
Abstract
Regional strain-based brain injury intensity during controlled cortical impact (CCI) was studied using a three-dimensional numerical rat brain model. A full factorial design of CCI computer experiments was performed using two typical impactor shapes (flat or hemispherical) at a fixed impact velocity of 4 m/s with various impact depths (1, 1.5, 1.6, 2, 2.5, 2.7, and 3 mm) and various impactor diameters (4, 5, 6, 8, and 9.5 mm). In total, 70 CCI cases were simulated numerically. Two injury assessment measures, the cumulative strain damage measure (CSDM), which accounts for the volume of brain tissue with elevated strains, and cumulative strain damage percentage measure (CSDPM), which is a strain-based estimate of the neuronal cell loss percentage, were used to evaluate the risk of brain injury. Results demonstrated positive nonlinear relationships between impact depth and these injury assessment measures in six regions of interest: ipsilateral cortex, ipsilateral corpus callosum, ipsilateral hippocampus, ipsilateral thalamus, cerebellum, and brainstem. However, the impactor diameter was not always positively correlated with regional tissue strains. For the flat impactor group, the 5 mm diameter impactor induced more tissue strain in the corpus callosum/hippocampus, and a smaller impactor induced more strain in the thalamus. For the hemispherical impactor group, a larger impactor tended to induce more tissue strain in subcortical regions, with the exception of the 6 mm diameter impactor. This study systematically predicts regional intensity of primary brain injury according to tissue strain distributions in the hope that strain distribution maps may become a common platform to compare CCI severities with different configurations.
Introduction
P
Human TBI experiments can only be conducted at non-injurious levels for obvious ethical reasons. To make up for this shortcoming, many in vivo TBI animal models have been developed to provide insight into injury mechanisms at the cellular/molecular level and are also used for studying the efficacy of candidate therapeutic interventions. In general, the symptoms, histological images, and behavioral evaluations monitored in animals are used to define brain injury severity (e.g. mild, moderate, or severe) in a global sense. Because one advantage of laboratory TBI tests is that the externally applied mechanical factors can be precisely controlled and measured (explained more fully in the subsequent paragraph), these external impact parameters are also frequently used as general indictors for reporting TBI severity. However, these global classification methods are inadequate because an animal subjected to a specific impact scenario may sustain different injury severities at each distinct region of the brain. Additionally, many challenges exist to equate animal and human TBI, one of them being how to define “comparable” injury severity in different species at different regions given the obvious geometrical differences between humans and laboratory animals (predominantly rodents).
The controlled cortical impact (CCI) model has been extensively used to induce focal brain injuries via indentation of a rigid impactor at a pre-set speed onto the exposed dura mater of a rat (Dixon et al., 1991; Lighthall, 1988), despite the fact that others have reported that this experimental model may also generate diffuse injuries (Hall et al., 2008). The injury severity (mild, moderate, or severe) is usually defined in reference to external impact parameters, such as the impact depth and velocity, without consideration of varying regional responses. Because different laboratories define their own injury severity based on different combinations of these parameters, conflicting definitions are commonly observed in the literature. For example, in different publications, an impact depth of 3 mm was considered “moderate” (e.g., Aoyama et al., 2002; Dunn-Meynell and Levin, 1997; Ji et al., 2005; Kawamata et al., 1997; Portella et al., 2000; Strauss et al., 2004) whereas an impact depth of 2 mm (or less) was deemed “severe” (e.g., Ahn et al., 2008; Baldwin et al., 1996; Davis et al., 2008; Gabbita et al., 2005; Larner et al., 2005; Rothoerl et al., 2000; Sutton et al., 1993; Woertgen et al., 2001, 2002). Similar conflicting conclusions can be identified for impact velocities as well. This confusion may be the result of other external parameters, such as the impactor shape or varying precision of different CCI devices used in different laboratories. In any event, deciphering the combined effects of the various parameters in different experimental setups would be very difficult, if not impossible. Partially for this reason, comparison of regional injury severities created by different CCI setups used by various laboratories was rarely attempted.
These findings suggested that impact parameter-based injury severity has only limited value and intracranial biomechanical measures are needed to classify region-specific injury intensity. During an injury, externally applied loading is transferred to intracranial tissues, which in turn react with increased stress/strain. Both in vitro and in vivo experiments have shown that there are direct correlations between brain tissue stress/strain and injury outcome (e.g., Bain and Meaney 1999, 2000; Cater et al., 2006; Elkin and Morrison, 2007; Elkin et al., 2007; LaPlaca et al., 2007; Morrison et al., 2003; Shreiber et al., 1997). Therefore, it can be hypothesized that regional tissue-level strain response is directly linked to the primary brain injury observed in the same region. A systematic biomechanical investigation of regional tissue strains could provide a common ground for describing the heterogeneous nature of injury distributions inside a brain.
