
Abstract
More than 75% of patients with mild traumatic brain injury (MTBI) report chronic pain whose potential detrimental effects on cognitive recovery need to be identified. The objective of this study was to investigate the relationship between pain, performance on a working memory task, gray matter density, and mid-dorsolateral prefrontal cortex (mid-DLPFC) activation in subjects with a MTBI. For comparison purposes, we performed identical correlation analyses with a group of subjects without MTBI who sustained sports injuries. Twenty-four subjects who experienced a MTBI in the past 12 months, 16 control subjects, and 29 subjects with sport injuries were included. One hour prior to entering the magnetic resonance scanner, the subjects were asked to fill out the pain Visual Analogue Scale. Subsequently, a high-resolution T1-weighted image was acquired followed by a functional magnetic resonance imaging session using the visual externally ordered working memory task. Results showed that MTBI subjects reporting severe pain in the hour preceding the testing had reduced mid-DLPFC activation during the working memory task and poorer performance on the task. Subjects with sport injuries and severe levels of pain showed the reverse pattern: pain was associated with higher activation in the mid-DLPFC and did not correlate with performance. Gray matter density measures were independent of pain level. This study showed that behavioral performance and cerebral functioning are affected by pain after a MTBI. Moreover, this study suggests that pain, cognition, and cerebral functioning interactions could not easily be generalized from one clinical population to another.
Introduction
M
It is generally assumed that chronic pain impairs cognition 5 through two different mechanisms. First, pain may mobilize attention, thereby limiting the cognitive resources that would otherwise be allocated to a cognitive task. In support of this possibility, some studies have shown that the presence of pain more frequently impairs performance on challenging tasks. 6 –8 This effect, however, has not been reported in several other studies in which induced pain had no or only minimal detrimental effects on performance. 9 Second, neuroimaging studies have identified structural changes that could in part explain the impaired cognitive abilities reported in patients with chronic pain. These involve mostly decrease in gray matter density in dorsolateral prefrontal cortex (DLPFC), thalamus, brainstem, primary somatosensory cortex, and parietal cortex (see review 10 ), as well as decreased cortical thickness in DLPFC. 11
Our functional magnetic resonance imaging (fMRI) studies in subjects with MTBI have shown reductions in mid-DLPFC activation during the performance of working memory tasks that were mostly associated with post-concussive symptoms. 12 –14 However, the specific contribution of pain to these altered fMRI activation patterns after MTBI remains unknown.
Our primary objective was to investigate in subjects with MTBI the relationship between pain, performance on a working memory task, and the BOLD signal changes associated with it. We hypothesized that the MTBI population would show poorer performances and lower mid-DLPFC activation in the presence of more severe pain level. Another goal was to verify whether these correlations were specific to the MTBI population. To achieve this second objective, we performed identical correlation analyses with a group of athletes who did not suffer a MTBI (identified as “athletes” here) but who complained of various levels of pain due to minor orthopedic injuries. We surmized that, contrary to MTBI subjects, pain level would not be associated with poorer performance or reduced activation in mid-DLPFC in athletes since their cognitive resources would remain unaffected (i.e., non-MTBI). A third objective was to determine whether pain was associated with reduced gray matter density in subjects with MTBI. Our hypothesis was that decreased gray matter would be observed in association with pain as observed in previous studies.
Methods
Subjects
Twenty-four subjects (46% women; 27.4±10.6 years old) who sustained a MTBI in the past 12 months were included in the study (avg. time after MTBI, 3.7±3.8 months). Fourteen of the subjects were also included in a previous study. 14 All subjects were referred by physicians working at the McGill University Health Centre or at the Hôpital du Sacré-Coeur de Montréal, two tertiary trauma centers in the Montreal metropolitan area. Diagnosis of MTBI was made by a physician at the emergency room, and confirmed by a second physician expert in MTBI, according to the proposed definition and criteria, 15,16 which included a Glasgow Coma Scale (GCS) score between 13 and 15 approximately 30 min after the injury (i.e., admission to emergency room). In our study, most subjects had a GCS of 15, with two subjects having a GCS of 14 and two subjects having a GCS of 13. None of the subjects needed a neurosurgical intervention, none was involved in litigation, and brief loss of consciousness (<30 min) was documented in 55% of the cases. CT scans were performed in eight of 24 subjects at the emergency room and two subjects showed positive results, representing 8% of our sample. This proportion is consistent with previous studies. 17,18 The mechanisms of injury were recreational/sport injury (50%), motor vehicle accident/bicycle (25%), fall (20%), and accident at work (5%). Patients with MTBI were compared to a group of 16 healthy subjects matched for age and gender who never sustained MTBI (50% women, 32.6±9.6 years old). MTBI patients had an average of 2.3 years less education than control subjects (MTBI group, 14.0±2.4 years; control group, 16.3±3.1; t(37)=−2.6, p<0.05).
