
Abstract
The complications of spinal cord injury (SCI) increase in number and severity with the level of injury. A recent survey of SCI researchers reveals that animal models of high SCI are essential. Despite this consensus, most laboratories continue to work with mid- or low-thoracic SCI. The available data on cervical SCI in animals characterize incomplete injuries; for example, nearly all studies published in 2009 examine discrete, tract-specific lesions that are not clinically-relevant. A primary barrier to developing animal models of severe, higher SCI is the challenge of animal care, a critical determinant of experimental outcome. Currently, many of these practices vary substantially between laboratories, and are passed down anecdotally within institutions. The care of animals with SCI is complex, and becomes much more challenging as the lesion level ascends. In our experience, the care of animals with high-thoracic (T3) SCI is much more demanding than the care of animals with low-thoracic SCI, even though both injuries result in paraplegia. We have developed an animal care regimen for rats with complete high-thoracic SCI. Our practices have been refined over the past 7 years, in collaboration with animal care centre staff and veterinarians. During this time, we have cared for more than 300 rats with T3 complete transection SCI, with experimental end-points of up to 3 months. Here we provide details of our animal care procedures, including acclimatization, housing, diet, antibiotic prophylaxis, surgical procedures, post-operative monitoring, and prevention of complications. In our laboratory, this comprehensive approach consistently produces good outcomes following T3 complete transection SCI: using body weight as an objective indicator of animal health, we have found that our rats typically return to pre-operative weights within 10 days of T3 complete SCI. It is our hope that the information provided here will improve care of experimental animals, and facilitate adoption of models that directly address the complications associated with higher level injuries.
Introduction
T
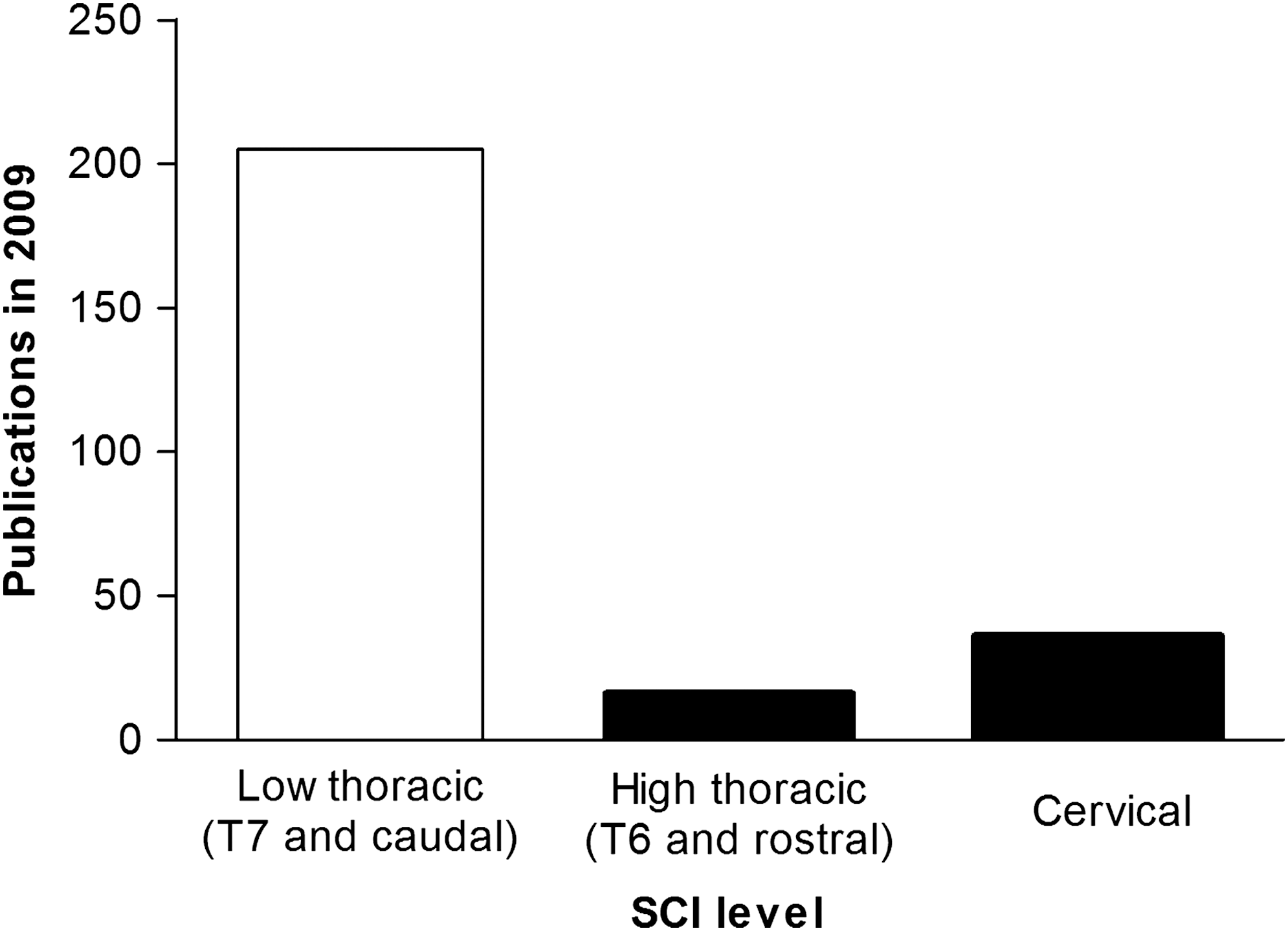
The majority of experimental spinal cord injury (SCI) research employs animal models of low SCI. A systematic search was conducted using PubMed to identify original research articles on experimental SCI. The search term was “spinal cord injury,” and was limited to animal studies published in English during 2009. The articles returned by the search were reviewed to identify the injury level. Based on the most rostral level of SCI, the publications were designated as studies of cervical, high-thoracic (T1–T6), or low-thoracic (T7 and caudal) SCI. For studies of cervical and high-thoracic SCI, the articles were reviewed to identify the mode of injury, maximum survival period, and outcome measures investigated (Table 1). Studies of SCI in embryonic animals, as well as those using in vitro or ex vivo preparations, were excluded. Studies employing models of SCI induced at T7 or below dramatically outnumber studies of SCI at more rostral levels.