At present, the best method to predict intracranial biomechanical strains is through finite element (FE) modeling. Several FE models of the rat brain have been developed to simulate various CCI scenarios (Levchakov et al., 2006; Mao et al., 2006; Pena et al., 2005). By comparing regional tissue strains predicted from FE models to various cellular or axonal injuries observed in the corresponding location in experimental tests, the vulnerability of different cells/axons could be investigated. Such a strain-based vulnerability “map” could provide useful information for choosing appropriate animal models for the study of therapeutic strategies to treat region-specific TBI.
The objective of the current study was to systematically calculate intracranial biomechanical responses at six regions of interest (ROI's), including the ipsilateral cortex, ipsilateral corpus callosum, ipsilateral hippocampus, ipsilateral thalamus, cerebellum, and brainstem. This was accomplished using a previously developed FE model of the rat brain, which was subjected to a large spectrum of commonly used CCI scenarios. Also, both flat and hemispherical impactors were simulated to depict differences caused by geometric variation at the impactor–brain interface. Lastly, statistically based response surfaces were generated to deduce the relationships between different combinations of external impact parameters (CCI impact depth and impactor diameter) and regional injury intensity based on FE model-predicted strain values.
Methods
Brief descriptions of the FE rat brain model
The FE rat brain model previously developed by Mao et al. (2006) was used in the current study (Fig. 1). The model geometry was taken from histological studies of rat brain by Paxinos and Watson (2005) and included explicit representations of all essential anatomical features of a rat brain, such as the olfactory bulb, cortex, hippocampus, thalamus, hypothalamus, corpus callosum, brainstem (midbrain, pons, and medulla oblongata), cerebellum, lateral ventricle, third ventricle, fourth ventricle, internal capsule, external capsule, and part of the spinal cord. Typical spatial resolution of the FE model was 200 μm to ensure numerical convergence under impact loading conditions. All brain materials were simulated using a linear viscoelastic material (LS-DYNA Material Type 61) with a decay constant of 20 ms. For the cerebral gray matter, cerebellum, and brainstem, a short-term shear modulus of 1.72 kPa and a long-term shear modulus of 0.51 kPa were assumed (Gefen et al., 2003). For the white matter, a short-term shear modulus of 1.2 kPa and a long-term shear modulus of 0.36 kPa were assumed. The model was biomechanically validated against experimentally measured cortical deformation reported by Shreiber et al. (1997).

Rat brain finite element model.
CCI parameters selected for full factorial simulations
A review of 235 articles, found through PubMed (United States National Library of Medicine) search of CCI experiments on adult rats, was performed for choosing most appropriate spectrum for FE analysis. For the impact depth, the most often used was 2 mm (77 articles), followed by 2.5 mm (52), 3 mm (29), 1 mm (23), 2.7 mm (14), 1.5 mm (11), and 1.6 mm (10). Fewer than five articles used other impact depths. As to the impactor diameter, a 5-mm diameter impactor was most often used (75), followed by 6 mm (39), 8 mm (12), 9.5 mm (7), and 4 mm (5) whereas fewer than five articles reported use of other sizes. Most studies did not report the shape of the impactor used. Among those studies that reported the impactor shape, a flat impactor was most prevalent, whereas limited studies used a hemispherical or rounded impactor. In a series of numerical analysis (Mao et al., 2010b), the impact velocity was not found to have a statistically significant effect on the FE model-predicted strain responses in the range of 4 to 6 m/s, and was hence not studied.
Based the abovementioned review, a full factorial design was adopted to study the effect of each parameter (the impact depth, impactor diameter, and impactor shape) as well as interactions between these parameters on the injury assessment measures (responses). A total of 70 CCI cases were simulated, which included two impactor shapes (flat and hemispherical), seven impact depth levels (1, 1.5, 1.6, 2, 2.5, 2.7, and 3 mm), and five different impactor diameters (4, 5, 6, 8, and 9.5 mm). The center of impact was adjusted between bregma and lamda sutures based on most commonly used experimental setups. For 4, 5, 6, and 8 mm diameter impactors, the impact center was 4.5 mm lateral to center line. For 9.5 mm diameter, the impact center was slightly adjusted as 5.0 mm lateral to center line. The diameters of unilateral craniotomy were 1.0 mm larger than the impactor diameters except for the 9.5-mm diameter impactor, for which a 10.0 mm diameter unilateral craniotomy was used to avoid crossing over the midline. In all cases, the impactors were adjusted to point perpendicularly to the brain surface.
