
Abstract
The potential for sertraline administered in the first 3 months after moderate to severe traumatic brain injury (TBI) to decrease the incidence of depression in the first year after injury was assessed in a double-blinded randomized control trial. Subjects were enrolled an average of 21 days after injury (none >8 weeks) followed by oral administration of placebo (50 subjects) or sertraline 50 mg (49 subjects) for 3 months. Subjects were not depressed at the time of study initiation. Outcome was assessed using the Hamilton Depression Rating Scale (HDRS) and the Depression Scale of the Neurobehavioral Functioning Inventory (NFI). Based on intent-to-treat and efficacy subset analyses, those receiving placebo exhibited significantly greater depressive symptoms than those receiving sertraline during the first 3 months after injury while receiving placebo/drug (10% of placebo group achieving a score of 6 or greater on the HDRS, 0% of the sertraline group; p < 0.023.). There was no significant difference in depressive symptoms during the remainder of the year between the two groups. Sertraline is effective in diminishing depressive symptoms even among those not clinically depressed while the medication is being taken. However, the results do not support the idea that administration early in recovery diminishes the expression of depressive symptoms after the drug is stopped. There is no basis from this study to assume that sertraline administered early in recovery after TBI, when neurotransmitter functioning is often altered, has ongoing effects on the serotonin system after sertraline is discontinued.
Introduction
D
Factors influencing development of depression after traumatic brain injury
The causes of depression following TBI are a matter of debate, with evidence of a complex interaction among neuroanatomic, neurochemical, and psychosocial factors (Rosenthal et al., 1998). Premorbid risk factors for depression include low pre-injury occupational status (Bowen et al., 1998), poor premorbid social functioning or poverty (Seel et al., 2003), psychiatric difficulties (Federoff et al., 1992), previous brain injury (Federoff, 1992), and substance abuse (Dikmen et al., 2004). Several studies (Gomez-Hernandez et al., 1987; Bowen et al., 1998; Glenn et al., 2001) indicate that gender, race, age, and education do not contribute to severity of depression following TBI, although contrary findings also exist (Seel et al., 2003; Dikmen et al., 2004). Changes in lifestyle and other psychosocial factors after injury may be associated with development and persistence of depression, such as changes in vocational status (Gomez-Hernandez et al., 1997), diminished social contacts (Gomez-Hernandez et al., 1997; Douglas and Spellacy, 2000), and alteration in family roles (Leach et al., 1994).
In terms of injury characteristics, Jorge et al. (2004) report a higher incidence of depression in individuals with TBI than individuals with traumatic injuries of comparable severity without TBI. However, the severity of injury, as measured by Glasgow Coma Scale (GCS) score or duration of post-traumatic amnesia (PTA), has an equivocal association with depression after injury (Gomez-Hernandez et al., 1987; Bowen et al., 1998). In those studies that have detected an effect, it is often found that people with less severe injuries have a higher risk of depression (Glenn et al., 2001; Dikmen et al., 2004).
Role of chronic serotonergic disruption
Alterations in neurotransmitter function have a recognized role in the development and maintenance of depression in the absence of TBI (Belmaker and Agam, 2008). However, there is mounting evidence that TBI can cause disruption of neurotransmitters (including serotonin), which potentially could contribute to the expression of depression. The serotonin system is particularly susceptible to disruption following TBI given that it projects through the basal ganglia and frontal-subcortical white matter (Federoff et al., 1992). There is evidence that TBI impacts levels of serotonin in the central nervous system, but disagreement as to whether there is an elevation or depletion of serotonin in the first hours and days after injury (Markianos et al., 1992; Nayak et al., 1980; Salzman et al., 1987; Sharm et al., 1989; van Woerkom et al., 1990; Karakucuk, 1997). However, a decrease in serotonin level has been documented up to 60 days following TBI (Karakucuk, 1997), suggesting a chronic dampening of the serotonergic system. Animal models further suggest that neuronal synthesis of serotonin may be inhibited even though extracellular levels of the substance may be high (Saran, 1985). There is also evidence that damaged serotonergic neurons can survive an injury and in time re-enervate target regions to reestablish synaptic and neurotransmitter function (Zauner and Bullock, 1996; Whitaker-Azmitia et al., 1990).