Despite the prevalence and devastating effects of clinical high SCI, these injuries are not routinely studied in animal models. A review of original research on experimental SCI published in 2009 reveals that most studies involving cervical SCI employed discrete, tract-specific lesions (unshaded). Only a few use a clinically-relevant injury model, such as a compression or a contusion, that is moderate (medium gray shading) or severe (dark gray shading) in nature. Note that complete transection injuries are also indicated in dark grey. The injury severity “shading” scale is based on the probability of spontaneous functional recovery. In rodents, injuries described as “moderate” (e.g., contusions) often result in substantial amounts of functional recovery over time. Therefore none of the studies published in 2009 examined functionally complete cervical SCI (in keeping with the clinical definition) beyond the acute stages (i.e., 48 h post-SCI).
uni., unilateral; bi., bilateral; EMG, electromyography; MRI, magnetic resonance imaging; fMRI, functional magnetic resonance imaging; TNF, tumor necrosis factor.
The widespread reluctance to perform experiments on animals with higher-level SCI may be in large part due to the challenges associated with animal care. The details of animal care are often handed down anecdotally within institutions or between collaborators, and it is often these details that determine the success or failure of experiments. We have an ethical obligation to provide the best possible care to experimental animals, but the scientific impetus is equally persuasive; for example, such apparently trivial interventions as enriched housing may affect the functional outcome of experimental SCI (Berrocal et al., 2007; Eaton et al., 2008; Lankhorst et al., 2001). Outside the field of SCI, data documenting the impact of animal care on experimental outcome are plentiful and dramatic. Faced with the daunting task of keeping pace with the literature in their own field, many trainees or new investigators working in SCI research may not fully appreciate how these findings on animal care relate to their own work.
Here we report our experience with rats with high-thoracic complete transection SCI. Severe high-thoracic SCI has been used extensively in our laboratory and by others to examine SCI-induced cardiovascular dysfunction (Cameron et al., 2006; Krassioukov and Weaver, 1995; Krenz et al., 1999; Laird et al., 2006; Mayorov et al., 2001). It provides an excellent intermediate step between low-thoracic SCI (which does not typically induce AD, orthostatic hypotension [OH], or other types of cardiovascular dysfunction), and severe cervical SCI (in which these conditions undoubtedly exist, but have not yet been well characterized in animals). We hope our experience can provide some foundation for researchers in other laboratories who might want to test their interventions in a higher, more severe model of SCI. These findings could be particularly useful for groups who wish to incorporate autonomic assessment into their standard battery of outcome measures following experimental SCI.
Methods
Since establishing our laboratory in Vancouver in 2003, we have worked with the University of British Columbia (UBC) Animal Care Centre (ACC) staff and veterinarians to develop a comprehensive approach to animal care. Our practices have evolved over the past 7 years, as we cared for more than 300 experimental animals. Here we present a detailed description of all aspects of animal care in our laboratory, including acclimatization, antibiotic prophylaxis, surgical procedures, caging and bedding, diet, post-operative care and monitoring, and prevention and management of complications. We also provide the rationale behind our practices, and where applicable, cite pertinent data from the animal care/welfare literature.
Our laboratory is primarily interested in autonomic function and dysfunction following SCI. We work with male Wistar rats, weighing approximately 300 g at the time of injury, supplied by Charles River Laboratories (Montreal, Quebec, Canada), or bred at our local animal care facility at the UBC. Experimental animals receive a complete spinal cord transection at the third thoracic level (T3), or sham injury (including durotomy) at the same level (see the section on surgical procedures, below). All of the procedures described have been approved by the UBC ACC.