Response variables and injury threshold
Two response variables, cumulative strain damage measure (CSDM) and cumulative strain damage percentage measure (CSDPM), were selected to analyze individual and combined effects of the three parameters. It has been postulated by Bandak and Eppinger (1994) that the extent of brain injury is related to the cumulative volume of brain matter experiencing a strain exceeding the injury threshold. This concept of using a cumulative measure to estimate the risk of brain injury is better than using the maximum value calculated in one element (or a limited number of elements in a region); in part because a single element may happen to have poor mesh quality, which affects computational accuracy. Takhounts et al. further termed this concept CSDM and applied it to predicting the risk of sustaining diffuse axonal injury during automotive crashes by counting the volume of elements, which experienced strain over a pre-selected threshold value (Takhounts et al., 2003, 2008). Mao et al. (2006) adopted the CSDM concept to study rat brain contusion volume during CCI. These authors found that the FE model-predicted cumulative volume, based on a 30% maximum principal strain (MPS) threshold, matched well with experimentally measured brain contusion volumes measured between 7 and 14 days post-injury. In the current study, the total volume of the elements experiencing an MPS of >0.30 during the CCI impact (henceforth refer to as CSDM 0.30) was calculated at six ROI's, namely the ipsilateral cortex, ipsilateral hippocampus, ipsilateral thalamus, ipsilateral corpus callosum, cerebellum, and brainstem, for all 70 cases, to systematically evaluate the effects of these parameters.
Another concept hypothesized is that the element-level peak strain magnitude is related to the intensity of brain injury within that element. In particular, the percentage of cell loss is assumed to be related to the magnitude of element strain. The FE rat brain model used in this study consists of 255,700 hexahedral elements among which a total of 116,738 hexahedral elements representing the six ROI's were examined. Mao et al. (2010a, b) proposed a CSDPM concept and found a significant positive correlation between experimentally measured percentage of neuronal cell loss and FE model-predicted MPS. The difference between CSDPM and CSDM is that CSDM counted the total volume of brain elements exceeding a certain threshold strain value. In CSDPM, neuronal loss percentage was calculated for each brain element (∼200 μm resolution) first before the average percentage of cell loss for a region was determined. Equation 1 shows the proposed CSDPM as:
Where i represents the brain element number and N is the total number of elements in the FE brain model.
Finite element model simulations
All 70 cases of CCI simulation were performed using LS-DYNA 971 (LSTC, Livermore, CA) on a 64-bit Opteron 128 CPU cluster. The impact velocity was assumed constant at 4 m/s, which was the most common impact velocity from the literature review. At this velocity, the peak deformation (3 mm) was reached 0.75 ms after impact initiation. Consequently, only the first 2 ms of CCI was simulated to save computational cost. The typical execution time was 7 h for each simulation using 16 CPU's with the MPS values output at an interval of 0.1 ms for all brain elements. After all the simulations were completed, several in-house programs in C++ (Microsoft, Seattle, WA) were used to calculate the peak MPS each element experienced during CCI. From these data the CSDM and CSDPM were computed for further analysis.
Response surface methodology - radial basis functions
Response Surface Methodology (RSM) is a statistical technique commonly used to represent the relationships between response variables and input parameters. In this study, the response variables are regional CSDM and CSDPM and the input parameters are impact depth and diameter. The goal of using RSM was to graphically and mathematically depict the relationship between changing impact depth and diameter on CSDM and CSDPM. The response surface is constructed from sampling points (defined as the magnitude of response variable at chosen parameter values) obtained experimentally or, in this case, a full factorial design of computer experiments (DOCE). Since the response surfaces represent continuous and complex changes based on a limited number of sampling points, the selection of an appropriate function to construct the RSM and validation procedures are critical to guarantee the reliability of response surfaces.
Data reported in the literature suggest that a simple polynomial response surface model may be insufficient for modeling complex processes (Bates et al., 1996; Koehler and Owen, 1996; Sacks et al., 1989a, b). For example, second-order response surfaces are incapable of modeling response surfaces with multiple extrema, as these surfaces allow only one extremum. Radial basis functions (RBF's) are a commonly used method to approximate a multivariate function with a combined number of linear terms that depend only upon the distance from a reference point. Because each term is based on radial distance only, RBF are a powerful tool for constructing a multi-dimensional response surface. Using this method, each sampling point is ensured to pass through the response surface. For points other than the sampling points, interpolations are performed to form a smooth surface. It has been shown that RBF are highly efficient in practice for easy adjustment of smoothness with high convergence properties (Buhmann, 2003).