Twenty-nine athletes (all males, 20.2±1.7 years old) from university football, hockey, or soccer teams were also tested and acted as a second control group. None of them had sustained a concussion or a MTBI in the past. They were tested as control subjects for a previous study 12 and were not specifically matched for age, gender, or education to the MTBI subjects in the present study. They nonetheless constituted an interesting group to investigate, because they reported similar pain intensity to that observed in subjects with MTBI and were otherwise healthy. The pain reported by athletes during testing was due to mild orthopedic injuries sustained during play (i.e., knee, back, and shoulder pain) but their inclusion in this study did not depend on the presence of pain.
Exclusion criteria for all subjects included the presence or history of any diagnosed psychiatric or neurological condition, including depression, and the use of drugs known to affect cognition, including analgesics. No patient had specific pharmacological treatment for pain, except occasional use of acetaminophen or ibuprofen. Migraine diagnosed before the MTBI was also an exclusion criteria. Each participant was informed of the research protocol and gave written informed consent before the beginning of the study. The protocol was approved by the hospital ethics committee.
Questionnaires
One hour before entering the MRI scanner, the subjects filled out the following questionnaires: Visual Analogue Scale (VAS), 19 the Post Concussion Scale (PCS), 20 and the Beck Depression Inventory (BDI-II). 21 The VAS version used in this protocol consisted of a 100 mm line with ends labelled “no pain” to “worst possible pain.” Numbers from 0 to 10 along the scale provided guidance. The written instructions given to the subjects were: “Please circle the number that best describes the question being asked.” Four different questions were asked: (1) What is your pain right now?; (2) What is your typical or average pain?; (3) What is your pain level at its best?; (4) What is your pain level at its worst? Subjects were asked to use the past week as a reference point when answering the last three questions. Only questions 1 and 2 were used in our statistical analyses.
Working memory task
All subjects extensively practiced the visual externally ordered working memory task 22 in order to familiarize themselves with the set of images and the experimental procedure before undergoing the fMRI session. The task was used in our previous fMRI studies and has been described in details. 12,14,23 Briefly, on each trial, four images selected randomly from the same set of five images were presented successively at the center of the screen. The subject had to monitor which items appeared on each trial, because after a short delay following the sequential presentation of these items, one of the five stimuli was shown on a test trial and the subject had to decide whether or not the test item was among the four previously presented items. In the control condition, during the stimulus presentation phase, a single image was shown four consecutive times. After a delay, one of two images associated with either a left or a right mouse button click was presented and the subject had to choose the appropriate response.
Image acquisition
We used a 1.5 Tesla Siemens Sonata scanner (Siemens AG, Erlangen, Germany). All participants underwent a routine MRI examination as part of the functional scanning, including sagittal high resolution (1 mm3) T1-weighted 3D structural imaging (repetition time [TR]: 22 msec; echo time [TE]: 9.2 msec; flip angle [FA]: 30°), axial T2-weighted turbo spin echo imaging (TR: 3910 msec; TE: 81 msec; FA: 150°) and axial fluid-attenuated inversion recovery (FLAIR, TR: 9000 msec; TE: 66 msec; inversion time: 2500 msec; FA: 180°) sequencing. Structural MRIs were examined by an expert clinical neuroradiologist for signs of injury. Two functional runs lasting 6 min each were then acquired in a single session. Each functional run consisted of blocks of working memory and control conditions presented alternatively every eight trials (equivalent to 20 image acquisitions). In all, 120 image acquisitions were obtained in each run, with T2*-weighted, gradient-echo echo-planar imaging sequences (TR: 3000 msec; TE: 51 msec; FA: 90) and voxel size=2.3×2.3×7.0 mm. Twenty oblique slices (7 mm thick, −35° relative to the anterior commissure–posterior commissure line, interleaved signal order) were taken during each acquisition.
Image processing
Functional MRI
According to the neuroradiologist's evaluation, all structural MRIs (T1, T2, FLAIR) were normal, with no sign of injury. Images were first realigned to the third frame of the first run to correct for movement artefacts. Images were then smoothed with a MINC blurring software (mincblur) using a 6-mm full-width at half-maximum Gaussian filter to increase the signal-to-noise ratio of the data. Data were then analyzed using fmristat
24
(an in-house package available at
Voxel-based morphometry
Voxel-based morphometry was performed using the VBM8 toolbox (
Statistical analysis
To test main hypotheses
Our first objective was to understand the relationship between pain, performance on the working memory task, and BOLD signal change in MTBI subjects using fMRI. To achieve this goal, two methods were used: (1) Pearson's correlation co-efficients to measure relationships between two scores obtained on VAS (i.e., question 1: “pain right now” and question 2: “typical/average pain”), behavioral responses, and fMRI variables (BOLD signal changes in the left and right mid-DLPFC, BA 46, and 9/46, using regions of interests); and (2) multiple regression analyses with fmristat 24 as exploratory measures to analyze the relationship between cerebral BOLD signal change (without a priori hypothesis on the brain region involved) and pain scores on VAS in the MTBI group. These analyses were also performed in the group of athletes, but not in control subjects because of the lack of variability in the VAS scores in the latter group (all scores were 0 or 1).