A limited body of literature offers tentative support for the use of agents targeting the serotonin system in treating depression following TBI. In mild TBI, Saran (1985) found no benefit of amytriptaline treatment for 4 weeks, although Fann et al. (2000) found an 87% response rate in an 8-week trial of sertraline in a sample of 15 individuals. Among people with severe TBI, Cassidy (1989) described an uncontrolled open trial of fluoxetine with improvement in five of nine patients who were experiencing depression 5–20 months after injury. In a similar descriptive study, Perino et al. (2001) reported significant improvement in a range of mood symptoms after administration of citalopram and carbamazepine for 12 weeks. In another small (10 subjects per group) but more rigorous double-blind placebo-controlled study, Lee et al. (2005) found both methylphenidate and sertraline to improve depressive symptoms relative to placebo.
Prophylactic treatment: rationale and hypotheses
Although the mechanisms underlying development of depression after TBI are multifactorial and not fully understood, the rates of depression and its impact on outcome justify exploration of prophylactic treatment approaches. Addressing early and chronic disruption of the serotonin system is one potential approach. An initial phase I study (Meythaler et al., 2001) examining the potential beneficial impact of serotonin agonists on recovery after TBI indicated that sertraline was safe, although the study may have been limited by a small subject pool (n = 10) and a short duration of treatment with a selective serotonin reuptake inhibitor (SSRI; 2 weeks). This study sought to build on those findings and examine the prophylactic benefit of SSRI administration on development of depressive symptoms after moderate to severe TBI. Theoretically, pharmacological manipulation of neurotransmitter levels, including serotonin, may aid in the repair and reestablishment of useful neural pathways. Thus, there may be a period of time when introduction of serotonin agonist agents might be beneficial to recovery of the normal serotonin response. The present study examines this possibility. Specifically, it is hypothesized that early administration of sertraline will result in a decreased incidence of depressive symptoms in the first year following moderate to severe TBI.
Methods
Subjects
Approval of the Institutional Review Board (IRB) was obtained. Hospital inpatients who received a consult for rehabilitation services following TBI were screened over a span of 3½ years (a total of 371 cases). TBI was determined on the basis of an admission GCS score of 12 or less, or neuroimaging results consistent with the effects of trauma (e.g., contusion, subdural hematoma). Only six individuals had admission GCS scores greater than 12; all had imaging findings positive for subdural hematoma, subarachnoid hemorrhage, and contusion. Inclusion criteria were 19–75 years of age, within 8 weeks of injury, and injury sufficient to require inpatient rehabilitation. Exclusion criteria were existing neurological difficulties, use of antidepressant medication at the time of injury, administration of antidepressant medication in the hospital prior to enrollment, ongoing steroid treatment, depression necessitating treatment at the time of enrollment, pregnancy, alcohol or drug abuse in the year prior to the injury, or systemic medical illnesses that would independently limit outcome (such as severe renal disease and cardiac difficulties). Consent was initially provided by a legally authorized representative followed by assent from the participant at each stage of the study.
Primary outcome measure
Among available depression instruments, the HDRS stands out in the TBI literature and in studies examining depression in psychiatric populations (Snaith, 1996). It has the advantage of being an examiner rating of depressive symptoms and thus is not dependent on a person filling out a questionnaire, which can be difficult depending on cognitive ability following TBI. Among studies in the general population focusing on examiner-rated depressive symptoms, the HDRS is generally the preferred instrument (Snaith, 1996; Faries et al., 2000; Williams 2001). The study utilized a six-item short form of the HDRS (HDRS-6). The HDRS-6 was developed to improve measurement consistency across depression subtypes by focusing on the core symptoms of depression (O'Sullivan et al., 1997) while minimizing sensitivity to somatic morbidity, a common criticism of the HDRS (Linden et al., 1995; Molloer, 2001). The decreased somatic focus of the HDRS-6 is consistent with recommendations of Stein et al. (1996) for assessing depression in patients with behavioral or neurological impairment.
The Structured Clinical Interview for DSM Disorders (SCID-I) was administered as needed based on the results of the HDRS-6. The SCID-I is a semi-structured interview instrument for making DSM-IV diagnoses. The research versions of the SCID-I have enjoyed widespread popularity in clinical research as a means of arriving at reliable and valid psychiatric diagnoses (Williams, 2001; Simon et al., 1993). The SCID-I was administered by trained clinicians in this study. The current study utilized only the modules that assess current and past mood episodes and mood disorders.