Equation 2 shows a typical way of using RBF to approximate a multivariate function:
where the approximating function y(x) is represented as a sum of N RBF's, each associated with a different center ci and an appropriate weighting coefficient wi. Because the approximate function is based on linear combination in the weights, wi can be estimated using the matrix methods of linear least squares. Approximation schemes of this kind have been particularly useful in developing time series predictions (Hong and Billings, 1998; Sheta and Jong, 2001), controlling of nonlinear systems exhibiting sufficiently simple chaotic behavior (Cowper et al., 2002; Kim et al., 2000), 3-D reconstruction in computer graphics (Boyd and Wang, 2009; Lapeer et al., 2010), and among other applications.
As in any reasonably reconstructed response surface model, several data points not used in constructing the response surface are needed to test the accuracy of the response surface created by RBF's. Of the 70 cases simulated, injuries induced by the flat or hemispherical impactor were considered not comparable; hence, simulation results from these two groups were analyzed separately. For the 35 FE simulations within each group, data from 31 FE simulations were extracted based on a data set reducer algorithm (modeFrontier 4.2.0, Esteco, Trieste, Italy) to construct the corresponding CSDM and CSDPM response surfaces based on RBF's using minimized standardized mean squared error. According to Yang et al. (2005), between 10% and 20% of sampling cases were typically used for validation. In this study, the remaining four data points (12.9%) were used to validate the accuracy of the RBF-based response surfaces. For each type of impactor (flat or hemispherical), two injury measures (CSDM and CSDPM) were obtained at six different regions (ipsilateral cortex, ipsilateral corpus callosum, ipsilateral hippocampus, ipsilateral thalamus, cerebellum, and brainstem) from FE simulations. Hence, a total of 24 (2 × 2 × 6) response surfaces were constructed.
In modeFrontier version 4.2.0, commonly used RBF's include Gaussians, Duchon's polyharmonic splines, Hardy's multi-quadrics, inverse multi-quadrics, and Wendiand's compactly supported functions. In order to construct the most accurate response surfaces, all the abovementioned RBFs were tested to determine which function provided the minimal relative errors. For each of the 24 response surfaces, the best RBF was selected to construct the final response surface.
The regression parameter R 2, was used as an error indicator to gauge the accuracy of the RBF's generated response surfaces. When R2 calculated from the RBFs is sufficiently close to 1, the process of constructing the approximated model stops. Otherwise, new sample points are added to update the approximated model. In the current study, 31 sampling points produced sufficiently small errors and no additional points were added in the response surface constructions. Meanwhile, the relative error defined by the ratio between the absolute residual, which was defined as the difference between the FE model calculated value and the value computed by RBF-based response surface model, and FE model calculated value, was used to measure the goodness of fit for the response surfaces constructed.
Results
At the time of maximum indentation, typical MPS contours for both the flat and hemispherical impactors for the most commonly used CCI input scenario (impact depth: 2 mm, impact diameter: 5 mm) are shown in Figure 2. Most high MPS regions were located directly beneath the impact region. The high strain regions were also found to distribute along the flat impactor rim and near the center about the longitudinal axis of the hemispherical impactor. Table 1 summarizes the total volume in which the CSDM exceeded the pre-set 0.30 threshold and percentage of cell death predicted by CSDPM for both impactors under the most commonly used CCI inputs in the six ROI's. In general, the CSDM- and CSDPM-predicted injury responses were less in the hemispherical shape impactor group than in the flat impactor group under the same impact conditions.
Maximum principal (tensile) strain at coronal and sagittal sections for CCI cases using flat and hemispherical impactor. Regions with mesh indicate corpus callosum. Contours are shown with strains mapped to undeformed brain.
For all 24 RBF-based response surfaces, the regression parameters R2 were >0.99. Such R2 values indicated that the response surfaces were accurate to estimate the relationships between the parameters studied (impact depth and impactor diameter) and regional injury responses (CSDM and CSDPM). The average relative errors of the injury responses were very low at 2.44% (±2.04%) for CSDM and 1.72% (±1.94%) for CSDPM, with the maximum error of 5.56%.
