
Abstract
Chronic subdural hematoma (CSH) is a disease frequently seen in the neurosurgical department. CSH also has a high rate of recurrence. Our hypothesis is that thrombin solution irrigation reduces recurrence in high-risk CSH patients. We define high risk as follows: use of anti-platelets, use of anticoagulants, recurrent CSH, renal failure, liver cirrhosis, and hematological disease. From January 1, 1998, to March 31, 2008, we compared a saline solution irrigation group (43 patients) and a thrombin solution (100 unit/ml) irrigation group (36 patients) prospectively and randomly. Surgical procedures were the same: one burr hole craniostomy, drainage of hematoma, irrigation of cavity, frontal insertion of silicon tube, replacement of air with solution, and removal of tube at 24 h after surgery. We define recurrence as an additional drainage operation due to neurological deficit within six months of surgery. Recurrences of CSH arose in two patients (5.5%) with thrombin irrigation and in 11 patients (25.6%) with saline irrigation (p < 0.05). Saline irrigation patients with anti-platelet medication experienced recurrence in five of 19 patients, although no thrombin-irrigated side recurred with the same drug. No complication occurred in relation to thrombin irrigation. Irrigation of CSH with thrombin solution is an effective treatment option for high-risk cases of CSH without complication.
Introduction
C
Hematoma in CSH stems from the sinusoidal vessels of the capsule or the inner trabecula of the hematoma cavity. Many authors have reported that hyperfibrinolysis in CSH causes continuous bleeding from the capsule of a CSH (Ito et al., 1976; Kawakami et al., 1989; Nomura et al., 1994; Saito et al., 1989). Murakami et al. (2002) reported that endothelial cells of the sinusoidal vessel showed positive reactivity for thrombomodulin, a receptor of thrombin.
From this evidence, we postulate that thrombin induces a hemostatic reaction in the sinusoidal vessels situated in the capsule. We prospectively and randomly irrigated the CSH cavity with thrombin solution to reduce recurrence in high-risk CSH cases.
Methods
This project was approved by the ethics committee of the Hirosaki University School of Medicine. We acquired written, informed consent from patients and/or families. According to previous reports, we defined CSH risk factors as the use of anticoagulants, anti-platelets, coagulopathy (hematological disease, chronic renal failure, liver cirrhosis), and recurrent CSH (El-Kadi et al., 2000; Konig et al., 2003; Mori et al., 2001; Reymond et al., 1992).
From January 1, 1998, to March 31, 2008, we operated on 297 patients (377 sides) with CSH in our department. Seventy-nine patients (97 sides) fulfilled the definition of high-risk CSH. After the patient and/or family agreed to our written informed consent for the study, we randomly selected the saline solution or thrombin solution by coin toss. Thirty-six patients were irrigated with thrombin solution (thrombin group), while 43 patients were irrigated with saline (saline group; Table 1). The thrombin group included 26 men and 10 women; mean age of this group was 70.5 (95% confidence interval [CI] was 66.9–74.1) years. The saline treatment group included 36 men and seven women; mean age of this group was 74.1 (95% CI 70.8–77.4) years. No patient had a ventriculo-peritoneal shunt. Pediatric patients younger than 18 years were excluded from this study (Table 1).
There is no statistical significance between the two groups as to sex distribution, age, number of bilateral cases, volume of hematoma, or risk factors.
CI, confidence interval.
We did not interrupt anti-platelet medication. Anticoagulant medication (i.e., warfarin), however, was reversed by trans-venous infusion of vitamin K according to the value of the prothrombin time international normalized ratio (INR). We operated on the CSH after the INR reached normal value.
Volume of CSH was calculated using the XYZ/2 method (Gebel et al., 1998; Kwak et al., 1983; Sucu et al., 2005). Brain atrophy was classified into four grades: none, mild, moderate, and severe (Amirjamshidi et al., 2007; Oishi et al., 2001; Rasquin et al., 2004). Three of the authors (N.S., Y.O., M.N.) separately diagnosed brain atrophy on day 7 post-operative computed tomography (CT), and a consensus discussion was held.
Surgical procedures were as follows: We perforated the cranium at the thickest part of the CSH. After incision of dura mater, a silicon drainage tube (Create Medic Co., Yokohama, Japan) was inserted into the hematoma cavity, and irrigation was then done. A drainage tube was reinserted in the direction of the frontal tuber (Fig. 1), and we replaced air with irrigation solution after skin suture for prevention of recurrence (Nakaguchi et al., 2000; Okada et al., 2002; Wakai et al., 1990). In the saline group, we used warm sterile saline only. In the thrombin group, thrombin solution was used, diluted with sterile saline (100 unit/ml). We used 200 ml of solution for one-sided irrigation. A drainage tube was connected to a closed system. The drainage tube was removed very carefully about 24 h after the operation, avoiding the introduction of air into the CSH cavity. We also did drip infusion of 2 g tranexamic acid per 24 h trans-venously. Resumption of warfarin started 2 days after surgery.