For statistical analyses performed on fMRI data, for a single voxel in a directed search within predicted brain regions (i.e., mid-DLPFC, putamen, thalamus, and caudate nucleus), the threshold for significance (p<0.05) was set at t=4.1. For a single voxel in an exploratory search involving all peaks within an estimated gray matter of 600 cm3 covered by the slices, the threshold for reporting a peak as significant (p<0.05) was t=4.6. Finally, a cluster of voxels with a volume exceeding 487 mm3 with a t value > 3 was significant (p<0.05), corrected for multiple comparisons using a previously described method. 27 Region of interest (ROI) analysis consisted in the examination of the left and right mid-DLPFC (BA 9 and 9/46) involvement in the working memory task compared to the baseline control task, and the selection of these structures was based on our previous study. 12 For each subject, mean percentage of BOLD signal change was calculated in these regions within a 10-mm3 radius gray matter volume centered on the activation peaks in the ROI, as performed in previous studies of our group. 14,28
Our second main objective was to determine whether gray matter density correlated with the level of pain. We first verified whether MTBI subjects had reduced gray matter density in comparison to control subjects. Between-group local differences in gray matter density were measured with an analysis of co-variance with age as co-variable. We applied family-wise error correction for multiple comparisons at voxel level 29 and threshold for significance was set at p<0.05. To specifically assess the association between pain and gray matter density, correlation analyses between VAS scores (i.e., “pain right now” and “typical/average pain”) and gray matter density were done in MTBI subjects and athletes separately with age as co-variable. Again, the statistical threshold was set at p<0.05 after applying the family-wise error correction.
To test our secondary hypotheses
Group differences (MTBI vs. control group) on demographic (age and education) were tested with student t-tests. Group differences (all three groups) on questionnaires (PCS, BDI-II, and VAS) were tested with one-way ANOVA. Scores obtained on VAS were correlated with age and clinical variables (i.e., time post-injury, PCS total score, BDI-II total score) using Pearson's correlations. Group differences (MTBI vs. control group) on BOLD signal changes in the ROI of the mid-DLPFC were performed using Student t tests.
All statistical analyses were performed using fmristat (
Results
Symptoms
Table 1 shows results obtained with questionnaires. MTBI subjects reported significantly higher post-concussion symptom severity and depression symptoms than control group and athletes. Group differences were also found for pain as reported on VAS. First, all MTBI patients but none of the athletes reported headaches as the main source of pain. MTBI subjects and athletes had higher total scores on VAS than the control group, and no difference was observed between MTBI subjects and athletes on this score. No group differences were found between MTBI subjects and athletes for VAS questions 1 (“pain right now”) and 2 (“typical/average pain”), but they had significantly higher scores in comparison with control subjects. Correlation between VAS scores (“pain right now” and “typical/average pain”) and subject characteristics (age, education, delay since TBI, PCS total score, and BDI-II total score) were performed only in the MTBI and athlete groups, because the control subjects' scores of 0 or 1 out of 10 on the VAS lacked variability. A significant correlation between “typical/average pain” and BDI-II total score was found for the MTBI group (r=0.45, p<0.05) where patients reporting more severe pain had more depression symptoms. No correlation between pain and depression was found for athletes. No other correlations were observed between pain and demographic or clinical variables.
Data available for 19 of 29 subjects only.
Values are given as mean±standard deviation. ns, not significant.
Behavioral performance
No group differences were found for the behavioral results (Table 2). Figure 1 shows the correlation between pain and accuracy for MTBI subjects and athletes. “Pain right now” and “typical/average pain” were both significantly correlated with accuracy on the working memory task in the MTBI group: subjects with higher pain were less accurate (see Fig. 1 for r and p values). When BDI total score was added as a co-variable (partial correlation), no change was found in the results for “pain right now” (r=−0.57, p<0.01), but the results for “typical/average pain” (r=−0.44, p=0.053) varied. Thus, depression symptoms appeared to influence the correlation between “typical/average pain” and behavioral performance but not the association between “pain right now” and accuracy on the working memory task. No correlations were found between pain and performance on the control task. Contrary to that seen in MTBI subjects, no correlation was found between scores reported on the VAS and reaction times or accuracy on the working memory or the control tasks in athletes.