Figures 3 and 4 show CSDM response surfaces constructed for the six ROI's for the flat and hemispherical impactors, respectively. The mesh lines in each response surface indicate the changes of responses along one parameter, whereas the second parameter was maintained constant. For example, the dark solid line in the top left figure of Figure 3 describes the changes of CSDM as a function of impact depth when the impactor diameter was fixed at 6.03 mm. Furthermore, 24 spreadsheets with macros were generated by modeFrontier based on these response surfaces. Any interested parties may contact the authors to obtain an electronic copy of such spreadsheets to calculate the corresponding CSDM and CSDPM for any CCI parameters they used.
CSDM showing relations between impact depth/impactor diameter and regional injury intensity for flat impactor group. CSDM, Cumulative strain damage measure.

CSDM showing relations between impact depth/impactor diameter and regional injury intensity for hemispherical impactor group. CSDM, Cumulative strain damage measure.
As an example of what information can be obtained from the numerical analysis, for a randomly defined CCI using a 4.31 mm diameter flat impactor and 1.67 mm impact depth, the CSDM 0.30 were 26.65 mm3 for ipsilateral cortex, 4.88 mm3 for ipsilateral corpus callosum, 1.44 mm3 for ipsilateral hippocampus, 0.00 mm3 for ipsilateral thalamus, 0.10 mm3 for cerebellum, and 0.00 mm3 for brainstem. Figures 3 and 4 also demonstrate significant differences in regional response variables. Under the same impact conditions, a much larger volume of the cortex experienced high strains compared to the small volume affected in the thalamus.
Increasing the impact depth increased the CSDM responses, although nonlinearly, for all six ROI's (Fig. 3). However, enlarging the impactor diameter increased the CSDM responses effectively in the cortex, cerebellum, and brainstem regions but not in the subcortical regions such as corpus callosum, hippocampus, and thalamus regions (Fig. 3). For the flat impactor group, a 5- mm diameter impactor induced more injuries in the corpus callosum, hippocampus, and thalamus than did larger diameter impactors (Fig. 5 A–C). On the other hand, an impactor with the smaller diameter seems to be prone to induce thalamus injuries (Fig. 5 C). The impactor diameter played a different role for the hemispherical impactor group, as CSDM responses generally increased along with impactor diameters, except that a local minimum occurred at around the 6 mm diameter impactor (Fig. 5 D–F).
CSDM response changes with impactor diameter at fixed impact depth. CSDM, Cumulative strain damage measure.
Varying regional injury intensity and nonlinear relationships among different impact parameters investigated were also observed for the CSDPM response surfaces at the six ROI's for the flat and hemispherical impactor group (Figs. 6 and 7). In general, the CSDPM-predicted responses increased as the impact depth or impactor diameter increased. Below an impact depth of 2 mm for the flat impactor group, quasi-plateau CSDPM-predicted responses were observed when the impactor diameter was ≥ 6 mm for the corpus callosum, hippocampus, and thalamus.

CSDPM showing relations between impact depth/impactor diameter and regional injury intensity for flat impactor group. CSDPM, Cumulative strain damage percentage measure.
CSDPM showing relations between impact depth/impactor diameter and regional injury intensity for hemispherical impactor group. CSDPM, Cumulative strain damage percentage measure.
Discussion
Twenty-four CSDM- and CSDPM-predicted response surfaces were generated from FE simulations of 70 commonly used CCI input scenarios using a validated rat brain model to systematically analyze strain-based injury severities at six ROI's. Several general predictions from these FE and response surface simulations were supported by experimental observations of injuries. The cortex experienced the largest volume of severe strains for all CCI cases simulated, whereas the affected volumes were much less in other regions. This finding matched the focal cortical contusions seen in all published CCI experiments. In general, the CSDM-predicted injured volumes and CSDPM-predicted percentages of cell death for all six brain regions increased as the impact depth increased, although at different degrees of nonlinearity. This prediction seemed to match experimental studies in which brain injury intensity (represented by cell loss, behavioral dysfunction) was increased with increasing impact depth (e.g., Baskaya et al., 2000; Davis et al., 2008; Igarashi et al., 2007; Scheff et al., 1997; Taylor et al., 2008). Under the same CCI inputs, the hemispherical impactor produced tissue strains to a lesser extent than did the flat impactor. Although no such experimental data were reported for the rat, the cell-loss pattern observed in a mouse CCI study displayed a similar trend (Carlson et al., 2009). Also, the flat impactor tended to induce strain concentrations near the impactor rim, which agreed with CCI experimental studies that a circular hemorrhage ring was reported using a flat impactor (Ueno et al., 1995) and that cortical damage was found along the impactor edge for moderate TBI (Sutton et al., 1993).
