive medication, categorized as “hypertension.” Diabetes status 16,17 was ascertained if fasting blood glucose was ≥126 mg/dL, HbA1c was ≥6.5%, or if participants reported a prior diabetes diagnosis or current use of oral diabetes medication, categorized as “diabetes.”
RGS measurement
Grip strength was measured in kilograms using the JAMA 5030J1 device (SAEHAN, Korea). Participants sat in a chair with their arms positioned at a 90-degree angle, completing three grips with each hand, and the average strength was recorded for both sides. In this study, RGS was determined by dividing AGS by BMI, a method supported by previous research highlighting its predictive value for chronic diseases. 16 RGS was stratified into “low,” “middle,” and “high” tertiles by gender for analysis. Furthermore, to examine interactions between RGS and IR risk, we categorized RGS by gender into “low” and “high,” and IR risk into “non-IR risk” and “IR risk,” analyzing them as “low RGS/IR risk,” “high RGS/IR risk,” “low RGS/non-IR risk,” and “high RGS/non-IR risk.”
Diagnosis of NAFLD
In accordance with previous studies demonstrating an inverse association between muscle strength and NAFLD, 18 NAFLD diagnosis relied on the hepatic steatosis index (HSI) with a specificity of 93.1%. HSI was calculated using the formula [8 * ALT/AST] + BMI [+ if DM; + if female]. Participants were categorized as “NAFLD” if their HSI score exceeded 36 points and as “non-NAFLD” if it was 36 points or below. 19
Statistical analysis
In this study, data analysis was conducted using STATA/IC 14.1 (STATA Corp., College Station, TX, USA). Descriptive analysis, which included chi-square tests and calculation of means, was performed to examine the demographic characteristics of the participants. Variables were presented as percentages or means with standard deviations. To calculate the incidence density of NAFLD risk among participants under observation, we calculated person-years across the entire follow-up period. Log-rank tests were conducted to establish the analytical model for evaluating the relationship between RGS, insulin resistance risk (IRR), and NAFLD incidence. Significant differences in NAFLD incidence rates were observed across RGS levels (p = 0.0001) and IRR levels (p < 0.001). Assuming proportional hazards in our study, we used Cox proportional hazards regression models to independently assess hazard ratios (HR) and 95% confidence intervals (95% CI) for NAFLD incidence, stratified by gender-specific RGS and IRR levels. In addition, we explored the interaction between gender-specific IR risk levels and RGS in relation to NAFLD, calculating HR and 95% CI using Cox regression models. Our analysis using the proportional hazards Cox regression model adjusted for confounding variables such as age, sex, regular exercise participation, skeletal muscle mass, eGFR, hs-CRP, alcohol consumption, smoking status, HOMA-IR, diabetes status, and hypertension status, which may influence NAFLD incidence and RGS. All significance levels were set at p < 0.05.
Results
The demographic characteristics of this study are detailed as follows (Table 1): a total of 1702 participants, including 682 males (mean age, 66.28 ± 8.00 years) and 1020 females (mean age, 66.56 ± 8.63 years). Among males, the high RGS group, compared to the low RGS group, was characterized by higher RGS, younger age, higher lean body mass, higher eGFR, lower levels of hs-CRP, lower rates of diabetes and hypertension, higher rates of current alcohol consumption and smoking, and increased participation in regular exercise. Among females, the high RGS group, compared to the low RGS group, was characterized by higher RGS, younger age, higher lean body mass, higher eGFR, lower HOMA-IR, lower rates of diabetes and hypertension, higher rates of current alcohol consumption, and increased participation in regular exercise. Significant demographic differences between males and females were observed in RGS, sleep time, lean body mass, hs-CRP, HOMA-IR, hypertension, smoking status, alcohol consumption, and regular exercise participation, while no significant differences were found in age, eGFR, and diabetes.
Baseline Characteristics of Study Participants by Relative Grip Strength by Sex
Significant difference in male and female:
<0.05.
<0.01.
<0.001.
BMI, body mass index; eGFR, estimated glomerular filtration rate; HOMA-IR, homeostatic model assessment for insulin resistance; hs-CRP, high sensitivity C-reactive protein; IRR, insulin resistance risk; RGS, relative grip strength.