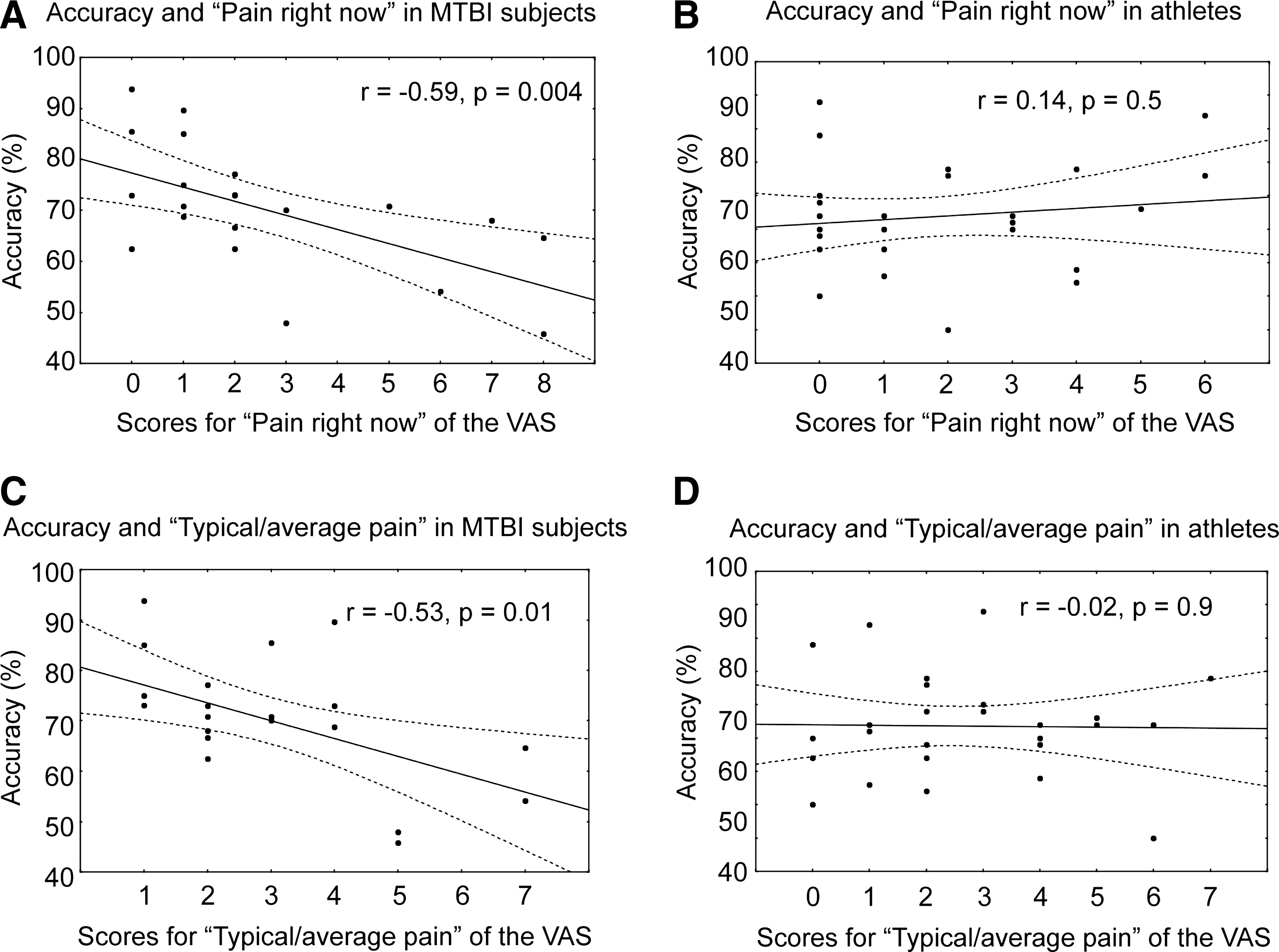
Correlations between accuracy for the working memory task and pain reported by MTBI subjects and athletes. Correlations between accuracy on the working memory task and “pain right now” for MTBI subjects (
Values are given as mean±standard deviations. ns, not significant; na, not applicable.
Functional MRI activations and deactivations observed in all groups
As observed in our previous studies, 12,14 significant activations were predominantly found in the left and right mid-DLPFC (BA 46 and 9/46), the precuneus and the superior parietal lobule (BA 7), the thalamus, the body of the caudate nucleus, and the putamen. Negative peaks or deactivations were also found in both groups in the medial orbito-frontal, the rostral anterior cingulate, and the posterior cingulate cortex. When groups were compared on BOLD signal change in mid-DLPFC using ROI analysis, a trend was found for lower activation in the left mid-DLPFC in the MTBI group in comparison with the control group (t(38)=−1.96, p=0.058).