Results
Acclimatization
Animals need to become accustomed to a laboratory diet and their surroundings prior to any experimentation, in order to minimize stress and ensure reliable data (Conour et al., 2006; Obernier and Baldwin, 2006). Upon arrival at our facility, the animals are immediately transferred to a cage and given food and water ad libitum. Rats bred locally at the UBC are housed in our facility for at least 3 days prior to surgery. Rats shipped by air from Charles River (in our case, from Montreal to Vancouver) arrive at least 1 week prior to the beginning of an experiment. In our experience, these periods of acclimatization dramatically improve post-operative recovery.
Routine animal transportation induces a wide range of physiological changes (Conour et al., 2006; Obernier and Baldwin, 2006). Interestingly, such effects appear to be proportional to the time spent in transit rather than the mode of transportation used (Aguila et al., 1988; Landi et al., 1982). Available data on rodents suggest that a 48- to 72-h acclimatization period is required for most physiological values to return to normal following transport (Conour et al., 2006). Given the critical and controversial roles of the immune system following SCI (Chan, 2008; Popovich and Longbrake, 2008), it is important to note that the rodent immune response is suppressed for several days subsequent to transportation (Obernier and Baldwin, 2006).
During the acclimatization period, new arrivals are provided with the enriched diet used to support them post-operatively. We have found that feeding the animals this diet prior to surgery dramatically reduces post-operative weight loss. In fact, we do not perform surgery until the animals are readily accepting the enriched diet.
As a final component of acclimatization, handling is gradually increased from the time of arrival. The investigators involved in the experiment handle the animals multiple times per day. This is critical in experiments with behavioral or physiological outcomes, since animals habituated to a handler exhibit reduced handling stress (Yelvington et al., 1985). If specific maneuvers will be performed post-operatively (for example, loose restraint for blood pressure monitoring), these maneuvers are mimicked during acclimatization. Acclimating our animals both to investigators and testing procedures increases the chances that the animals will react only to the particular experimental stimuli under investigation (Conour et al., 2006).
Housing
Our animals are housed in a secure clean conventional facility. Rats and mice are housed in separate rooms equipped with internal temperature controls (20–22°C), with low (less than 300 lux) lighting, on a 12-h light-dark cycle (with the light period starting at 7:00
We use kiln-dried and screened wood-chip bedding in the majority of our experiments, although we are currently experimenting with pellet bedding (Purina Yesterday's News; Société des Produits Nestlé S.A., Vevey, Switzerland). Cages for rats with SCI are set up to facilitate movement and keep the abdominal area dry. To this end, a thin (less than one-half inch) layer of bedding is spread on the bottom of the cage, covered by fenestrated matting (Multy Tile; Multy Industries, Atlanta, GA), and then another 1-inch layer of bedding (Fig. 2). We have found that this arrangement dramatically improves mobility and the general condition of rats with SCI. Following surgery, the cages are changed frequently (typically every other day).
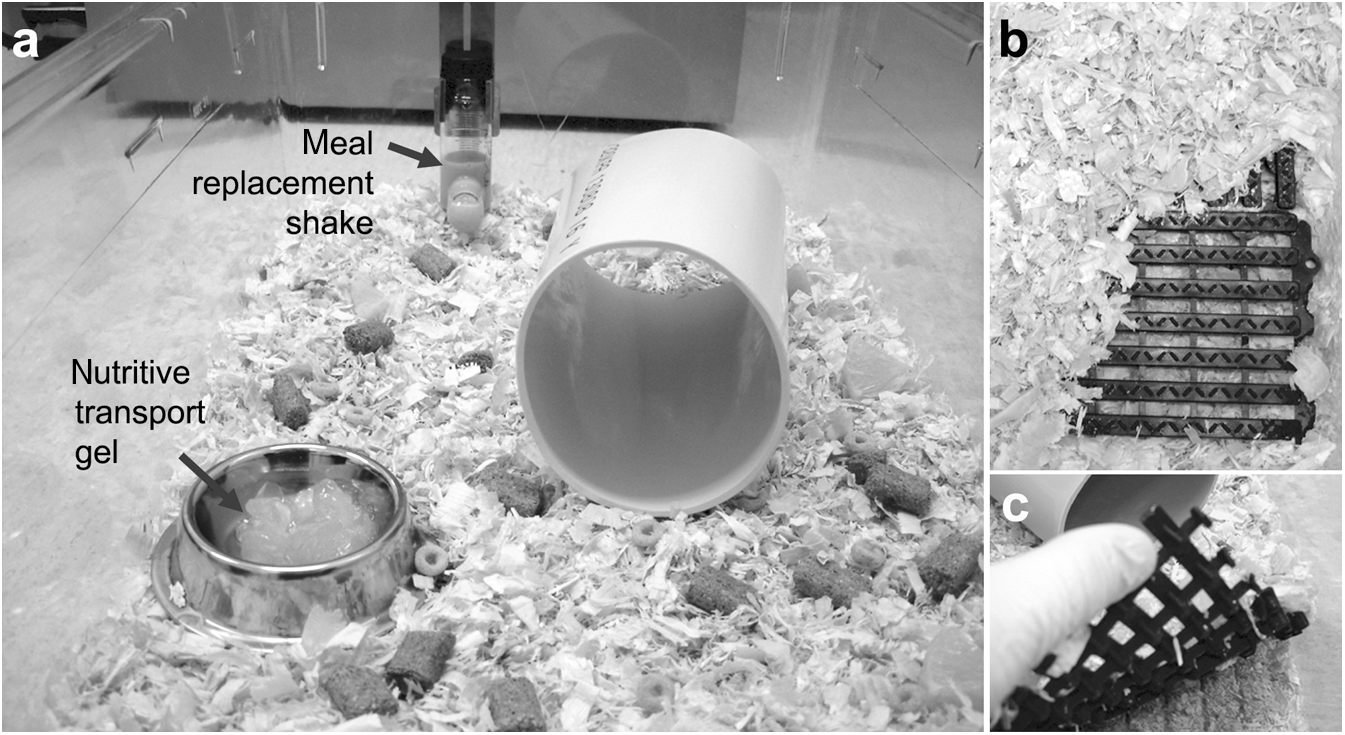
Adapted caging facilitates movement for rats with T3 complete spinal cord injury (SCI). (
As they are social animals, rats are housed in groups of two to four. There is some evidence to suggest that groups of four rats are optimal: Sharp and colleagues (2002) found that rats housed four per cage exhibited a weaker and shorter stress response (elevated heart rate and blood pressure) to common husbandry and experimental procedures than rats housed singly or in pairs. For this reason, we always create stable housing groups of four rats per cage prior to SCI.