The results pertaining to the association between gender-specific RGS levels, IR risk, and the risk of NAFLD incidence are presented in our study (Table 2). The incidence density per 1000 person-years varied across RGS levels (low RGS = 36.97, high RGS = 22.38). After adjusting for various confounders, both the middle and high RGS groups exhibited a substantial reduction in NAFLD incidence compared to the low RGS group, HR decreasing by 30% (HR = 0.70, 95% CI = 0.53–0.93) and 69% (HR = 0.31, 95% CI = 0.22–0.44), respectively. Furthermore, a significant decreasing trend in NAFLD incidence HR with increasing RGS levels was observed (p-trend <0.001). Similar patterns were seen among females compared to all participants, with HR of 0.65 (95% CI = 0.46–0.92) for middle RGS and 0.31 (95% CI = 0.20–0.47) for high RGS, both in comparison to the low RGS group. Among males, significant associations were observed solely between the high RGS group and NAFLD incidence HR (HR = 0.32, 95% CI = 0.17–0.61). In addition, the findings regarding the association between IR risk and NAFLD incidence risk revealed that across all participants (HR = 2.78, 95% CI = 1.98–3.91), males (HR = 2.49, 95% CI = 1.25–4.99), and females (HR = 2.84, 95% CI = 1.91–4.21), individuals with IR risk faced more than twice the risk of NAFLD incidence compared to those without IR risk.
Incidence Density and Hazard Ratio of NAFLD according to Relative Grip Strength and Insulin Resistance by Sex
Multivariable adjusted age, sex, sleep time, eGFR, hs-CRP, lean body mass, alcohol intake, smoking status, HOMA-IR, exercise participation, diabetes, and hypertension.
Incidence density = case/person-year × 1000.
CI, confidence intervals; NAFLD, nonalcoholic fatty liver disease.
The association between gender-specific RGS and IR risk interaction with NAFLD incidence is detailed in our study (Table 3 and Fig. 1). We found that the high RGS/IR risk group (HR = 0.38, 95% CI = 0.28–0.53), low RGS/non-IR risk group (HR = 0.65, 95% CI = 0.46–0.91), and high RGS/non-IR risk group (HR = 0.28, 95% CI = 0.19–0.41) significantly reduced NAFLD incidence HR compared to the low RGS/IR risk group. Among females, the high RGS/IR risk group (HR = 0.34, 95% CI = 0.23–0.50), low RGS/non-IR risk group (HR = 0.63, 95% CI = 0.42–0.95), and high RGS/non-IR risk group (HR = 0.23, 95% CI = 0.14–0.37) significantly reduced NAFLD incidence HR compared to the low RGS/IR risk group. However, among males, no significant association was found between the low RGS/non-IR risk group and HR of NAFLD incidence (p = 0.297). Notably, the high RGS/non-IR risk group exhibited the most pronounced reduction in HR of NAFLD incidence among all groups.
Hazard Ratio of NAFLD According to Joint Association Between Relative Grip Strength and Risk of Insulin Resistance by Sex
Multivariable adjusted age, sex, sleep time, eGFR, hs-CRP, lean body mass, alcohol intake, smoking status, HOMA-IR, exercise participation, diabetes, and hypertension.
Discussion
In this study, middle and high RGS levels significantly reduced the risk of NAFLD compared to low RGS levels among all participants and females. But among males, significant associations with reduced NAFLD incidence compared to low RGS levels were found only in the high RGS group. In addition, IR risk increased the risk of NAFLD incidence compared to non-IR risk among all participants. When comparing the low RGS/IR risk group with the high RGS/IR risk, low RGS/non-IR risk, and high RGS/non-IR risk groups, we found that all these groups reduced the risk of NAFLD incidence among all participants and females, but among males, significant associations with NAFLD incidence risk were found only in the low RGS/non-IRR group.
