
Abstract
Therapeutic hypothermia remains a promising treatment for patients with severe traumatic brain injury (TBI). Multiple animal studies have suggested that hypothermia is neuroprotective after TBI, but clinical trials have been inconclusive. Systemic hypothermia, the method used in almost all major clinical trials, is limited by the time to target temperature, the depth of hypothermia, and complications, problems that may be solved by selective brain cooling. We evaluated the effects on brain temperature of a cooling device called the ChillerPad,™ which is applied to the dura in a non-human primate TBI model using controlled cortical impact (CCI). The cortical surface was rapidly cooled to approximately 15°C and maintained at that level for 24 h, followed by rewarming over about 10 h. Brain temperatures fell to 34–35°C at a depth of 15 mm at the cortical gray/white matter interface, and to 28–32°C at 10 mm deep. Intracranial pressure was mildly elevated (8–12 mm Hg) after cooling and rewarming, likely due to TBI. Other physiological variables were unchanged. Cooling was rapidly diminished at points distant from the cooling pad. The ChillerPad may be useful for highly localized cooling of the brain in circumstances in which a craniotomy is clinically indicated. However, because of the delay required by the craniotomy, other methods that are more readily available for inducing hypothermia may be used as a bridge between the time of injury to placement of the ChillerPad.
Introduction
Hypothermia remains a promising therapy for TBI despite a lack of conclusive evidence showing efficacy (Schreckinger and Marion, 2009). Preclinical studies have consistently shown unequivocal neuroprotective effects of hypothermia after TBI (Clifton et al., 1991; Clark et al., 1996; Dietrich et al., 1994; Dixon et al., 1998; Yamamoto et al., 1999), but conflicting results have been obtained in clinical trials (Clifton et al., 2001; Jiang et al., 2006a; Marion et al., 1997; Qiu et al., 2005; Shiozaki et al., 2001; Zhi et al., 2003). In a recent meta-analysis of hypothermia after TBI in clinical trials, the authors reported beneficial effects on mortality and neurological outcome, but the results were not statistically significant (Peterson et al., 2008). The authors of another recent review concluded that hypothermia has been shown to be effective for TBI only in low-quality trials (Sydenham et al., 2009). Accordingly, the Brain Trauma Foundation and the American Association of Neurological Surgeons guidelines task force has issued a Level III recommendation for optional and cautious use of hypothermia for adults with TBI.
The failure of the translation of hypothermia from preclinical to clinical trials is likely due to a variety of factors, but those relevant to this study are the time to target temperature and degree and duration of hypothermia. The time to target temperature is a function of the tissue mass being cooled, and the efficiency of the physiological mechanisms resisting cooling. About 4 h is needed to achieve a bladder temperature of 33°C using a combination of iced surface cooling and ice-water gastric lavage (Clifton et al., 2001). The degree of hypothermia that can be used in whole-body cooling is limited by shivering, which occurs at about 36.5°C (Lenhardt et al., 2009), and cardiac dysrthymias, that occur below 32°C (Holzer et al., 2005). Studies suggest that the effectiveness of hypothermia may increase with duration of cooling and greater depth of cooling, yet both are associated with a higher incidence of adverse side effects (Clifton et al., 2009; Polderman et al., 2001). Even mild hypothermia of 35–36°C is associated with increased adverse effects with longer duration of therapy. Potentially serious complications of systemic hypothermia include infection, hypotension, and coagulopathy (Clifton et al., 2001; Hutchison et al., 2008; Rohrer and Natale, 1992; Qiu et al., 2006a; Schwab et al., 2001; Shiozaki et al., 2001; Watts et al., 1998), which may partially or completely offset any benefits, especially in patients with multi-system trauma (Polderman et al., 2001).
The ChillerPad™ (Seacoast Technologies, Portsmouth, NH) was developed to circumvent some of the problems described above, by allowing profound focal cooling of the brain directly over the injured site without whole-body cooling (Nemoto et al., 2006a, 2006b; Wagner and Zuccarello, 2005; Wagner et al., 2006). It provides rapid cooling without the temperature limitations associated with cardiac instability or shivering, and for prolonged periods, without the risks of complications associated with whole-body cooling. The aim of this study in a monkey model of TBI was to evaluate the temperature profile of brain tissue cooling for 24 h with the ChillerPad applied to the dura.