Association between pain and BOLD signal changes in MTBI subjects
Correlation analyses were first performed between pain reported on VAS and BOLD signal changes obtained from the working memory task minus the control task in MTBI subjects. Using ROI, we found a significant correlation between BOLD signal change in the right mid-DLPFC (BA 46) and VAS (i.e., “pain right now” and “typical/average pain”), where a higher level of pain was associated with lower BOLD signal changes (see Table 3 for summary of results and detailed statistical r and p values). When BDI-II scores were added as a co-variable (partial correlation), no changes were found in the results for “pain right now” (r=−0.50, p=0.02) or for “typical/average pain” (r=−0.52, p=0.01). No correlations were found between BDI-II scores or PCS scores and BOLD signal change in the mid-DLPFC.
p<0.05, † p<0.01.
VAS, Visual Analogue Scale; BA, Brodmann area.
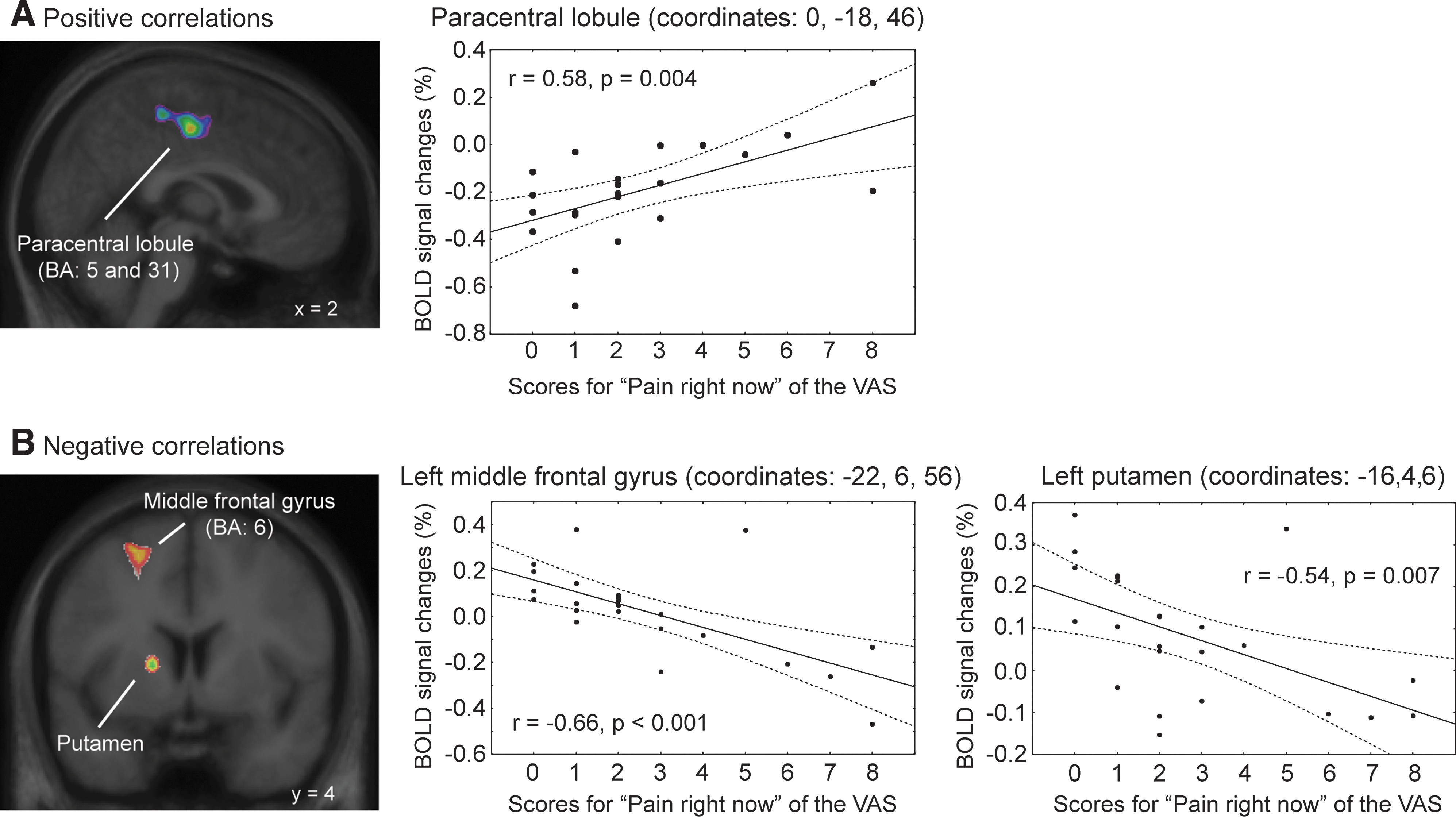
Voxel-wise whole-brain regression analyses were performed in order to verify whether BOLD signal changes were associated with pain, without an a priori hypothesis on the brain regions involved. Table 4 presents the cerebral regions where BOLD signal changes were significantly associated with “pain right now” and “typical/average pain.” Significant correlations include “pain right now” and BOLD signal changes in the medial paracentral lobules and the right postcentral gyrus where higher pain was associated with higher activation or lower deactivation (Fig. 2). “Pain right now” was also negatively correlated with activation in the left middle frontal gyrus, the left precentral gyrus, and the left and the right putamen: higher level of pain was associated with lower activation.