We do not individually house animals except when absolutely necessary (for example, to prevent cage mates from disturbing an exposed arterial cannula). In such situations the duration of isolation is minimized (i.e., kept to 24 h or less). The effects of social isolation, particularly long-term isolation, are numerous (Baer, 1971; Baumans, 2005). Individually housing rats can result in altered biochemical parameters, altered food consumption, reduced weight gain, exaggerated stress responses to husbandry procedures, leukopenia, eosinopenia, and changes in weight of the spleen, liver, and adrenal glands (Baer, 1971; Conour et al., 2006; Galef and Wright, 1995; Perez et al., 1997; Sharp et al., 2002, 2003). Long-term isolation (e.g., beyond 80 weeks) has been shown to reduce lifespan (Shaw and Gallagher, 1984). The effects of social isolation on rats are so dramatic that it has been suggested that individually-housed animals do not represent as robust a research model as group-housed animals (Baer, 1971; Conour et al., 2006).
Diet
Our animals receive a varied diet designed to promote good health, provide an additional source of enrichment, and mitigate post-operative complications (see the section on acute post-operative care, below). In addition to standard laboratory rat chow and water, the animals receive meal replacement shakes, nutritive transport gel, fruit, cereal, and a variety of commercially-available rat treats (Table 2). Solid food is scattered throughout the cage, and dispensers for meal replacement shake and nutritive transport gel are located on opposite sides of the cage (Fig. 2). This arrangement encourages movement and foraging behavior. The diet is initiated at least 3 days prior to surgery; beyond post-surgical day 14, meal replacement shakes and nutritive transport gel are no longer provided. By this time, rats are generally gaining 5–10 g of weight per day, and the early support of the shake and gel are no longer required. Food is weighed and provided in the same amounts (per rat) for sham- and spinal cord–injured animals (Table 2). In the days immediately following surgery, sham animals generally consume more than animals with SCI. This difference, however, becomes negligible by post-operative day 7, when caloric consumption per rat is equivalent for sham-injured rats and SCI rats (data not shown). While our diet is appropriate for studies in our laboratory, supplemental feeding should always be considered in light of the experimental question, to avoid potential confounds. For example, some data suggest that vitamin therapy can alter the inflammatory response following experimental SCI (Cristante et al., 2009).
Antibiotic prophylaxis
Prior to surgery, enrofloxacin (Baytril®; Associated Veterinary Purchasing, Langley, British Columbia, Canada) is administered (10 mg/kg SC) once daily for 3 days. Enrofloxacin is a broad-spectrum antibiotic, and we have found that antibiotic prophylaxis dramatically reduces the incidence of bladder infections post-SCI. All of the medications that we use are listed and described in Table 3.
NMDA, N-methyl-D-aspartate.
Surgical procedures
On the day of surgery, the animals are anesthetized with isoflurane (in oxygen, 5% in chamber for induction, 1–3% via nose cone for maintenance) or ketamine/medetomidine (70 mg/kg and 0.5 mg/kg, respectively, IP). The eyes are protected with ocular ointment (Refresh Lacri-Lube; Allergan, Irvine, CA). Then the animals are weighed and the surgical site is carefully shaved and disinfected with alternating swabs of chlorhexadine (Hibitane; Associated Veterinary Purchasing) and 70% ethanol (three times each), followed by povidone-iodine (Betadine®; Associated Veterinary Purchasing) applied for at least 1 min, and removed with alcohol. Buprenorphine (0.02 mg/kg SC) and ketoprofen (5 mg/kg SC) are administered to provide multimodal prophylactic analgesia; enrofloxacin is also administered. Importantly, the bladder is manually expressed in anesthetized animals immediately prior to surgery. We have found that if the bladder is full or if the urethra is obstructed at the time of SCI, post-operative bladder complications are much more likely.