Methods
Animals
These studies were approved by the University of Pittsburgh Institutional Animal Care and Use Committee, and were conducted in compliance with the Animal Welfare Act and other relevant federal statutes and regulations. Strict adherence was maintained according to the principles stated in the National Institutes of Health Guide for the Care and Use of Laboratory Animals. The studies were conducted using two female rhesus macaques (Macaca mulatta) weighing 6.9 kg and 5.9 kg, with both testing negative for simian immunodeficiency virus, simian retrovirus, and hepatitis. They were quarantined for 90 days, physically examined, and confirmed tuberculosis-negative according to the protocol of the University of Pittsburgh Division of Laboratory Animal Resources.
Surgical preparation and monitoring
On the day of the study, the animals were sedated with intramuscular (IM) ketamine (20 mg/kg) and given IM atropine (1 mg) to reduce oral secretions prior to endotracheal intubation. The trachea was intubated with a cuffed endotracheal tube and the lungs were mechanically ventilated on 70% nitrous oxide/30% oxygen and 1–2% isoflurane. Depth of anesthesia was guided by visual observation of spontaneous movement, and movement in response to toenail bed pinch by hand. Systolic arterial blood pressure was kept below 120 mm Hg throughout by adjusting the depth of anesthesia.
Central venous and arterial catheters were inserted using standard Seldinger technique through a right groin cut-down. A urethral (Foley) catheter and rectal temperature probe were inserted. Core body temperature was controlled with a water heating blanket and an overhead infrared heating lamp. Physiological variables were recorded every 15 min throughout the study.
Controlled cortical impact and temperature probe placement
The animals were placed prone in a stereotaxic frame during the craniotomy and controlled cortical impact (CCI). The optimal point of impact on the frontal cortex anterior to the precentral gyrus was determined from a baseline magnetic resonance imaging scan. A large U-shaped incision was made over the right scalp. The underlying soft tissues were reflected, and the periosteum over the sagittal suture and right hemisphere was removed. Using a high-speed pneumatic drill (Anspach, Palm Beach Gardens, FL) with a 1.2-mm-diameter burr, a craniotomy 25 mm in diameter was made centered 3.5–4.0 cm posterior to the supraorbital ridge, and 1.5 cm lateral to the superior sagittal suture. A 0.5 cm burr hole was made 1 cm posterolateral to the craniotomy for subdural insertion of a pressure transducer (Integra Neuroscience, Plainsboro, NJ).
CCI was performed with a pneumatic impactor device (Dixon et al., 1998) modified for use with large animals. The impactor device was positioned over the animal's head in the stereotaxic frame such that the impactor tip was targeted at the center of the craniotomy. The impactor tip (1.0 cm in diameter, beveled) was zeroed on the brain correcting for the distance between the dura and the cortical surface. The impactor device was set for a penetration depth of 7 mm at a velocity of 3.5 m/sec with a dwell time of 150 msec. The impact was timed to occur at the height of inspiration to make the depth of penetration and severity of injury consistent between animals. Dural tears were sutured with 6-0 polypropylene.
After CCI, two thermocouples were placed at the impact site (one epidural and one subdural). Three temperature probes were also inserted into the brain within the area exposed by the craniotomy (Fig. 1). The temperature probes were 2 mm (diameter) × 2 cm (length), with five thermocouples spaced 5 mm apart. The probes were inserted perpendicularly to the surface of the brain so that the first thermocouple at the top of each probe (P-0) was just within the cortical tissue. Three additional probes were inserted through burr holes, two posterior probes and one contralateral probe. The bone flap was then replaced on the craniotomy opening and the wound was sutured closed. At this point, a 3-h waiting period after CCI was included prior to initiation of brain cooling to simulate the delay in receiving definitive medical care in a human patient.