Secondary outcome measures
The NFI was administered to study participants and a caregiver during office visits at 3, 6, and 12 months after injury. The NFI (Kreutzer et al., 1999) is a 76-item self-report inventory used to quantify symptoms and behaviors associated with acquired neurological injury. It consists of six factor-analytically derived scales, including one focusing on depression. Separate formats for patient and family were used in this study, with a high degree of demonstrated concordance (Seel et al., 1997). Normative values are available based on age and severity of injury.
Procedure
This is a double-blind placebo-controlled study. The day after consent was obtained the drug/placebo was started and maintained for 3 months. The dose of sertraline was 50 mg and was not changed during the study. This dose was selected as being the lowest dose with possible clinical effects that minimized the potential for unwanted side-effects. Those being discharged were provided with sufficient drug/placebo to last 3 months with instructions for administration. Adherence was evaluated during phone contacts with the study nurse (S.R.). After achieving a level of orientation consistent with resolution of post-traumatic amnesia (Orientation Log score >25), the participant was interviewed weekly while hospitalized regarding symptoms of depression using the HDRS-6. From hospital discharge to 3 months after injury the participant received phone calls every other week from the study nurse to administer the HDRS and assess adherence. At 3–12 months after injury, the participant received monthly phone calls from the study nurse. The participants were asked to return to the rehabilitation hospital 3, 6, and 12 months following injury for a brief neuropsychological evaluation, interview with a neuropsychologist (including administration of the HDRS-6), and family interview. Based on existing literature using the HDRS-6, it was decided to set a score of 8 as the threshold to trigger a formal interview using the SCID-I to establish a diagnosis of depression. If depression was confirmed, the blind was broken for the treating physician, but not for the psychometrician performing the outcome assessments. Appropriate treatment with anti-depressant medication (or a change in treatment) was offered. Counseling was made available at the rehabilitation center or arrangements were made in the community, as dictated by the desires of the participant and family.
Statistical analysis
Recruitment, flow, and retention of participants are depicted in Figure 1. An intent-to-treat analysis was conducted that included all 99 randomized participants. Results were analyzed using chi-squared (χ2). Given that this study examines a prophylactic intervention and there was greater attrition in the treatment group, an intent-to-treat approach may paradoxically be biased toward finding a beneficial effect of treatment (Gross and Fogg, 2004). An efficacy subset analysis, again employing χ2, was thus undertaken using only participants who received the allocated intervention and were not lost to follow-up.