Regression analysis results for BOLD signal changes and scores for “pain right now” of the MTBI group. (
Significant with cluster analysis; p<0.05 (corrected).
BA, Brodmann areas.
In summary, in MTBI subjects, more severe “pain right now” measured with the VAS was associated with lower activations in the middle frontal gyri and the left and right putamen. More severe “pain right now” was associated with reduced deactivations in the posterior cingulate and the right parietal cortex.
Association between pain and BOLD signal changes in athletes
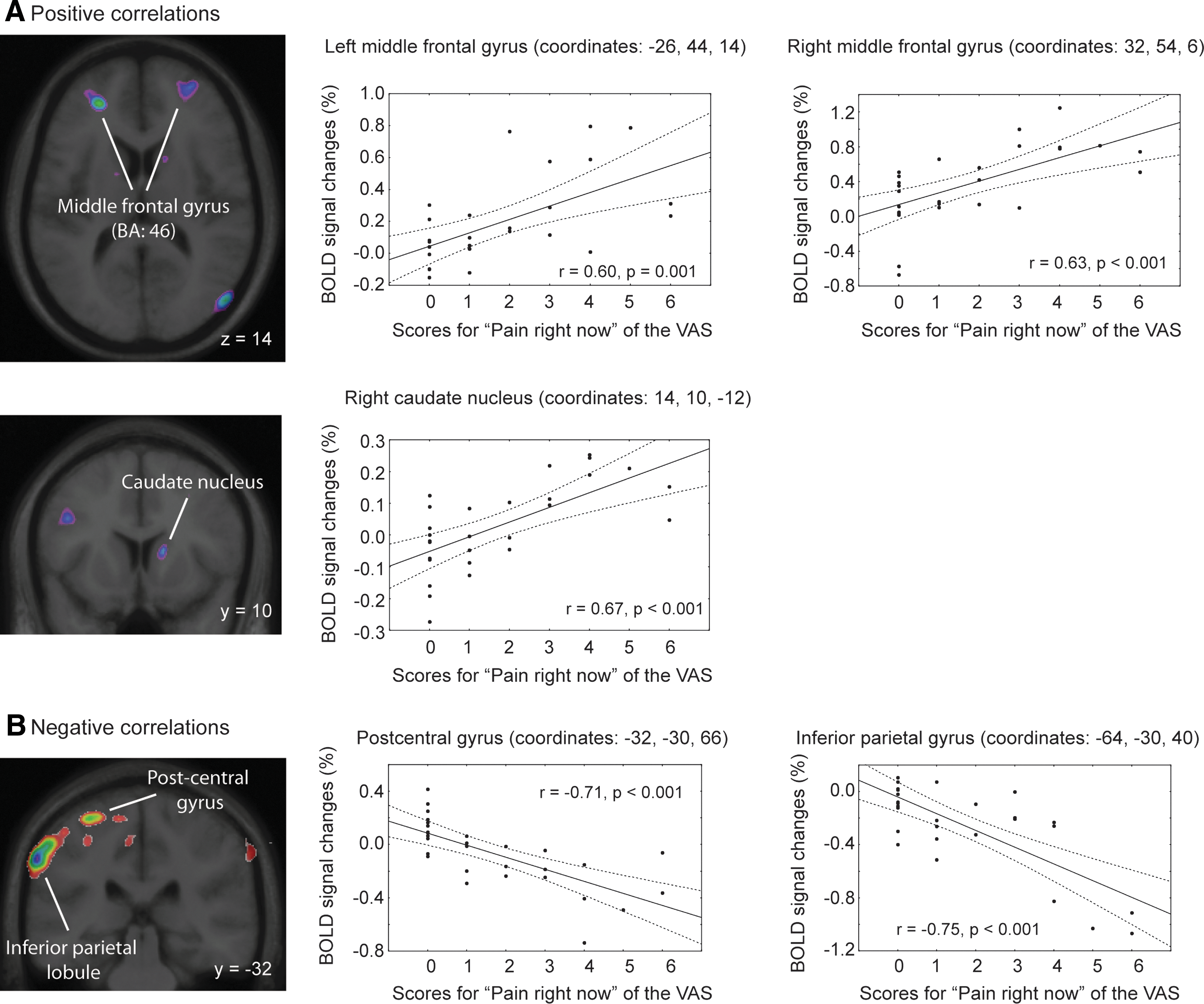
In athletes, the reverse result was observed: positive correlations were found between “pain right now” and BOLD signal changes in the left and right mid-DLPFC: the higher the pain, the higher the activation. However, no significant correlations were observed between “typical/average pain” and the BOLD signal change in the mid-DLPFC.