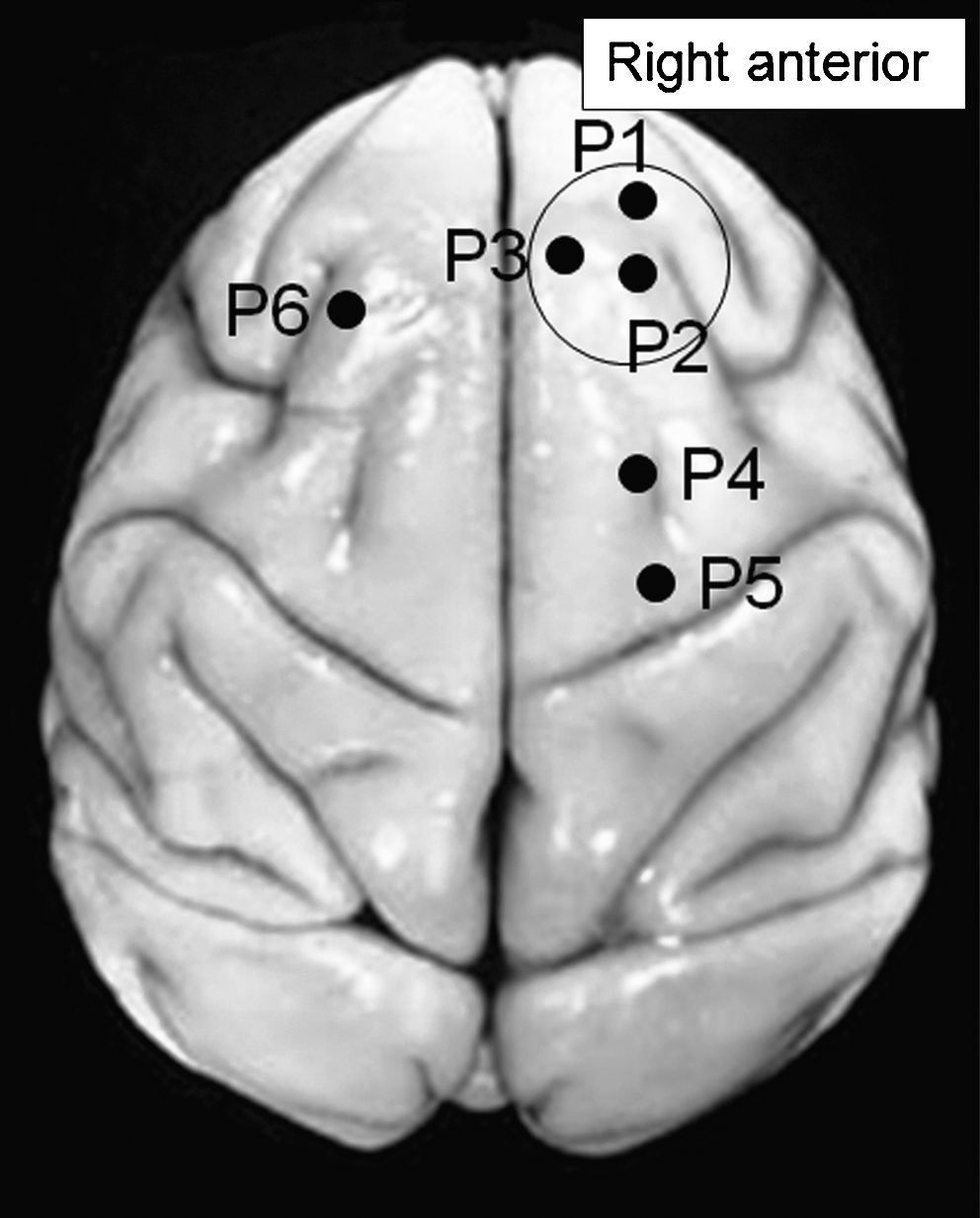
Illustration of the placement of the temperature probes. The circle indicates the craniotomy site (P1, anterior probe; P2, central probe; P3, medial probe; P4, posterior A probe; P5, posterior B probe; P6, contralateral probe).
Placement of the ChillerPad and cooling/rewarming
The ChillerPad device used in this study consisted of: (1) a 20 × 25-mm pad made of cast polyurethane (Fig. 2); (2) foam insulated input and output tubing; (3) a computer-controlled pump (model IP65; Ismatec, Glattbrugg, Switzerland); and (4) a thermoelectric cooler (model LC-200; TE Technologies, Traverse City, MI). At about 2.5 h after CCI, the craniotomy was reopened and the cooling pad was placed on the dura with a thermocouple directly under it. Hypothermia was then initiated 3 h after CCI by activating the pump and thermoelectric cooling device. The cortical surface was cooled to about 15° C and kept at that level for the next 24 h. After 24 h, the ChillerPad device was used to rewarm the brain from 15 to 37°C in a controlled fashion at a rate of 2.5°C/h over about 10 h. Temperature profile data acquisition was performed using a TempScan 1100 with an Exp/10A expansion unit (Omega Technologies Co., Stamford, CT). The data were collected using the ChartView 2.03.3 software application and then downloaded to a Microsoft Excel spreadsheet. Temperature readings for each of the thermocouples were recorded every 2 min for the duration of the study period. At the conclusion of the study, the animals were given a lethal dose of sodium pentobarbital (50 mg/kg) and the brains were perfusion fixed.