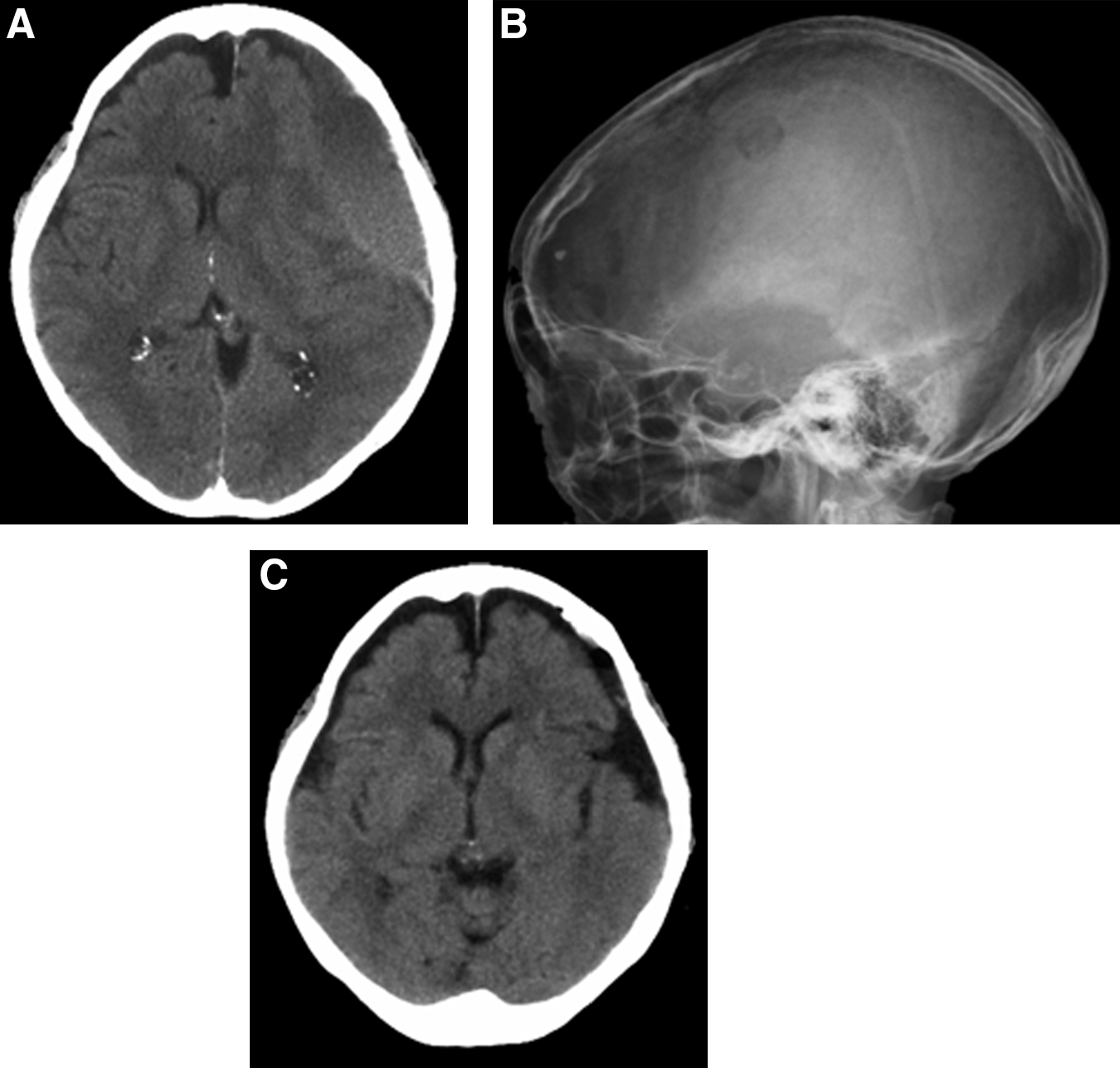
Eighty-three-year old woman with liver cirrhosis who was treated with thrombin solution. (
We took routine brain CTs 1, 7, 30, 90, and 180 days after the operation. If an additional neurological deficit due to CSH occurred, follow-up surgery was done. We defined recurrence as follow-up surgery.
Statistical analysis
We compared the two groups for patient characteristics and recurrence rate of CSH (paired t-test or Fisher exact test). Statistical calculation was done with JMP 8.0, and a p-value below 0.05 was accepted as statistically significant.
Results
In the saline treatment group, the age and number of bilateral cases were higher than those of the thrombin treatment group. But those differences were not statistically significant (Table 1). Differences of volume of hematoma and degree of brain atrophy in both groups were not significant (Table 2). Risk factors of two groups were also similar.
There is no significant change between the two groups.
The recurrence rate for the thrombin group was 5.5% (CSH recurred in two patients) and that of the saline group was 25.6% (CSH recurred in 11 patients; Table 3). Recurrence risk reduction was 20%, and this amelioration was statistically significant (p < 0.05: Fisher exact test). In bilateral cases of CSH, the thrombin treatment group did not experience recurrence (n = 6), but three out of 12 cases in saline treatment group had recurring CSH. In patients medicated with anti-platelets, the thrombin group (n = 15) showed no recurrence, but the saline group experienced recurrence in five of 19 patients (26.3%). Other risk factors did not influence CSH surgical results statistically.