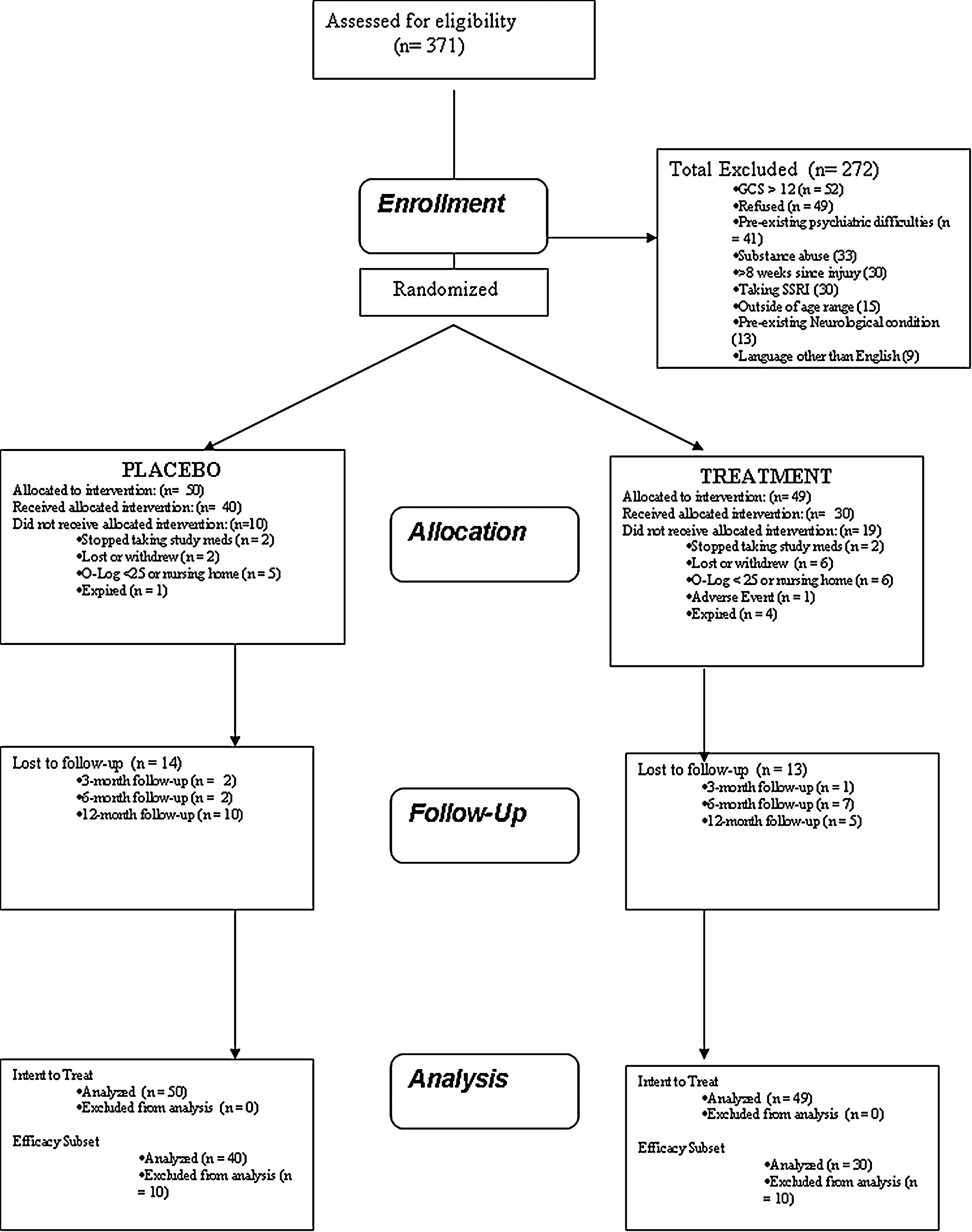
Flow diagram of screening, allocation, and follow-up.
Results
A total of 371 potential participants were screened, resulting in random assignment of 99 participants (49 to treatment, 50 to placebo). Reasons for refusal included concern about being involved in a drug trial, the need to return for follow-up appointments, and the chance of receiving a placebo when the trial medication was readily available clinically. Demographic characteristics of each group are presented in Table 1. All participants were enrolled within 8 weeks of injury, with no significant difference in this regard between groups. No significant between-group differences emerged in terms of age, initial GCS score, education, gender, or marital status at the time of injury. However, it was noted that the treatment group contained a significantly higher proportion of individuals with a GCS score of 3 or 3T (38.8%) than the placebo group (20%), χ2 = 4.2, p = 0.04.
Data missing for seven participants.
GCS, Glasgow Coma Scale; M, mean; SD, standard deviation.
Depression screening
A total of 763 HDRS-6 screenings were completed. Ten participants scored 8 or higher, and were formally diagnosed with depression upon administration of the SCID-I. This overall incidence was below expectation based on existing literature. An examination of the distribution of HDRS-6 scores suggested that an HDRS-6 cutoff of 6 or higher was more consistent with the natural “break” in the distribution. The data were thus analyzed using both criteria, in separate intent-to-treat and efficacy subset analyses.
Intent-to-treat analyses
Of the 49 randomized to treatment, 30 received the allocated intervention. Of the 50 placebo participants, 40 received the allocated intervention (for additional detail, see Fig. 1). Given the nature of the study, it was not possible to have a formal pre-injury depression assessment to carry forward in cases lost before the first formal screening. However, given the efforts to exclude participants with previous psychiatric difficulties, substance abuse, or SSRI treatment, all participants were considered to be non-depressed for the purpose of analysis until depression was identified by formal screenings. Of the 10 participants formally diagnosed with depression in the first year after injury, three were from the treatment group (6.1%), and seven were from the placebo group (14%), χ2 = 1.69, p = 0.19. Time of onset of depression for both groups (in terms of cumulative incidence) is presented in Figure 2. Of note, no cases of depression were identified in the treatment group during the 90-day intervention period, whereas three cases (6%) were identified in the placebo group during this time period, χ2 = 3.03, p = 0.08. For the remainder of the 1-year follow-up period, four cases (8.2%) of depression were identified in the treatment group, and seven in the placebo group (14%), χ2 = 0.133, p = 0.72.