All surgical procedures are performed in accordance with the guidelines of the Canadian Council for Animal Care, and approved by the UBC ACC. Surgery is conducted in a dedicated rodent surgical suite using aseptic technique (specifically, surgeons wear a cap, mask, gloves, and surgical scrubs; the animals are draped; the surgical tools are autoclaved before use and washed and sterilized in hot beads between surgeries; and surgical sponges and gauze are autoclaved prior to use). Surgical tools are only used for five consecutive surgeries with intervening hot-bead sterilization. After five surgeries, the tools are autoclaved prior to further use.
For complete spinal cord transection at T3 (or sham injury at the same level), the rat is positioned over a 5-mL syringe just caudal to the shoulder blades (i.e., with the forelimbs in front of the syringe), in order to create spinal curvature and vertebral separation between T2 and T3, and to improve exposure of the surgical field. A dorsal midline incision is made in the skin and the superficial muscles overlying the C8–T2 vertebrae. Muscles over the T2 vertebra are then bluntly dissected to isolate the T2 dorsal process, which is removed with rongeurs. At the T2–T3 intervertebral gap, the dura is opened with microscissors; this marks the end of the surgical procedure for sham injury, and the incision is closed (see below). For SCI, the spinal cord is cut using extra fine scissors (#14084-08; Fine Science Tools, Foster City, CA). Complete transection is confirmed under the dissecting microscope by visualizing clear division of the rostral and caudal stumps of the cord, and sterile gelfoam is placed in this space. The incision is not closed until hemostasis is achieved. The muscle is sutured continuously using absorbable sutures (Monocryl™ 4-0; Ethicon, San Angelo, TX), and the skin is closed with interrupted non-absorbable sutures (Prolene® 4-0; Ethicon).
Acute post-operative care
Following surgery, the animals receive warmed lactated Ringer's solution (5 mL SC), and are transferred to a temperature-controlled chamber (Animal ICU; HotSpot for Birds, Los Angeles, CA), and closely monitored. In animals with SCI the bladder is manually expressed immediately after surgery. When medetomidine is used as an anesthetic, atipamezole hydrochloride (1 mg/kg SC) is administered as a reversal agent at a minimum of 45 min after induction. Animals recover in the warm chamber until they are alert; at this stage they are returned to a clean cage with their pre-operative cagemates, and supplied with the enriched diet.
For the first 3 post-operative days, the animals receive buprenorphine (0.02 mg/kg SC in the morning and evening), ketoprofen (5 mg/kg SC in the morning), and enrofloxacin (10 mg/kg SC in the morning). For SCI animals, manual bladder expression is performed four times per day. On the seventh post-operative day the skin sutures are removed. All animals are closely monitored during this time, both qualitatively via frequent visits, and formally, using a standardized scoring system (Tables 4 and 5).
The animals are assessed and scored in six categories to generate a composite score. Experimental animals are weighed and monitored daily. In addition to a number of well-defined humane end-points, a composite score of 20 or above necessitates euthanasia. Using our monitoring system, scores for animals with T3 complete transection SCI and sham injury are generally similar by 14 days post-surgery.
IT, immediate treatment required; ISA, immediate surgical attention required; IE, immediate euthanasia.
Monitoring
For the first 14 post-operative days the animals are formally monitored once daily. From this point onward the animals are formally monitored every other day. Each animal is assessed in six categories (body weight, physical appearance, behavior/activity, clinical signs, lesions/autotomy, and tumors/cysts; Tables 4 and 5) to generate a composite score. In addition to a number of well-defined humane end-points, a composite score at or above a pre-determined limit indicates euthanasia. Using our monitoring system, scores for animals with T3 SCI and sham injury are generally similar by 2 weeks post-surgery.
One of our objective monitoring criteria (contributing to the score for physical appearance) is the presence or absence of porphyrin accumulation around the eyes or nose (chromodacryorrhea). Porphyrin is a reddish discharge produced by the harderian gland. Though occasional, small amounts of porphyrin are normal, rats are known to overproduce porphyrin when they are stressed and/or in pain (Harkness and Ridgway, 1980; Harper et al., 2001; Hipolide and Tufik, 1995; Kerins et al., 2003). Porphyrin accumulation is quite common during the first several days after T3 SCI. Significant porphyrin accumulation beyond 1 week post-SCI may be a sign of an underlying problem. In all cases, animals with porphyrin accumulation are monitored closely.
Prevention and treatment of complications
Although vigilant care reduces the frequency and severity of health complications following sham-surgery and SCI, conditions occasionally arise that require treatment. With close monitoring, complications are promptly identified and addressed. We maintain treatment records for each animal, to document the animal's condition and response to intervention.