The recurrence rate for the saline solution group is statistically greater than for the thrombin solution group (Fisher exact test, *p < 0.05).
CI, confidence interval; CSH, chronic subdural hematoma.
Discussion
Our results with thrombin solution irrigation for cases of high-risk CSH are encouraging. We found no prospective report focusing on solution treatment methods for high-risk CSH. Thrombin solution is effective in reducing recurrence of high-risk CSH, especially in patients medicated with anti-platelets. During the same study periods, we operated on 258 adult CSH patients (331 sides) with pure saline irrigation. Twenty-six patients (30 sides) experienced recurrence. Our overall recurrence rate with saline irrigation treatment is 10.1% based on patient numbers. In high-risk patients, the recurrence rate of CSH in the saline irrigation group was 25.6%. This risk difference was statistically significant (p < 0.05, Fisher exact test). Our definitions of high risk are acceptable.
We did not exchange the thrombin solution with pure saline. The bioactivity of the thrombin used for irrigation in the CSH cavity was permitted to continue until presumed, deactivating combination with antithrombin III (AT3) that oozed from the systematic blood circulation via the hematoma membrane. Usually, a high concentration of a thrombin-AT3 complex (TAT) can be detected in CSH (Suzuki et al., 1998b), but we drained most of the hematoma, so that little AT3 remained in the CSH cavity after the operation. We considered the active mechanism in our results to include thrombin-induced constriction, fibrin deposition, and hemostasis of the sinusoidal vessels of the CSH capsule. Additionally, we used 2 g of tranexamic acid at 2 days post-operative. Combination use of thrombin and tranexamic acid strongly induces a hemostatic reaction. Hemostasis of the CSH capsule, which induces bleeding, was completely achieved in the post-operative acute stage. After an operation, expansion of brain tissue diminishes the CSH cavity. We think post-operative complete hemostasis can prevent late phase recurrence of CSH.
Since anti-platelet drugs cannot be reversed immediately and there was a general bleeding tendency, hemostatic disability was continued into the perioperative period. On the one hand, thrombin solution irrigation was not superior to saline irrigation for patients medicated with anti-coagulants. Prior to surgery, we reversed anti-coagulation using a venous infusion of vitamin K, leading to a preoperative INR in the normal range. We resumed anticoagulants 2 days after surgery. During these periods, hemostasis of the hematoma cavity was completed, so that, in patients medicated with anti-coagulants, there was no significant difference between the two groups. Interruption of anticoagulant medication can induce thromboembolic complications. Kawamata and colleagues reported that one patient with a mechanical aortic valve suffered thrombo-embolic stroke during the interruption of anticoagulant in 27 intracranial hemorrhage patients who were medicated with anticoagulants (Ito et al., 1976; Kawamata et al., 1995). Köning et al. (2003) reported that outcome was significantly worse in the alcoholic group as well as in the recurrent group, but they also pointed out that there was no significant difference between patients with and without anticoagulant treatment. Some authors report that the effectiveness of coagulation factor application for intracranial hemorrhage is related to anti-coagulant medication, but to avoid infection we do not apply coagulation factor to CSH patients (Boulis et al., 1999; König et al., 2003).
Other risk factors—hematological disease, chronic renal failure, liver cirrhosis, and recurrence of previous CSH—demonstrate small differences between the two treatment methods. The number of sides with hematological disease, chronic renal failure, and liver cirrhosis treated surgically is small, and we found no useful results here. The differences in recurrent cases of previous CSH were not significant. In our opinion, this risk factor influenced the high recurrence rate of CSH in both treatment groups with unpredictable causes.
Our surgical procedure is supported by previous reports: irrigation and drainage (Nakaguchi et al., 2000; Okada et al., 2002; Suzuki et al., 1998a; Wakai et al., 1990), frontal insertion of tube (Nakaguchi et al., 2000; Shiomi et al., 2002), and less residual air (Mori et al., 2001; Oishi et al., 2001; Shiomi et al., 2001). One major difference in our procedure is the drainage period. Many authors retained hematoma cavity drainage for 2–4 days (Kiymaz et al., 2007; Nakaguchi et al., 2001; Suzuki et al., 1998a). We removed the drainage tube about 24 h after surgery, but we have not experienced unfavorable results due to short insertion periods. Some authors treated recurrent CSH with a large craniotomy and excision of the external CSH membrane (Tyson et al., 1980), or by conversion of the CSH cavity into the epidural space (Oku et al., 1984). We think such treatment methods are too invasive, especially in patients of advanced age, and thus we chose one-burr-hole surgery for CSH.
This study is prospective and randomized but is merely a single-center trial. A multi-center trial is required to provide further evidence. In addition, for prevention of this disease, we need to investigate CSH patients who are not at high risk.
Footnotes
Author Disclosure Statement
No competing financial interests exist.