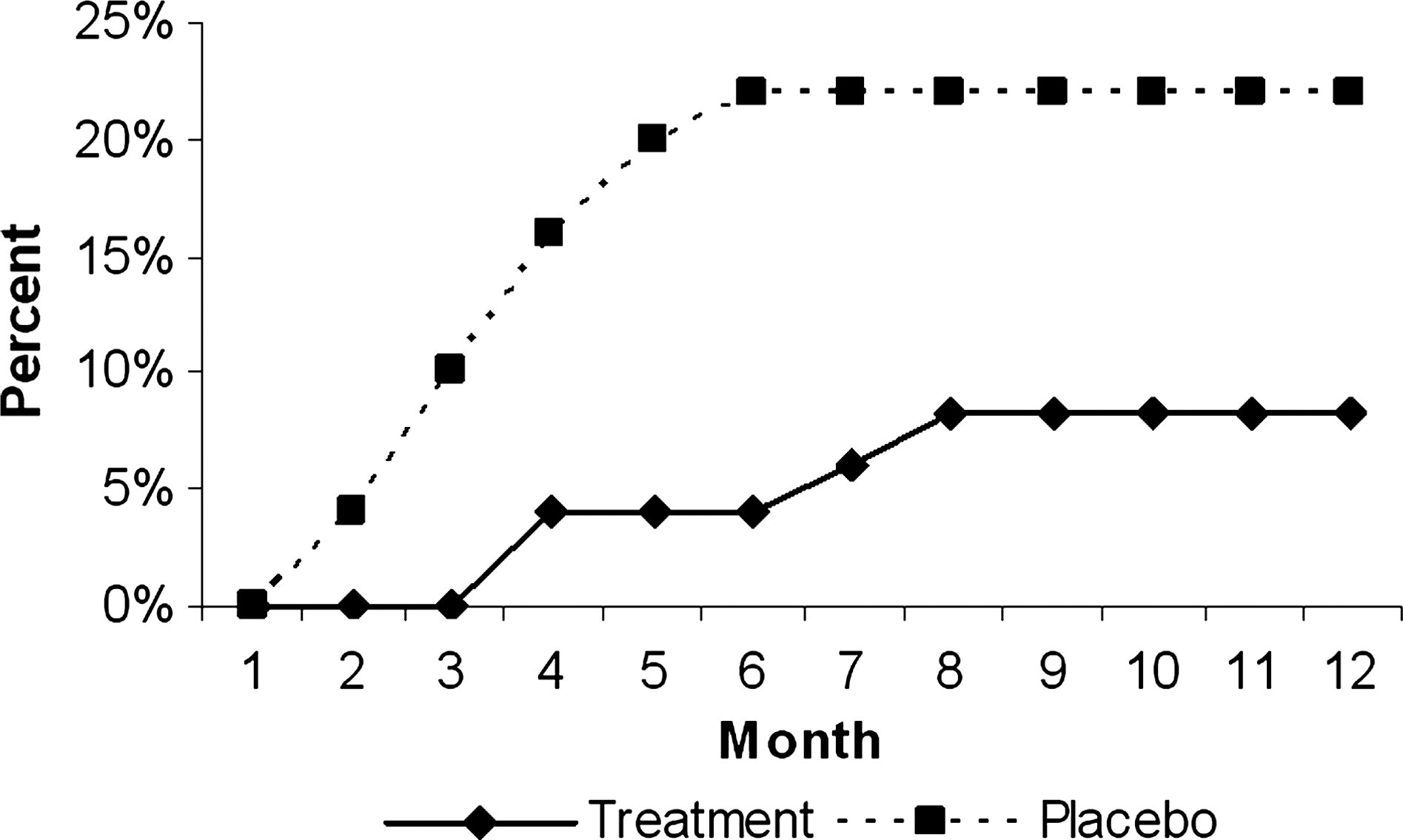
Cumulative incidence of depression (HDRS-6 ≥ 8 plus SCID-I diagnosis). HDRS, Hamilton Depression Rating Scale; SCID, Structured Clinical Interview for DSM Disorders.