Post-operative weight loss
Post-operative weight loss is a ubiquitous consequence of experimental SCI. Acute weight loss results largely from decreased food and water intake. During the first post-operative week, rapid and progressive atrophy of hindlimb muscles (Dupont-Versteegden et al., 1998) also begins to contribute to weight loss. Rats with T3 SCI typically lose approximately 10% of their pre-operative weight during the first 5 post-operative days (Krassioukov and Weaver, 1995). While early weight loss is expected, weight loss during the chronic period is a sign of morbidity, and necessitates intervention. In our monitoring system, weight loss exceeding 20% of pre-operative weight is a humane end-point, and is cause for immediate euthanasia.
To minimize weight loss and to help the rats achieve a normal growth curve during recovery from SCI, we provide an enriched diet, to which the rats are acclimated prior to surgery. If an animal is not gaining weight as quickly as expected, or exhibits other signs of morbidity, novel supplemental items (such as scrambled eggs) are provided to encourage eating. In addition, we test for dehydration using a skin pinch, and we treat dehydration with 5 mL of Ringer's solution (given SC) as necessary. An important and often overlooked component of weight loss prevention is adequate peri- and post-operative analgesia, in order to encourage normal food consumption and behavior. We use multi-modal analgesia for the first 3 post-operative days, and thereafter if indicated by inadequate weight gain or other signs of morbidity. In our laboratory, rats often return to their pre-operative weights within 7 days of T3 SCI (Fig. 3). By 2 weeks post-SCI, rats are typically gaining weight at a rate similar to that of sham-operated animals.
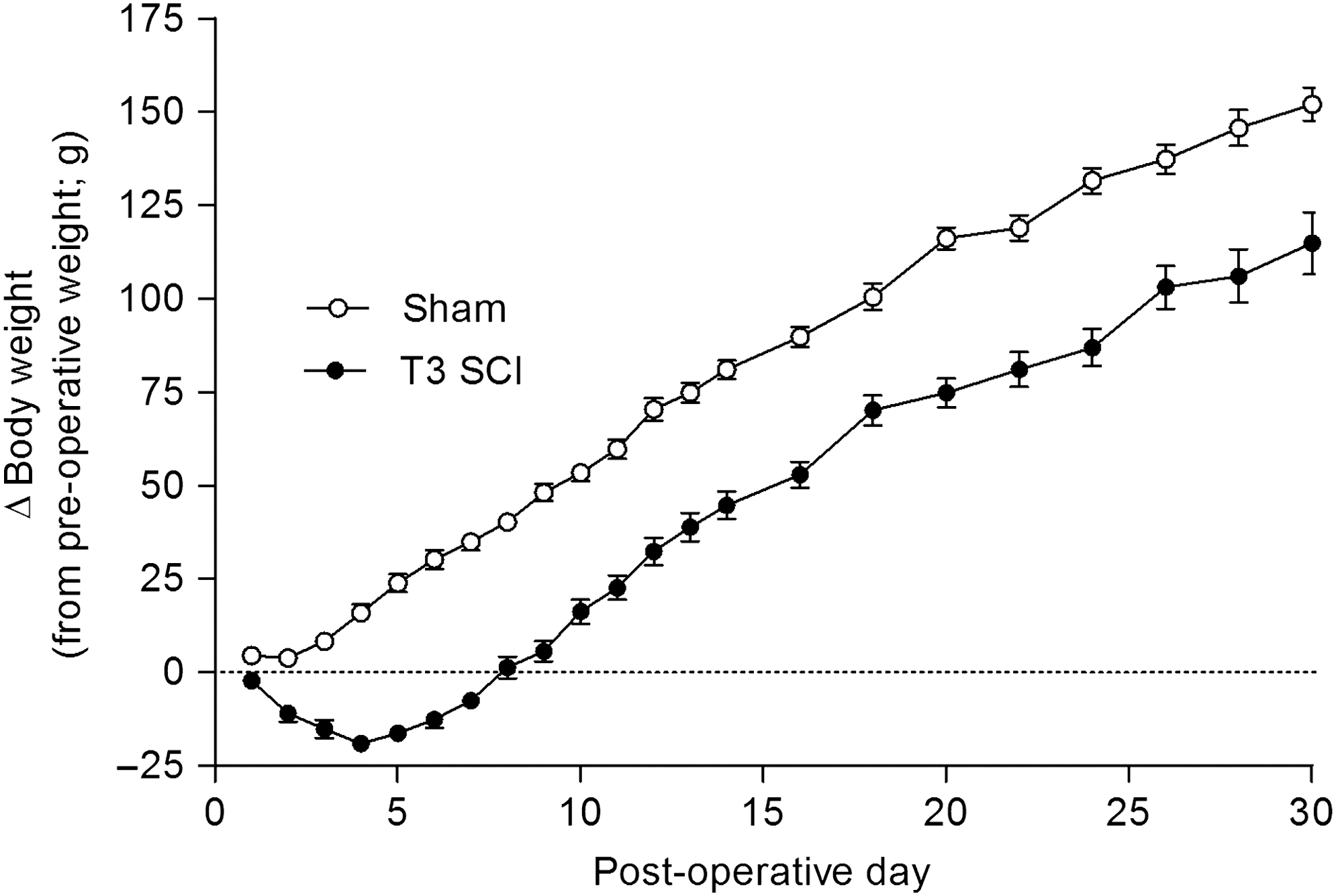
Rats with T3 complete spinal cord injury (SCI) typically return to pre-operative weights within 10 days of injury. Rats with T3 SCI often lose up to 10% of their pre-operative body weight in the first 5 post-operative days. After 5 days, SCI rats begin to gain weight at the same rate as sham-injured animals. From this point on, weight gain in SCI rats parallels that of sham-injured controls. These data are taken from experiments performed over a 1-year period in our laboratory. Error bars represent standard error of the mean (n = 27 for sham-injured animals; n = 50 for animals with T3 SCI).