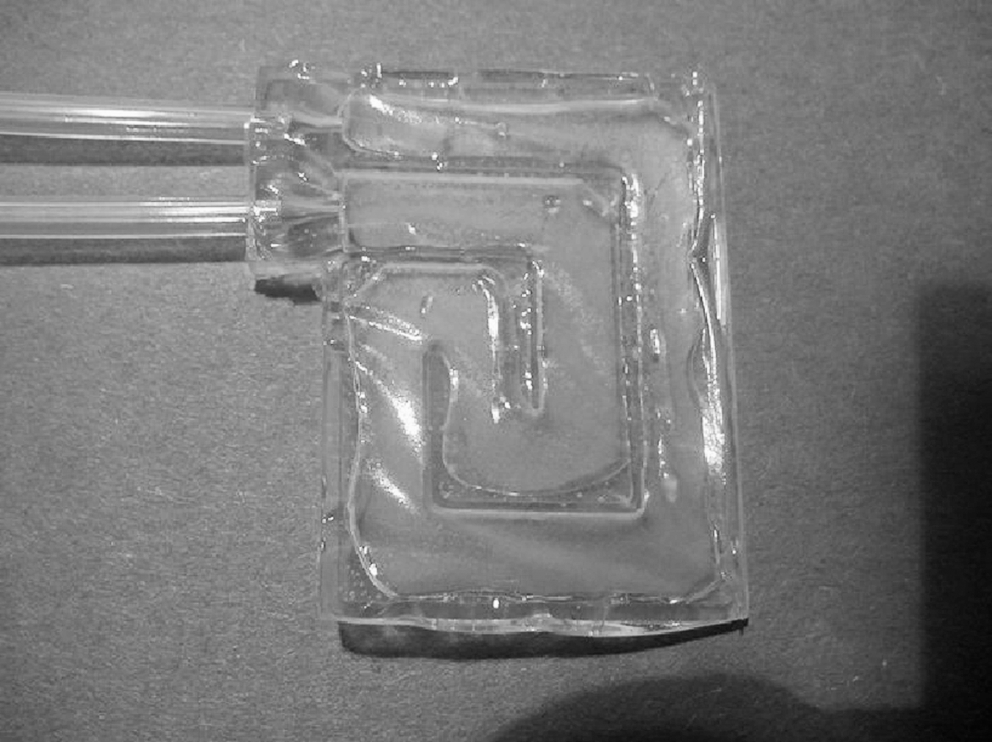
The ChillerPad (dimensions 20 × 25 mm). The pad is placed in contact with the dura and cold saline is circulated through it to provide profound focal cooling.
Results
Physiological variables and core temperatures in both monkeys were well maintained throughout the 24-h cooling and 10-h rewarming periods (Tables 1 and 2). The only notable change was a slight rise in ICP to values of about 8–10 mm Hg, likely due to the TBI. In neither monkey, however, was the ICP increased to a level that would be of clinical concern (i.e., >20 mm Hg), which may be partly due to the induced hypothermia. It would be of clinical interest if epidural cooling to a temperature of 15°C were effective in mitigating the development of intracranial hypertension after TBI.
Controlled cortical impact was performed at 17:16 on day 1. Cooling was initiated at 20:16 on day 1. Rewarming was initiated at 20:16 on day 2.
bpm, beats per minute; BrPM, breaths per minute; ET
Controlled cortical impact was performed at 17:16 on day 1. Cooling was initiated at 20:16 on day 1. Rewarming was initiated at 20:16 on day 2.
bpm, beats per minute; BrPM, breaths per minute; ET