Regression analyses performed in athletes (Table 5) showed a positive association between “pain right now” and activation in the left and right mid-DLPFC, the right caudate nucleus, and the right middle temporal gyrus (Fig. 3): the higher the pain, the higher the activation. Finally, a significant association was found between “typical/average pain” and BOLD signal changes for the left superior and the middle frontal gyri where positive correlations were found.
Regression analysis results for BOLD signal changes and “pain right now” of athletes. (
Significant with cluster analysis; p<0.05 (corrected).
BA, Brodmann areas.
In summary, athletes showed the opposite results when compared to MTBI subjects. In fact, more severe pain was associated with higher activations in the mid-DLPFC, the right caudate nucleus, and the temporal lobe.
Gray matter density
No group differences were found between MTBI and control subjects for gray matter density. However, 14 MTBI subjects were in a relatively acute stage after their MTBI (<2 months); this short time span may be insufficient to allow visualization of structural changes in the brain. We therefore excluded these 14 subjects and analyzed the results of the remaining 11 MTBI subjects in a post-acute MTBI stage. The 11 MTBI subjects were compared to the group of 16 control subjects and, again, no group difference was found for gray matter density.
Using regression analyses, no significant associations were found in MTBI subjects between “pain right now” or “typical/average pain” and gray matter density. No significant correlations were found for athletes for VAS scores and gray matter density.
Discussion
The main finding of this study was the association between pain reported at the time of testing and lower fMRI activation in mid-DLPFC in MTBI subjects. Those subjects reporting higher pain in the hour preceding testing showed reduced mid-DLPFC activation when performing the working memory task. The presence of pain was also associated with poorer performance on the working memory task, but not on the less demanding control task. Athletes presenting various levels of pain due to minor sport injuries showed the reverse pattern: pain was associated with higher activation in the mid-DLPFC during the working memory task. Moreover, contrary to MTBI patients, pain was not associated with poorer behavioral performance. Taken together, these results suggest that pain is associated with changes in cerebral functioning and behavioral performance in a cognitive task, but these associations were influenced by other factors that are probably related to the nature of the pain (i.e., headaches vs. orthopedic injuries) and/or neurological condition, such as MTBI. These results have important implications for future studies aimed at understanding the effects of pain on cerebral functioning for MTBI and other clinical neurological and non-neurological conditions. This study showed that pain, cognition, and cerebral functioning interactions could not easily be generalized from one clinical population to another.
Impact of pain on cerebral functioning
A few studies have used fMRI during the performance of cognitive tasks to look at the effect of pain on cerebral functioning. Bingel and colleagues 7 reported that induced pain in healthy subjects increased reaction times during a working memory task, but had no effect on working memory–related cerebral activity identified with fMRI. Conversely, patients with chronic low back pain had reduced DLPFC deactivation during a working memory task despite a normal performance on the task; the abnormal deactivation returned to normal values after pain relief. 11 These fMRI results suggest that pain characteristics (acute vs. chronic and induced vs. endogenous) need to be taken into account since they may affect cerebral functioning differentially.
To our knowledge, our study was the first to demonstrate an association between endogenous pain and BOLD signal change in neurological and non-neurological populations. Our results showed that in MTBI subjects, “pain right now” was associated with lower activation in the right mid-DLPFC and the putamen. This association was not observed in athletes; this group showed increased mid-DLPFC and caudate nucleus activation in the presence of pain. This difference between our groups may be explained by the amount of cognitive resources available to each group. In athletes, pain associated with orthopedic injuries partially mobilizes the subject's cognitive resources such that optimal performance on the working memory task requires more effort than usual, which in turn entails increased mid-DLPFC and striatum activation. In contrast, in MTBI subjects who report pain linked to headaches, there is a need to increase cognitive effort and/or cerebral activation to carry out the task. This increase is likely impeded by the brain injury leading to a decrease in activation in the normally activated regions (i.e., mid-DLPFC and striatum) and less accuracy on the task.