Bladder management
In caring for rats with SCI, bladder management is an especially important consideration. Prevention of bladder-related complications begins pre-operatively with antibiotic prophylaxis, and we empty the bladder immediately prior to SCI (i.e., after the animal is anesthetized). Following complete T3 transection, the bladder becomes neurogenic. As a result, the bladder should be manually expressed at least three times per day, and we typically perform manual expression four times per day for the first post-operative week. Once reflexive micturition returns, manual expression is reduced to twice per day (but is maintained to check for urethral obstructions or other problems). While reflexive micturition generally resumes by about post-operative day 10, substantial variation exists, and the frequency and timeline for manual expression must be determined according to the needs of the individual animal. In order to minimize the possibility of rupture, bladder expression must be conducted with patience and care. If the bladder does not empty readily in response to manual expression, we have found that light induction with isoflurane facilitates effective emptying.
In some experiments we have used catheterization to manage the neurogenic bladder in animals with SCI (e.g., Krassioukov and Weaver, 1995). Intermittent catheterization can be used in female rats; in male rats, suprapubic catheters can be implanted and tunneled subcutaneously to exit between the scapula. While catheterization is not strictly necessary for bladder management in rats with T3 SCI, it may provide an alternative or adjunct to manual expression for investigators with the appropriate expertise.
Despite routine bladder expression and prophylactic antibiotics, lower urinary tract (LUT) infection is still a relatively common occurrence in rats with SCI. Clinical signs of LUT infection include cloudy, discolored, or foul-smelling urine, increased difficulty in manual expression, and a wet or discolored abdomen (after the onset of reflexive micturition). While hematuria can be a sign of infection, early hematuria is common following experimental SCI, and may be due to distension of the bladder wall with capillary breakage (Santos-Benito et al., 2006). Animals suspected of having an infection are monitored closely and have their bladders manually expressed more frequently than normal. In addition, they receive a 3-day course of enrofloxacin (10 mg/kg SC once daily). These steps usually resolve the underlying infection, and bladder function returns to its pre-infection status.
Although less common than complications related to the LUT, disrupted bowel function is also encountered in rats with SCI. Constipation or compaction can occur following SCI, due to the loss of autonomic control of the gastrointestinal tract. This can be largely prevented by introducing an appropriate diet prior to SCI. The diet we use during the acute recovery period consists largely of liquids and fruit, and generally prevents problems with constipation. Rats with T3 SCI typically begin having bowel movements within 24 h of SCI. On rare occasions when constipation persists or recurs, we have successfully used glycerol enemata (50:50 glycerol to PBS) to soften stool in the rectum.
An occasional side effect of diets aimed at preventing constipation is soft stool. Dietary modifications (shifting toward an increasingly solid diet) usually resolve the condition within a week or less; frequent cage changes and close monitoring (e.g., assessing hydration status) are important in keeping animals healthy during this period. Soft stool unrelated to a liquid- or fruit-rich diet may be a sign of another underlying health condition, although this is not a complication we typically encounter in rats with T3 SCI.
Pressure sores
Rats with T3 SCI can develop pressure sores, typically on the abdomen, hips, and hind legs. Precursors to pressure sores appear as smooth hairless patches, which may become red and inflamed. Without treatment an ulcer can develop. Pressure sores can be largely prevented with appropriate caging. We arrange cages for rats with SCI to facilitate movement and keep the animals dry, and we change cages frequently (see the section on housing, above). Rats with SCI are inspected for early signs of pressure sores during daily monitoring; if hairless patches are observed the amount of bedding is increased, which usually resolves the problem. If redness, inflammation, or skin ulcerations develop, the area is washed (with Hibitane) and treated with topical antibiotic ointment twice daily until healed.
Complications associated with the surgical incision site
Complications associated with the surgical incision site are rare after experimental SCI, but can include infection, edema, and cyst formation. Superficial infections, indicated by persistent inflammation or the presence of pus, are normally treated with a topical antibiotic ointment applied one to three times daily. We treat more persistent infections with a 3-day course of enrofloxacin (10 mg/kg SC once daily). If edema appears and persists under the surgical incision site, the fluid is drained, and Ringer's solution is administered (SC). Cysts, on the other hand, are generally left undisturbed, unless the animal's condition begins to deteriorate or the cyst can easily be excised. With cysts, edema, and other such incision-site abnormalities, surgical intervention is a last resort.