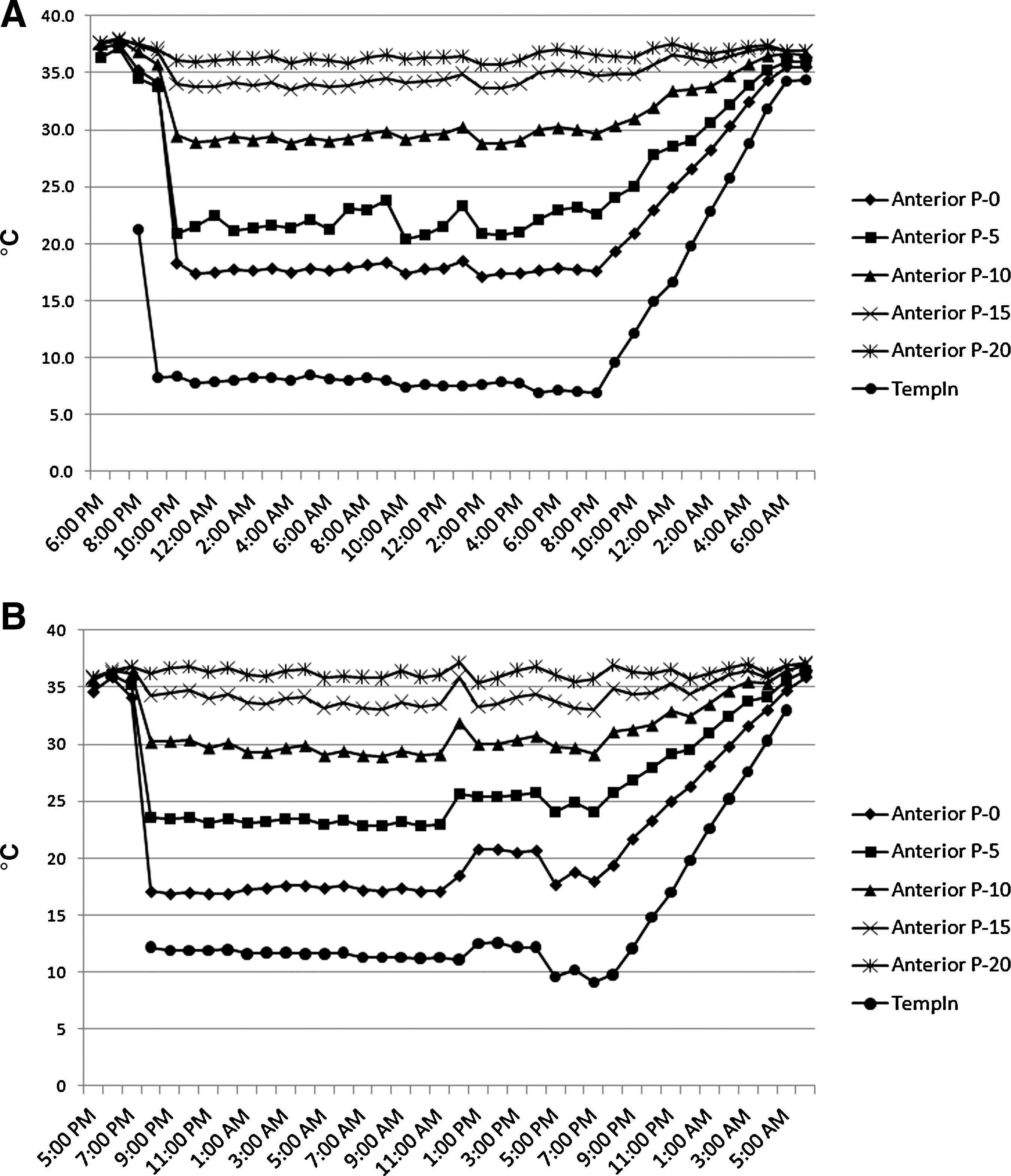
Representative temperature profiles for the P1 (anterior) and P2 (central) probes are shown in Figures 3 and 4. After circulation of cold saline was initiated through the ChillerPad, onset of hypothermia in the cortical tissue was rapid. Cooling to the lowest steady-state temperature occurred in about 10–15 min for the area of the cortex within the craniotomy, and about 30 min at the posterior probes. We elected to perform cooling by initially using circulating saline at >20°C, and then rapidly lowering the temperature. Using colder saline from the start would obviously have resulted in even shorter lag times for tissue cooling.
Temporal profile of brain temperature in monkey #1 (
Temporal profile of brain temperature in monkey #1 (
The P1 (anterior) temperature probe showed that for the first monkey a cortical surface (P-0) temperature of about 17°C resulted in minimum steady-state temperatures of approximately 23, 30, and 33°C at depths of 5, 10, and 15 mm, respectively (Fig. 3A). In the second monkey (Fig. 3B), the temperatures achieved at depths of 5, 10, and 15 mm were about 22, 29, and 34°C, and were approximately the same as those observed in Fig. 3A.