AGS is considered a convenient and suitable method for assessing the overall neuromuscular system in elderly individuals. 20 It is associated with maintaining skeletal muscle mass, which in turn reduces the incidence of various diseases. 21 AGS has been reported to closely correlate with mobility, functional status, and mortality rates in older adults independently of muscle mass. 20,22 RGS, specifically, is known as a predictive measure for muscle loss due to declining functional capacity. 22 Previous studies 9 on the association between NAFLD and RGS among Americans found that higher RGS independently correlated inversely with NAFLD (OR = 0.41, 95% CI = 0.28–0.60). This association was observed only in physically active individuals (OR = 0.31, 95% CI = 0.16–0.60), while no significant association was found in inactive individuals. 9 Another study 7 demonstrated that lower RGS increased the risk of NAFLD (OR = 3.62, 95% CI = 3.25–4.03), whereas increasing RGS reduced the prevalence of NAFLD by 24% (OR = 0.76, 95% CI = 0.68–0.82). These findings suggest that the relationship between these variables is mediated by IR. 7
The association between RGS levels and NAFLD remains challenging to explain mechanistically, but reduced RGS is associated with impaired physical function, indicating a close link with increased NAFLD risk due to decreased physical activity. 23,24 In this study, the high RGS group exhibited significantly higher rates of regular physical activity compared to the low RGS group: 1.61 times higher in males (44.74 vs. 27.75) and 2.04 times higher in females (37.24 vs. 18.24). This observation is consistent with prior research suggesting that the relationship between NAFLD and RGS is influenced by levels of physical activity. 9 Therefore, high RGS levels indicate a physically active status, 11 implying that maintaining high RGS levels through regular physical activity may mitigate the risk of NAFLD. 9
In our study, the stronger association between RGS levels and NAFLD in women compared to men is attributed to greater use of upper body muscles. Previous studies indicate that both men and women exhibit varying muscle strength levels regardless of body size, influenced more by their activity levels, particularly in upper body strength, which is more responsive to physical activity than lower body strength. 25
Comparing changes in RGS over 10 years among middle-aged adults, the results suggest that male experience a more pronounced decline in RGS compared to female, possibly due to female engaging more in household chores than male 26 Studies also note that female experience relatively less decline in muscle quality (MQ) in upper body muscles, reflecting age-related reductions in RGS compared to male. 27 Therefore, given that higher levels of upper body activity delay age-related declines in RGS and offer additional health benefits for female, 26 it is suggested that RGS may more effectively predict disease risks such as NAFLD in women compared to male. 9,27
The reason why higher RGS has a greater impact on reducing the risk of NAFLD compared to low IR levels is because RGS decreases IR, which directly affects NAFLD. Previous studies 28 suggest that groups with low MQ tend to accumulate excessive intramuscular fat due to obesity, despite having relatively heavier weight, while groups with high MQ can produce good muscle strength despite having low muscle mass. Therefore, increasing RGS is associated with reducing IR independently of body weight. 28 Muscles play a key role in stimulating insulin and facilitating blood glucose removal, thereby improving IR and enhancing glucose transport capabilities. 29,30 Consequently, decreased muscle mass and strength may increase IR 29 through hepatic fat accumulation and heightened inflammatory responses, potentially contributing to NAFLD. 24 Thus, maintaining high RGS through regular muscle contractions can positively impact IR, thereby indirectly reducing the risk of NAFLD. 24
The reason why higher RGS levels in male specifically reduce the risk of NAFLD incidence is believed to be more effective due to their impact on decreasing inflammatory substances influenced by higher levels of intramuscular fat compared to female. Muscle strength and NAFLD are closely associated with chronic inflammation, 11,31 and other studies indicate that muscle strength may affect NAFLD risk through the inflammatory marker hs-CRP. 32
In this study, male was found to have significantly higher intramuscular fat and RGS levels than female. With increasing RGS levels in male, hs-CRP levels decreased significantly, whereas no significant difference was observed in female. Previous research suggests that high RGS is indicative of greater muscle mass, 33 which could potentially improve inflammatory processes associated with adipocytes and lower hs-CRP levels. 34 Therefore, higher muscle strength levels may release various myokines into the bloodstream through vigorous skeletal muscle contractions, potentially reducing inflammatory cytokines via anti-inflammatory mechanisms. 35 Consequently, it is suggested that higher RGS levels in male due to greater lean body mass 33 might lower inflammatory cytokine levels, thereby contributing to reduced IR 36 and a decreased risk of NAFLD 31 compared to female.
This longitudinal study compared and verified the association between RGS levels, IRR, and the risk of NAFLD incidence. However, it has several limitations. First, as we diagnosed NAFLD using the HSI formula, direct confirmation of hepatic fat accumulation was not possible. Second, our examination focused solely on the relationship between RGS, an upper body strength indicator, and NAFLD risk. We did not assess NAFLD risk based on strength levels in other areas like the abdomen.
Conclusions
In this study, an increase in both low IR levels and high RGS significantly reduced the risk of developing NAFLD in both males and females. In addition, the study highlighted that enhancing RGS or improving IR is associated with a decreased risk of developing NAFLD, suggesting that increasing RGS may be more crucial than improving IR. Therefore, there is a pressing need to promote national programs aimed at reducing body fat and boosting muscle strength to maintain high RGS levels and mitigate NAFLD risk.
Footnotes
Authors' Contribution
Study concept and design: D.P. and O.L.; acquisition of data: D.P.; analysis and interpretation of data: D.P. and B.L.; drafting of the manuscript: D.P. and O.L.; critical revision of the manuscript: D.P. and O.L.; administrative, technical, or material support: O.L.; statistical analysis: D.P. and O.L.; and study supervision: D.P. and O.L.
Author Disclosure Statement
The authors declare that there are no conflicts of interest regarding the publication of this article.
Funding Information
Data in this study were from the KoGES (6635-302), National Institute of Health, Korea Disease Control and Prevention Agency, Republic of Korea.