This study further yielded predictions that lead to several interesting findings regarding regional injury intensity and its relationship with impact parameters. One such finding was that an increase in impactor diameter did not necessarily increase tissue strains for brain regions beneath the cortex. For the flat impactor group, the 5-mm diameter impactor induced the most injuries in the hippocampus and corpus callosum regions. In addition, the 5-mm diameter impactor can induce more injuries in hippocampus than the 6 mm diameter impactor can for the hemispherical group. This finding may be indicative of one reason that a 5-mm diameter had been the most common in CCI experiments over the past 20 years. This study found that a smaller, flat impactor was preferred to induce injury in the thalamus region. This is echoed in an experimental study performed by Chen et al. (2003) in which neuronal damage in the thalamus was reported. The authors used a 2.5-mm diameter impactor with an impact depth of 2 mm at an impact velocity of 4 m/s for CCI input. The local minimum for subcortical damage using a 6-mm hemispherical diameter impactor remains to be further investigated. We suspect that such a local minimum could be caused by the combined effects of “flatness” and size of the impactor. Figure 8 shows hemispherical impactors with diameters from 4 to 9.5 mm together with a cross-section of the FE rat brain model. As the impactor diameter increases, the hemispherical impactor tends to become more flat (in theory, a hemispherical impactor with an infinite diameter would be a flat impactor). As we can see from Figure 5A–C, a larger flat impactor induced lower sub-cortical tissue strains in certain impact depths (2 mm for the corpus callosum and 3 mm for the thalamus). We speculated that a 6-mm diameter hemispherical impactor may be near the transition point where strain increase in the subcortical regions caused by the enlarged impactor diameter was smaller than the strain decrease caused by increased flatness for 2- or 3-mm impact depth. For the brainstem and cerebellum regions, the simulations predicted high CCI-induced tissue strains when combining a large impact depth and a large impactor, although the literature does not provide conclusive support. The simulations in the current study indicated that brain tissues were compressed toward the foramen magnum but there is no experimental data to prove this prediction. Because no experimental studies measured brain motions in the foramen magnum, new experiments are required to validate findings predicted in the current study.
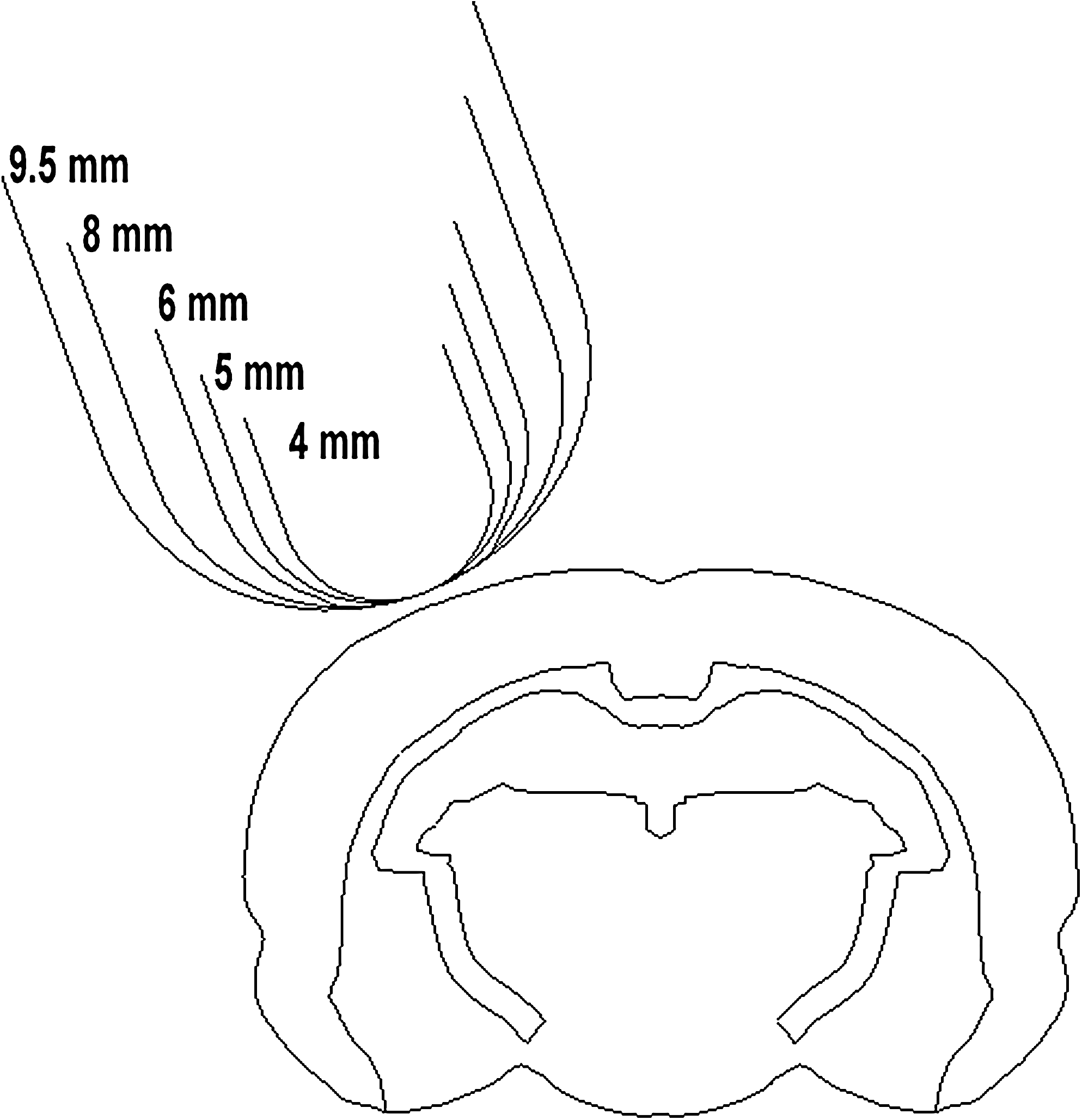
Hemispherical impactors of varying diameters and the finite element rat brain model at a coronal section through the impactor center. Increasing the impactor diameter accompanies an increase of flatness.
Different laboratories may define injury severities differently. Such variances, together with different CCI impact settings, make the comparison among different laboratories very difficult. One objective of this study is to describe clearly the settings for various CCI and the respective effects caused by these varying settings. The impact depth was found to be a leading factor affecting brain responses in CCI (Mao et al., 2010b). As such, the impact depth has been used by a number of researchers to indicate injury severity. However, even though the leading factor (impact depth) was fixed at 2 mm, the FE model