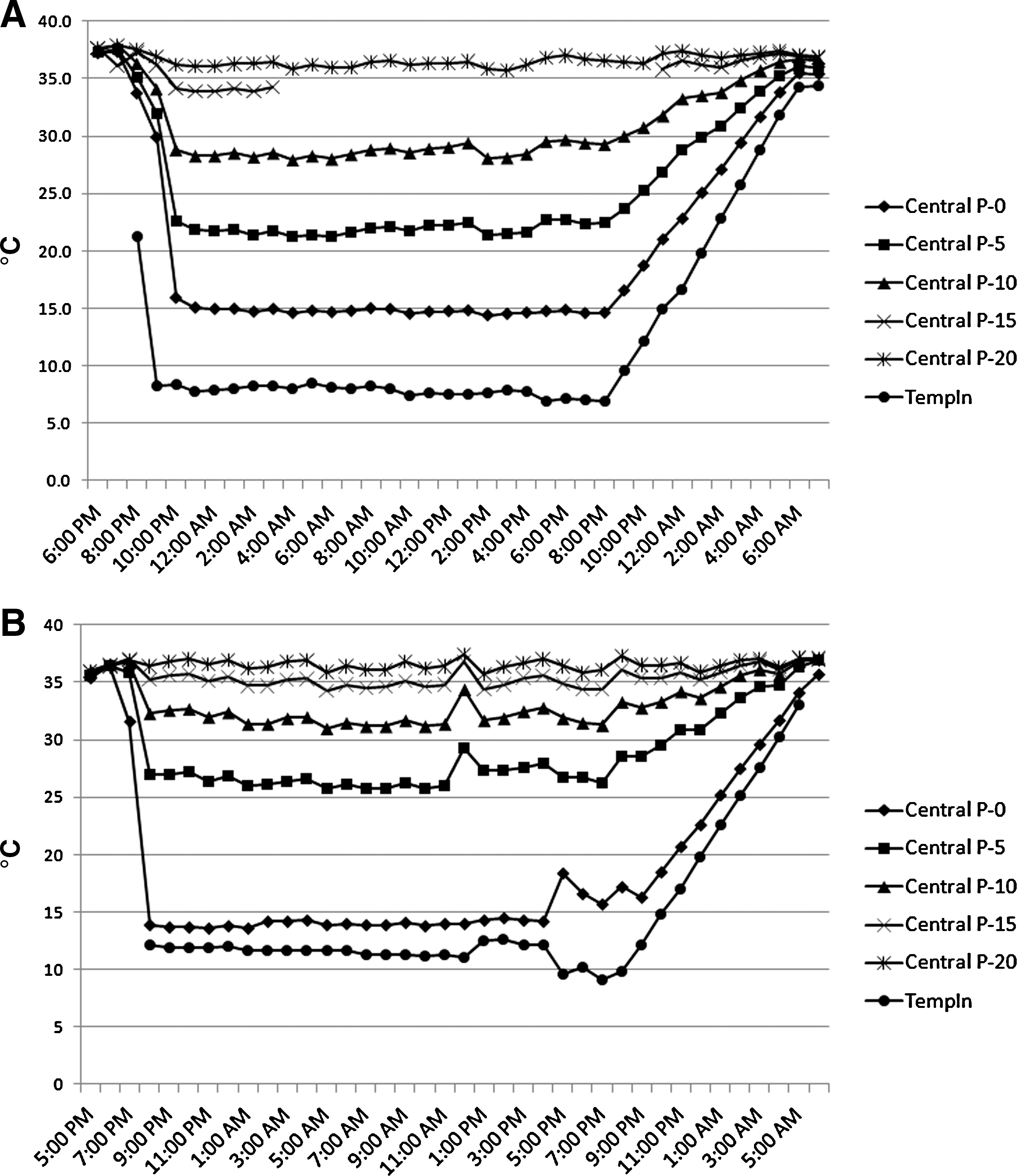
The P2 (central) probe was used as the measurement point for inducing a target temperature at the cortical surface of approximately 15°C. In the first monkey, an inflow temperature (TempIn) of 8°C was required to lower the surface temperature to 15°C, whereas in the second monkey, a surface temperature of about 14°C was achieved with an inflow temperature of about 12°C. Steady-state brain temperatures in the P2 (central) probe for the first monkey were about 22, 28, and 34°C at depths of 5, 10, and 15 mm, respectively (Fig. 4A). The temperatures recorded in the second monkey were slightly higher overall, possibly due to the depth of probe insertion, resulting in corresponding temperatures of about 26, 32, and 35°C, at depths of 5, 10, and 15 mm, respectively (Fig. 4B).
In a comparison of minimum steady-state temperatures at the cortical surface, we found that for the P1 (anterior) and P2 (central) probes, the temperatures were 14–17°C, or up to 10°C lower, than those in the P3 (medial) and P4 (posterior A) probes, indicating that the cooling effect at the surface fell off rapidly with increased distance from the ChillerPad (Table 3). On the other hand, with increasing depth the temperature gradient was less pronounced between probes, resulting in temperatures that were about equal (34–35°C) at a depth of 15 mm. Temperatures recorded at the P5 (posterior B) probe showed relatively minor effects (a minimum cortical surface temperature of approximately 30°C), and no cooling was noted in the P6 (contralateral) probe.
TProbe, five thermocouples per probe spaced 5 mm apart at four depths within the brain in two monkeys (M1 and M2). See Figure 1 for probe locations.
P-0, thermocouple just beneath brain surface; P-5, probe 5 mm deep; P-10, probe 10 mm deep; P-15, probe 15 mm deep.