Deactivation patterns and pain modulation
Less deactivation in the cingulate cortex was associated with higher pain in MTBI subjects, but not in athletes. During cognitive tasks, the deactivation pattern corresponds to the default-mode network that is generally observed in passive or non-demanding cognitive conditions. 30 A lower deactivation was previously reported in patients with chronic back pain in a study measuring the default-mode network dynamics. 31 The association of pain with lower deactivation probably represents a lack of passive condition, or less demanding condition, in patients with pain due to the constant cognitive resources allocated to pain. In our study, this lower deactivation pattern associated with pain was not found in athletes. The mid-DLPFC probably has a crucial role in pain modulation by inhibiting pain or keeping pain out of mind. 32,33 In agreement with this hypothesis, we observed increased activation in the mid-DLPFC in athletes who reported higher pain level before entering the scanner. The possible inhibition of pain by the mid-DLPFC in athletes may have led to both increased deactivation in regions associated with the default-mode network and to an absence of the detrimental effects of pain on performance in the working memory task. The hypothesis that the mid-DLPFC may play a role in deactivation patterns has already been put forward in subjects with chronic pain, 31 but needs to be tested in future studies.
Absence of structural changes associated with pain in post-acute MTBI
Many studies have reported atrophy or reduced gray matter density using VBM in clinical populations with chronic pain (see recent studies 11,34,35 ). No study has specifically investigated the MTBI population, but recently, loss of gray matter was observed in the DLPFC in patients reporting headaches 3 months after whiplash injury. 36 In the current study, no loss of gray matter was observed in the MTBI patients and “pain right now” or “typical/average pain” was not associated with lower gray matter density. Since our measures of pain were not performed in the chronic stage, this may explain the absence of an association between pain and loss of gray matter density. In fact, 41.6% of patients were tested within 2 months of their TBI and 58.4% were tested in the post-acute stage (i.e., 2–10 months post-injury). The extent of this delay was possibly not sufficient to detect changes in gray matter density.
Pain and depression
Several studies have shown that chronic pain is associated with depression symptoms in 30 to 50% of the cases. 37,38 This co-occurrence of pain and depression was also found in our study. Despite the fact that we did not measure pain in a chronic stage, we found an association between “typical/average pain” and BDI-II total score: MTBI subjects with higher pain had more severe depression symptoms. However, MTBI subjects with depression symptoms did not report higher “pain right now.” In the same manner, our results showed that depression symptoms influenced the correlation between “typical/average pain” and behavioral performance, but not the association between “pain right now” and performance on the working memory task in the MTBI group. Our results suggest that in MTBI subjects, the persistent or constant aspect of pain is associated more with depression symptoms and worse performance than with acute, transitory pain. The cause-effect relationship between pain and depression after MTBI needs to be investigated, but according to recent studies performed in non-MTBI patients, bidirectional and causative influence of pain and depression on one another is probable. 39,40
Correlations between pain, depression, and performance on the working memory task were not observed in athletes. More specifically, in this group of subjects reporting on average the same level of pain intensity as MTBI subjects, pain did not co-occur with depression.
Limitations
This study was performed within a larger research program that aims at understanding the effects of MTBI on brain functions. There are therefore several limitations to the present study: (1) Pain was assessed in a global manner without considering pain type (i.e., headaches vs. orthopaedic) and pain duration. The contribution of these factors to brain activation and deactivation patterns as well as to the etiology of depression symptoms needs further investigation; (2) Athletes without MTBI presenting different levels of pain were not matched with the MTBI subjects for age and gender. Nevertheless, the inclusion of athletes in order to compare pain and brain function associations lead to interesting results that will likely trigger further studies; (3) Other factors that may have mediated the association between pain and cerebral activation, such as disrupted sleep, 41 will need to be further investigated in studies with larger samples and with objective measures of sleep; (4) Finally, questionnaires evaluating specific aspects of pain could furnish interesting information in future studies.
Conclusion
This study showed that pain reported at the time of testing was associated with significant changes in cerebral activation in the form of activation and deactivation patterns during a cognitive task. Importantly, the type of population tested influenced these changes on brain functioning. This study suggests that neurological condition possibly plays a major role in the way pain affects cerebral activation during a cognitive task. This study also highlights the need to investigate the effects of pain on cognitive and cerebral functioning in different clinical populations reporting pain in order to understand its contribution to cognitive complaints.
Footnotes
Acknowledgments
This study was supported by the Canadian Institutes of Health Research (grants to A.P. and M.P. and fellowships to N.G. and C.B.) and by the Fonds pour la Recherche en Santé du Québec (fellowships to N.G. and J.K.C.). The authors are grateful to Dr. Diane Diorio, Mitra Feyz, Isabel Roy, and Cindy Hovington for their help with subject recruitment and/or technical support. We would also like to thank the staff of the Magnetic Resonance Imaging Unit of the McConnell Brain Imaging Centre, Montreal, Quebec, Canada for their assistance.
Author Disclosure Statement
No competing financial interests exist.