predicted CSDM (0.30) varied greatly from 40.23 to 116.20 mm3 when other variables such as the impactor diameter, impactor shape, impact velocity, and craniotomy pattern were changed (Mao et al., 2010b). Intuitively, one can reasonably speculate that for the same 2-mm impact depth, CCI with 116.20 mm3 CSDM-predicted contusion will be much more severe than that with 40.23 mm3 CSDM-predicted contusion. Therefore, a single variable (such as the impact depth), or two variables, should not be used to describe injury severities. Instead, brain internal responses as quantified by CSDM or CSDPM are more appropriate in the definition of injury severity.
Traditionally, FE brain models have been used mainly to study injury tolerances and to develop countermeasures for protecting the brain. The current study presented a potential application of using FE brain models to design specific laboratory-induced injuries before an experiment is conducted. Using an FE rat brain model, effects of changing external impact parameters on brain internal tissue responses can be systematically studied without killing any animals. The RBF-generated response surfaces based on these FE simulations could be used by different laboratories to compare regional tissue responses for many kinds of CCI input scenarios so that histological results and other physiological parameters can be compared with analogous loading severity. If a research group is interested in matching a specific regional injury observed in patients to an animal model before devising a therapeutic trial, the best CCI parameters can be identified using FE modeling by maximizing tissue responses in the desired region while minimizing tissue strains elsewhere.
The current rat brain model represents an average adult rat brain and the brain materials used in current study were based on the study reported by Gefen et al. (2003). Variations of anthropometry, material property, and anatomy might affect predicted tissue strains. Increase in brain size (mature vs. average) will slightly decrease the magnitudes of predicted strains (Mao et al., 2010a, Table 1). Strain responses within the brain caused by CCI were not affected much by using uniformly scaled materials. The peak MPS in cortical tissues slightly decreased (<2%) even though five times stiffer brain tissues were assumed (Mao and Yang, 2011). The material heterogeneity between the gray and white matter was incorporated in the current rat brain model with properties of the white matter defined as 70% as stiff as those assumed for the gray matter. A stiffer corpus callosum (125% as stiff as the gray matter) tends to generate lower strains in the cortex (<1%) but higher strains in the hippocampus and thalamus (<4%) (Mao et al., 2010a). Material heterogeneity seems to have much greater effect on brain tissue strains than does material stiffness for CCI simulations. In the future, a much finer three dimensional rat brain model is needed to further investigate brain responses, such as incorporating newly reported hippocampus material heterogeneity data (Elkin et al., 2010). The changes of regional geometry in the brain when different types of transgenic animals were used will affect strain predictions as well, but the trends may vary in different loading scenarios. In this case, a morphing technique (Pleasant et al., 2011) will be beneficial to morph a brain model to match a specific transgenic animal brain, to accurately predict strain maps.