A supplemental post hoc intent-to-treat analysis was conducted examining participants who scored 6 or higher on the HDRS-6, the cutoff more consistent with the natural break in the distribution of scores. Of the 15 cases identified by this criterion, four were from the treatment group (8.2%), and 11 were from the placebo group (22%), χ2 = 3.69, p = 0.055. Cumulative incidence was again examined (Fig. 3). No cases were identified during the 90-day intervention period for the treatment group, whereas five cases (10%) were identified for the placebo group in this time period, χ2 = 5.16, p = 0.023. Cumulative incidence for the treatment and placebo groups after the 90-day intervention period (four and six cases, respectively) did not differ significantly.
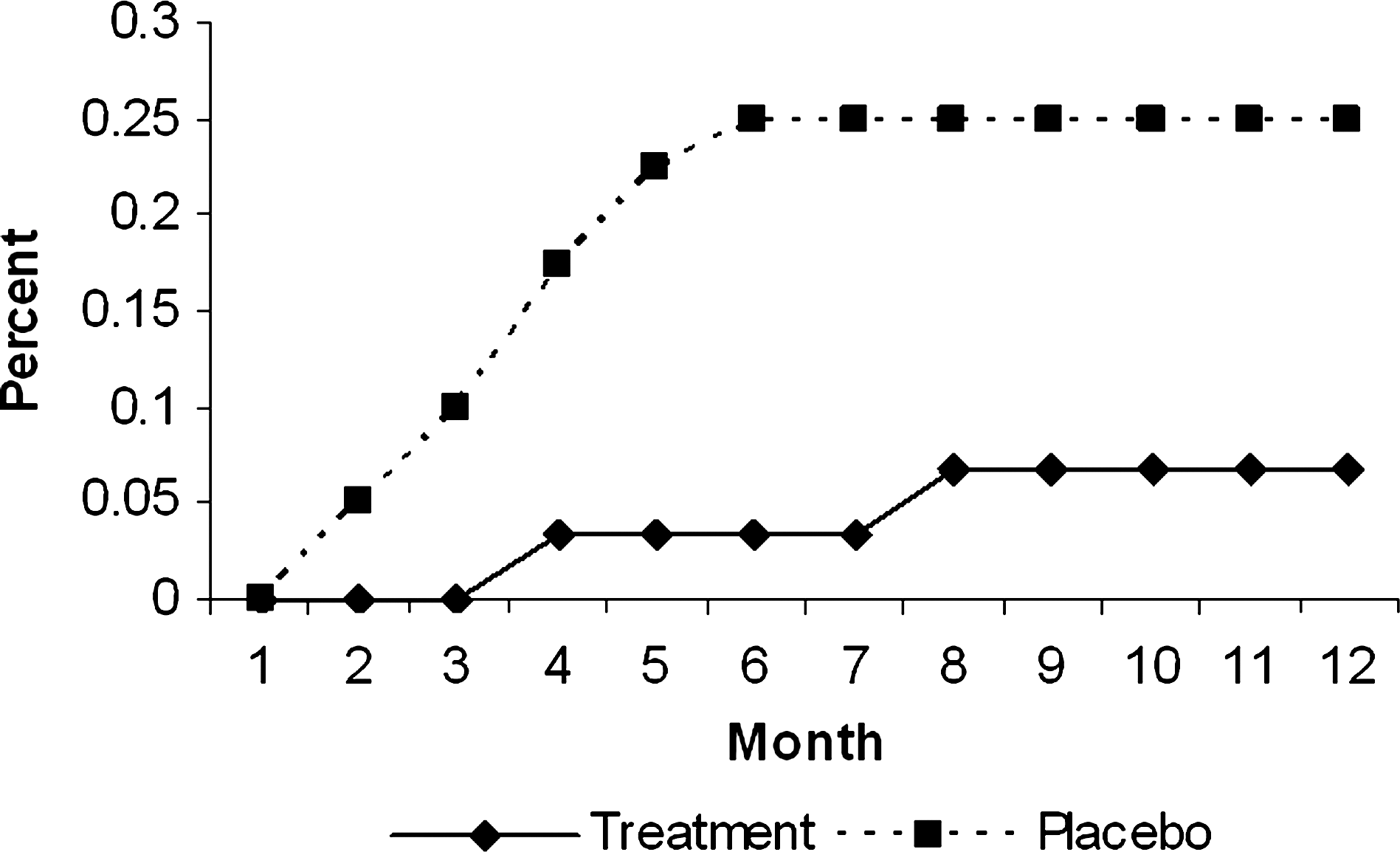
Cumulative incidence of depression (HDRS-6 ≥ 6). HDRS, Hamilton Depression Rating Scale.