Incision-site scratching occasionally occurs in sham-injured animals. Presumably indicative of discomfort and pruritus associated with sutures and surgical wounds, untreated scratching can cause significant damage to skin surrounding the incision site. Animals that exhibit persistent scratching receive ketoprofen (5 mg/kg SC) once daily until scratching (and associated skin irritation) resolves. To mitigate damage due to scratching, we clip the fore- and hind-paw nails (under isoflurane). Irritated skin is treated with topical and antibiotic ointment, applied one to three times daily. Sutures are removed as early as possible (by 7 days post-surgery), as they can contribute to pruritus and discomfort. We assume that animals with SCI may be experiencing similar sensations at the incision site, even though they are unable to scratch using their hind limbs. Therefore we also provide post-operative analgesia, remove sutures promptly, and apply ointment (if inflammation persists at the surgical incision) following SCI.
Rapid return of pre-operative weight following T3 SCI
We have cared for more than 300 rats with T3 SCI over the past 7 years, with experimental survival times ranging from 1 week to 3 months. During this time we have continually refined our practices, in consultation and collaboration with the UBC ACC staff and veterinarians. In addition, all of our staff (trainees and technicians) complete mandatory courses with classroom and laboratory components covering rodent biology, handling, husbandry, anesthesia, and surgery. As a result, we believe we are able to provide a very high level of animal care. Despite the severity of SCI, we have very low mortality rates (ranging from 0–10%), and experience few unanticipated complications. Using body weight as an objective indicator of experimental animal health, we have found that our rats typically return to pre-operative weights within 10 days of T3 complete SCI (Fig. 3), a dramatic departure from what we have heard anecdotally, and from what has been reported previously in the literature (e.g., Primeaux et al., 2007).
Discussion
Recent clinical data reveal that the incidence of high SCI is increasing (
Although animal care is a critical determinant of experimental success, the description of animal care provided in the Methods section of many manuscripts is often very limited. In many cases, the detail provided would not allow other researchers to successfully maintain animals with SCI: however, there are several notable exceptions. Osborn and colleagues (1990) describe an intensive approach to care of rats with complete cervical (C7-T1) transection. Although the animals were only maintained for one week in this study, this is a very severe injury, and the animal care procedures described are complex and technically demanding. Several days prior to SCI, animals were implanted with indwelling cannulae for intragastric infusion of a liquid diet. To our knowledge, this is a unique approach to the problem of reduced food and water intake following high SCI. Animals were also implanted with indwelling catheters for bladder management. The authors indicate that manual expression of the bladder proved inadequate in this high injury model, and that AD due to bladder distension can be fatal in rats with severe, cervical SCI. While we report that bladder catheterization is not strictly necessary following complete transection at T3, it may be required for management of animals with higher SCI. This is certainly plausible in light of clinical findings, which indicate that severity of AD increases as lesion level ascends (Curt et al., 1997; Helkowski et al., 2003).
Two other published works (Santos-Benito et al., 2006; Puckett et al., 2008) document in detail the care of animals with SCI. Although these are not specific for care of animals with high SCI, they should be consulted by investigators as resources that are complimentary to this manuscript. The book chapter by Puckett and colleagues provides excellent examples of animal monitoring protocols, as well as information on medications and suppliers that may be particularly pertinent to investigators working in the US. Some features of animal care documented in this chapter represent a slight departure from our approach. For example, Puckett et al. do not describe antibiotic prophylaxis as part of their standard of care. Also, they suggest 48 hours as a minimum acclimation time (in keeping with guidelines of the American Association for Laboratory Animal Science). Longer acclimation periods and antibiotic prophylaxis may be requirements for care of animals with higher SCI, although we have not tested this premise experimentally. Puckett et al. also remark that animals are initially resistant to liquid meal supplements (such as Ensure) offered post-operatively. We have found that it is critical to introduce animals to Ensure prior to performing SCI, a method that we adopted from Pearse and colleagues (Pearse et al., 2004). These distinctions highlight the importance of consulting multiple sources in developing an animal care strategy: the best approach will incorporate the combined experience of multiple research groups.
The work of Chance reveals an effect that commonly receives short shrift: the better the care of laboratory animals, the lower the variance in experimental results (Chance, 1957; Chance and Russell, 1997). The issue of variability is particularly germane to SCI research, for which multiple treatments are often combined, targeting different barriers to functional recovery (Bunge, 2008). The Achilles' heel of the combinatorial approach is the large number of experimental groups required. To rigorously investigate a potential combination therapy, the components must first be tested alone and in every combination (Pearse et al., 2004). The practical importance of reducing the number of animals in each group is immediately apparent. Thus, excellent animal care is not merely an ethical, but also a scientific obligation, which maximizes our chances of success; it should be foremost in all of our minds when performing investigations of SCI.
Footnotes
Acknowledgments
These experiments were supported by the Heart and Stroke Foundation of Canada (HSFC; British Columbia and the Yukon). L.M.R. is also supported by the HSFC. We gratefully acknowledge the ongoing support of the Animal Care Centre at the University of British Columbia. We would like to thank Drs. Tamara Godbey and Lowell McPhail for their assistance and support.
Author Disclosure Statement
No competing financial interests exist.