Brain injuries include those caused by the initial insults and subsequent cascade of biological events. Unfortunately, there are few valid noninvasive methods to assess site-specific brain injury at multiple time points, including axonal injury and contusion. As a result, it would be very costly to set up an experimental study aimed at determining what mechanically-induced injury occurs at which specific time point. Brain contusion could develop right after the initial impact if the tissue strains exceed that of the injury threshold. Mao et al. (2006) and Mao and Yang (2011) found a higher MPS threshold (30%) is needed to correlate the volume of long-term brain contusion (7–14 days post-injury) whereas a lower MPS (26.5%) can be used to predict the contusion volume measured at 24-h post-injury. Also, regions that showed signs of recovery were found to be located in the peripheral margins of the contusion where lower levels of tissue strains were presented when comparing FE-predicted strain maps and histological images. Therefore, it is achievable to correlate FE model predictions with time-dependent injuries provided that injury data at a large number of time points are available.
One critical limitation that needs to be resolved in future is the need to further study region- and cell-specific injury tolerances. The current study is based largely on simple correlations of contusion volume measured by Sutton et al. (1993), Kochanek et al. (2005), Scheff et al. (1997), and Chen et al. (2003), and neuronal cell death reported by Igarashi et al. (2007) with respect to FE model-predicted strains. Therefore, the response surface-predicted CSDM or CSDPM values in this study are only useful in analyzing the general trends. CSDM is derived based on correlating brain contusion volume with model-predicted MPS. On the other hand, CSDPM is derived from cell loss percentages, and it is better used to predict diffuse neuronal damage. Currently, CSDM is recommended for cortical lesions, whereas no regional preference was recommended for CSDPM. The brain is intricately constructed with different kinds of cells and axons, which are structured with all different orientations. Different cells/axons at various regions may respond differently to various mechanical loading modes such as tensile, compressive, or shear strain. One of the more elegant methods to study tissue level injury tolerance is to use in vitro tests, in which the mechanical loading is well controlled, to study the relationship between injuries and tissue stress/strain (e.g., Cater et al., 2006; Cullen et al., 2007; Elkin and Morrison, 2007; LaPlaca et al., 2005; Morrison et al., 2003). Obviously, in vitro studies do not totally reflect tissue responses of intact animals. Another method is to use a more detailed three-dimensional FE rat brain model, equipped with much more anatomic details than the current FE model, to compare FE model-predicted responses to histologically measured injuries. The advantage of this method is that the in vivo environment can be guaranteed, but a high-resolution high-biofidelity FE rat or mouse brain model is required, and the amount of histological work to measure various types of cellular and axonal injury would be enormous.
In summary, the current study systematically analyzed the relationship between CCI impact parameters and FE model-predicted tissue strains within six brain regions. This study presented an opportunity to apply the FE rat brain model to advance neurotrauma research, including strain-based descriptions of regional injury intensity and biomechanical explanations of variations among different laboratories conducting CCI research. In the future, the rodent brain regional strain responses during laboratory experiments could be compared to human brain tissue responses predicted by an FE human model under real-world injury scenarios. Such comparisons could assist in the design of improved methodologies to translate laboratory animal test results to human brain injuries with comparable tissue level biomechanical responses. The brain tissue strains predicted by the FE model could also be used to correlate with different injuries for studying cell/axon tolerances and vulnerability, which are important for neuroprotection and are potentially helpful for therapeutic intervention schemes as well.
Footnotes
Acknowledgment
We thank Christina D. Wagner for proofreading the manuscript. The development of the finite element rat brain model is financially supported by the Injury Control Research Center at the University of Alabama in Birmingham. The project is partially supported by the Bioengineering Center, Wayne State University, and State Key Laboratory of Advanced Design and Manufacturing for Vehicle Body of Hunan University. We thank LSTC for providing LS-Dyna and Esteco for providing modeFrontier. Financial support of Fengjiao Guan is provided by the China Scholarship Council.
Author Disclosure Statement
No competing financial interests exist.