Discussion
At a dural temperature of approximately 15°C, the ChillerPad cooled the monkey brain to between 34 and 35°C at a depth of 15 mm, the level of the cortical gray/white matter interface. At depths of 5 and 10 mm, brain tissue temperatures of 22–26°C and 28–32°C, respectively, were achieved. These temperatures were sustained for 24 h after CCI, without affecting systemic physiological parameters, and with core temperatures that were readily maintained in the normal range. ICP rose slightly, but this was probably due to the TBI, and it did not reach clinically concerning levels. Induction of profound brain hypothermia by the ChillerPad was highly localized, however, as the extent of tissue cooling rapidly diminished with increasing distance from the device.
To our knowledge, this is the first study to report brain temperature profiles using epidural cooling in a non-human primate TBI model. Cheng and associates described a novel method of epidural cooling in a swine model without TBI using circulating cold saline infused directly into the epidural space (Cheng et al., 2006). They reported brain temperature profiles that demonstrated that hypothermia could be rapidly induced and easily controlled over a 6-h period, after which the brain was allowed to passively rewarm over about 20 min. In a subsequent swine study, this method of epidural cooling was shown to reduce infarction size after middle cerebral artery occlusion (Zhang et al., 2007).
While a swine model has several advantages for this type of study over rodents, the larger cortex relative to the total brain size of a non-human primate more closely models the human brain (Hofman, 1988). For both of the swine epidural cooling studies, commentators for the articles recommended performing similar studies using a non-human primate model. Additionally, only a limited number of temperature probes were used in the prior swine brain temperature profile study: one deep brain probe (1.5 cm deep), one subdural probe, and one epidural probe. In our study we used six penetrating probes with thermocouples at five depth levels, as well as subdural and epidural probes, to obtain a more detailed picture of the effects of epidural cooling on the brain. We also induced hypothermia for 24 h, followed by controlled rewarming over about 10 h, which more closely replicates a therapeutic regimen that might be used in human patients.
The main limitation of this study is the fact that the data were obtained from only two animals. Our goal was to provide clinically applicable estimates of the changes in brain tissue temperatures seen over time resulting from epidural cooling in a TBI model that closely matched humans. Greater precision of these estimates would obviously require additional animals. However, for studies involving non-human primates, issues of appropriate animal resource utilization must be carefully considered. Since the temporal profiles obtained in both animals were similar, we did not believe that a higher degree of precision of the temperature estimates warranted sacrificing additional animals, given the primary purpose of the study.
Our results also do not answer the question of whether profound focal brain cooling for prolonged periods is safe or efficacious. Although the core temperature and other systemic physiological parameters were unaffected, it is possible that cooling an area of the brain to very low temperatures for 24 h or longer may cause tissue damage. Temperatures of 15–18°C appear to be well tolerated by the brain for relatively short intervals (2–3 h) in patients undergoing operative deep hypothermic circulatory arrest (Mascio et al., 2009; Percy et al., 2009). Furthermore, in a porcine model of intracerebral hemorrhage, Wagner and colleagues used the ChillerPad to induce focal cooling at a brain surface temperature of 14°C, followed by brief passive rewarming (30 min), and found a reduction in vasogenic edema and decreased interleukin-1β gene expression (Wagner et al., 2006). However, the duration of cooling in this study was only 12 h. Focal cooling has been performed for as long as 48 h in a rodent stroke model, with improved behavioral and histological outcomes, but only mild hypothermia (33°C) was induced (Clark et al., 2009). Further research will be needed to establish the safety and efficacy of profound focal brain cooling when used for periods of 24 h or longer.
The advantages of a device like the ChillerPad are that deep brain cooling can be localized to the traumatized area and applied for extended periods without affecting body temperature. Rewarming is also easily accomplished by gradual elevation of the ChillerPad temperature. The primary disadvantage of the ChillerPad is the need for a craniotomy. However, a craniotomy is often required as part of routine neurosurgical intervention for subarachnoid hemorrhage and after stroke or TBI requiring decompression, lobectomy, or débridement. Whether local cooling with the ChillerPad will improve recovery in these situations remains to be determined. It is unlikely that the ChillerPad would be effective for deep brain cooling if applied externally (i.e., without a craniotomy), even if used at lower temperatures, because of the insulating effects of the skull, although induction of mild to moderate local hypothermia may be feasible. As discussed below, methods of selective brain hypothermia that involve surface cooling appear to be most effective when blood flowing to the brain is cooled.
The limited extent of brain cooling possible with the ChillerPad is a drawback in the application of such a device for the clinical management of TBI patients. Unlike the situation with stroke, in which brain injury is often more focal, severe trauma frequently causes diffuse injury that affects large areas of both sides of the brain. In such cases, the size of the craniotomy required to use a device like the ChillerPad (or the need for multiple craniotomies) may be impractical. Furthermore, injury to deeper structures of the brain would make any method of epidural cooling ineffective if used as the only means of inducing hypothermia.