Efficacy subset analyses
The efficacy subset included subjects who completed the intervention and participated in follow-up (30 treatment, 40 placebo). Demographic characteristics of each efficacy subset group are presented in Table 2. The groups did not differ significantly in terms of age, initial GCS, or marital status at time of injury, although gender and education approached significance (i.e., slightly higher education and higher proportion of males in the treatment group). The proportion of individuals with a GCS of 3 or 3T remained higher in the treatment group (33.3%) than the placebo group (15%), χ2 = 3.27, p = 0.07. It was noted that in the overall sample, individuals with GCS scores of 3 or 3T were significantly more likely to drop out (44.8%) than those with higher GCS scores (22.9%), χ2 = 4.8, p = 0.03. Dropout occurred most often in the early stages of the study and involved those unable to participate in outcome assessment due to the severity of their disorder. As such, it would appear that the differential dropout rate between groups can be partially attributed to the previously mentioned higher proportion of individuals with a GCS of 3 or 3T in the treatment group, and a greater likelihood of dropout for these individuals.
GCS, Glasgow Coma Scale; M, mean; SD, standard deviation.
The between-groups difference in formal diagnosis of depression across the year (treatment = 6.7%, placebo = 17.5%) remained nonsignificant (χ2 = 1.8, p = 0.18). A supplemental post hoc analysis based on the HDRS-6 ≥ 6 criterion revealed a significant between-groups difference (treatment = 6.7%, placebo = 25%), χ2 = 4.1, p = 0.04. Comparison of onset during the 90-day intervention period revealed a near-significant difference (treatment = 0%, placebo = 10%, χ2 = 3.2, p = 0.07). The difference in case incidence after the 90-day intervention period was not significant (treatment = 6.7%, placebo = 15%).
Finally, depressive symptoms were examined using a secondary outcome measure, the Depression subscale of the NFI. This subscale has the advantage of being a continuous measure that was developed for use in TBI patient populations. It also offers both patient and caregiver report forms. Data for the 3-, 6-, and 12-month follow-ups are presented in Table 3. Consistent with other analyses, the 3-month patient self-report scores (administered at approximately the end of the 90-day intervention period) were significantly lower in the treatment group, although the magnitude of the difference was not great. Significant differences in self-report did not emerge at the 6- or 12-month follow-ups, nor were significant differences found for family report at any of the follow-up points.
NFI
p < 0.05.
NFI, Neurobehavioral Functioning Inventory; M, mean; SD, standard deviation.
Discussion
This study sought to examine the hypothesis that early administration of sertraline would result in a decreased incidence of depressive symptoms in the first year following moderate to severe TBI. It needs to be emphasized that participants in this study were not depressed at the time of enrollment, so the effect on depressive symptoms occurred in a non-depressed sample. Support for the hypothesis was mixed. Significant differences in rates of depressive symptoms across the full year were not found. However, the rate of depressive symptoms in the placebo group was higher during the 90-day treatment period. In fact, using two sets of criteria based on the HDRS-6 yielded no cases of significant depressive symptoms or formal diagnoses of depression in the treatment group during the treatment period. Evidence of a continued benefit beyond the 90-day treatment period was limited. Cumulative development of depressive symptoms remained somewhat lower in the treatment group for the remainder of the year (Figs. 2 and 3). Although this is an interesting observation, small sample sizes and an unexpectedly low rate of depressive symptoms overall preclude firm conclusions in this regard. Although the results suggest prophylactic benefit of sertraline administration early after TBI, this benefit appears to be restricted to the period of medication administration. The results do not strongly support the idea that early administration of an SSRI reverses serotonin depletion in the early stages of TBI recovery in a manner that would confer enduring benefit. Perhaps the strongest conclusion that could be drawn is that any such enduring benefit is modest in magnitude, and much less pronounced than the benefit conferred by active SSRI administration. As such, generalized use of SSRIs such as sertraline for depression prophylaxis after TBI is not strongly indicated, although it may be worth considering in individuals with significant identified risk factors for depression.