Some studies have suggested that hypothermia is most likely to be effective in limiting brain injury if started early after the primary insult. One potential reason that clinical trials have failed to show convincing evidence that hypothermia is effective in treating TBI is that cooling has typically been initiated 4–6 h after the traumatic event, and target temperatures are often not reached until 8 h or longer post-trauma (Clifton et al., 2001; Jiang et al., 2000). Such delays may result in application of hypothermia beyond the therapeutic window (Clifton et al., 2009; Markgraf et al., 2001). Animal studies showing hypothermia to be highly effective in treating TBI have typically had much shorter intervals before beginning therapy. To minimize delays in treatment, it is possible that the optimal approach may prove to be initiating hypothermia on a presumptive basis in the field for patients with serious head injuries (e.g., using intravenous infusion of cold saline), until local brain cooling can be achieved with the ChillerPad or some other selective brain cooling technique.
Several approaches to selective brain cooling have been studied in the setting of TBI (Christian et al., 2008). Surface cooling of the head and neck has been performed using cooling helmets or caps with neck bands, which continuously circulate cold fluid (Liu et al., 2006; Qiu et al., 2006b; Wang et al., 2004). These methods rely on heat transfer through the surface tissues of the scalp and skull, as well as cooling blood in the neck before it flows to the brain. Preliminary results from clinical trials have suggested that this type of selective brain cooling may improve outcomes in patients with TBI (Liu et al., 2006; Qiu et al., 2006b). However, it is unclear how effectively these methods induce brain hypothermia, as they have the same drawback of producing a cooling gradient that limits the utility of epidural cooling (i.e., structures anatomically distant from the cooling source are less affected), and they are a relatively inefficient means of cooling blood flowing to the brain. Nevertheless, the favorable results from initial clinical trials indicate that the extent of cooling may be adequate to provide neuroprotective effects after TBI.
Intranasal cooling has been performed using balloon catheters filled with cold circulating saline (Covaciu et al., 2008), and an inert evaporative coolant sprayed into the intranasal cavity (Wolfson et al., 2008). This approach is very similar in concept to surface cooling with a cooling helmet, and may therefore suffer from the same limitations. Endovascular cooling techniques that have been described include infusing cold autologous blood (Parkins et al., 1954; Schwartz et al., 1996), or cold lactated Ringer's solution (Jiang et al., 2006b), through the carotid artery; infusing cold lactated Ringer's solution through the vertebral artery while clamping the carotid arteries (Ohta et al., 1992); and infusing cold saline through the external jugular veins to achieve a retrograde flush (Wen et al., 2005). While such techniques are efficient methods of cooling the entire brain, they are limited by the difficulty and possible complications of cannulating the carotid or vertebral arteries, as well as the effects of hemodilution or increased cerebral blood flow. Another method of cooling the blood flowing to the brain that does not require arterial cannulation is extraluminal vascular cooling, which involves implanting cooling cuffs around both common carotid arteries (Wei et al., 2008). Although the need to cannulate the carotid or vertebral arteries is avoided with this technique, the task of surgically exposing the carotid arteries prior to placement of the cooling cuffs is technically complex, and would be associated with serious potential complications. Selective brain cooling methods may therefore hold promise, but further research is needed to demonstrate their safety, efficacy, and feasibility, before they can become viable clinical treatment options.
In summary, we have shown that epidural cooling can be used to induce profound focal brain hypothermia in a monkey CCI model. Cooling was easily maintained for 24 h, followed by a 10-h period of controlled rewarming, without changes in core temperature or systemic physiological parameters. It should be noted that since the company that developed the ChillerPad is no longer in business, this device is not available commercially. However, the technology underlying epidural cooling is straightforward and it can be accomplished using similar methods. Furthermore, given the large number of medical device manufacturers in the U.S., it is likely that another company will offer the ChillerPad or a system like it, should this form of treatment prove to be a valuable part of the clinical management of TBI.
Footnotes
Acknowledgments
The authors wish to thank Dr. Geoffrey Manley (Department of Neurosurgery, University of California–San Francisco) for his helpful advice on the setting and timing for the use of the controlled cortical impact device in the monkey. This study was funded by a grant from Seacoast Technologies, Portsmouth, New Hampshire.
Author Disclosure Statement
At the time of this study, Dr. Larnard was the president of Seacoast Technologies, and Mr. Robinson was the technical director for Seacoast Technologies. The company is no longer in business. Dr. Larnard currently holds the patent for the ChillerPad. No other competing financial interests exist.