The low incidence of depression in this study was surprising given estimates of 10–50% after TBI based on multiple studies. In the present study 10% of the sample developed clinical depression. Even a less conservative criterion (HDRS-6 ≥ 6) resulted in only a 22% rate of depressive symptoms in the placebo group. This did not appear to be a problem with recognizing the symptoms of depression that would lead to a diagnosis of the disorder. Participants were screened regularly and frequently using an established measure of depressive symptoms and interviews took place in person, as well as over the phone, with separate interviewers for each. As a result of these efforts, it appears very unlikely that instances of significant depression were missed among those who responded. In addition, due to concerns that the incidence of depression was less than anticipated, multiple measures of depressive symptoms were employed. The depression subscale of the NFI (for both the participant and caregiver) confirmed the pattern of findings based on the HDRS-6. Also, during the course of the study other measures of depressive symptoms were added to validate the results of the HDRS and NFI. The CES-D (Radloff, 1977) was administered 126 times and PHQ-9 (Kroenke et al., 1999) 26 times. The results from these scales corresponded closely to the results obtainedf from the HRDS-6 and the NIF. So, the low incidence of depressive symptoms and clinical depression noted in this sample appears to be valid.
Although the low rate of depressive symptoms overall tempers interpretation of the findings, the differential dropout rates in the two groups (19 participants in the treatment group, 10 in the placebo group) is also of concern. The overall drop-out rate was frustratingly high, which unfortunately is not unique to this study (Levin et al., 1990; Sherer et al., 2002). If the dropouts were due to development of depression without effective treatment, one would anticipate comparable dropout rates between groups (barring the implausible hypothesis that sertraline caused depression). It is possible that individuals who developed depressive symptoms remained in the study in the hopes of receiving assistance, resulting in greater retention in the placebo group, although it is also possible that development of side effects could have resulted in greater dropout in the treatment group. Causes of dropout could not be confirmed outright because these individuals did not respond to multiple attempts at contact. There is, however, evidence that the relatively higher dropout rate in the treatment group was attributable in significant part to the higher proportion of individuals with admitting GCS scores of 3 or 3T, who in turn were more likely to drop out from the study. As such, the differential dropout does not likely reflect a medication effect (positive or negative). The lack of follow-up data on many of those individuals does, however, temper conclusions and suggest caution in interpreting the data.
The present study has several weaknesses that can be addressed in future studies. The sample size is smaller than intended, although larger than many other studies that have examined the impact of medication on symptoms of depression following TBI. The intended sample size was larger, but it proved difficult to enroll participants for a number of reasons that are not unique to this site. The low dose of sertraline employed in this study may not have been sufficient to impact serotonin levels in the manner predicted by the hypothesis. Providing different dose levels of sertraline was considered, but this would have added another grouping level to the study and thus increased the needed sample size. Moreover, it is difficult to justify administering a dose that is higher than the typical initial clinical dose, considering the use is prophylactic. A prophylactic study offers no criterion by which dose increases (e.g., lack of benefit) could be incorporated. Some consideration should be given to the possibility that administration of sertraline may not have been early enough in recovery to have the desired effect, even though administration began an average of 3 weeks after injury. It could be that initiation of the medication within hours or days after injury is necessary. Although this approach might be feasible in clinical practice, it is difficult to examine in a clinical trial. Enrolling participants in a longitudinal study very early in the course of recovery presents difficulty in terms of outcome measurement. It is impossible to tell in the first few days after injury who will be able to participate in follow-up interviews and testing. Four of the five subjects who died were enrolled while in the neurointensive care unit, as were all of the subjects who proved to be unresponsive and thus unable to participate in follow-up.
Footnotes
Acknowledgments
This project was supported by the National Institute of Disability and Rehabilitation Research Grant H133A980010 Traumatic Brain Injury Model System Project.
Author Disclosure Statement
No competing financial interests exist.